Page 1 of 8
AS1.1-4 | Evolution, Scope, Ethics and Career Pathways in Anaesthesiology — SDL Guide
References
CLINICAL SCENARIO
On 16 October 1846, in the Ether Dome of Massachusetts General Hospital, a dentist named William Morton administered diethyl ether to a patient while surgeon John Collins Warren painlessly removed a neck tumour. Warren turned to the assembled students and declared: "Gentlemen, this is no humbug." That single event transformed surgery from an act of agonised endurance into a humane and precise discipline — and in doing so, created the medical specialty of Anaesthesiology. As a Phase III medical student preparing to enter clinical practice, you will work alongside anaesthesiologists every day in the operating theatre, intensive care unit, labour ward, and pain clinic. Understanding who they are, what they do, and why their ethical commitments matter is foundational to effective teamwork and patient safety.
WHY THIS MATTERS
Anaesthesiology is one of the broadest and most safety-critical specialties in modern medicine. The anaesthesiologist is simultaneously a pharmacologist, physiologist, intensivist, pain physician, and resuscitation expert. For you as a future clinician — whether you pursue surgery, obstetrics, general medicine, or anaesthesia itself — knowing the scope, ethical framework, and career landscape of this specialty equips you to: (1) communicate effectively with anaesthetic colleagues during pre-operative planning; (2) understand consent obligations specific to anaesthesia; (3) recognise which anaesthetic subspecialty to involve in complex patient scenarios; and (4) make an informed career choice if you are considering postgraduate training in anaesthesiology or an allied field. (References: Morgan & Mikhail's Clinical Anesthesiology, 7th ed.; Ajay Yadav's Short Textbook of Anaesthesia, 7th ed.; Paul Barash's Clinical Anesthesia, 8th ed.; NMC Competency-Based Medical Education Curriculum 2024.)
RECALL
Before we explore the evolution and scope of Anaesthesiology, briefly recall: (1) What is the role of the autonomic nervous system in haemodynamic stability during surgical stress? (2) What is the difference between analgesia, sedation, and general anaesthesia as physiological states? (3) Name two ethical principles you have studied in the Foundation Course that guide clinical decision-making. These prior concepts will anchor your understanding of how anaesthetic agents work and why informed consent in anaesthesia demands special attention.
Orientation: What is Anaesthesiology and Why Does It Matter?
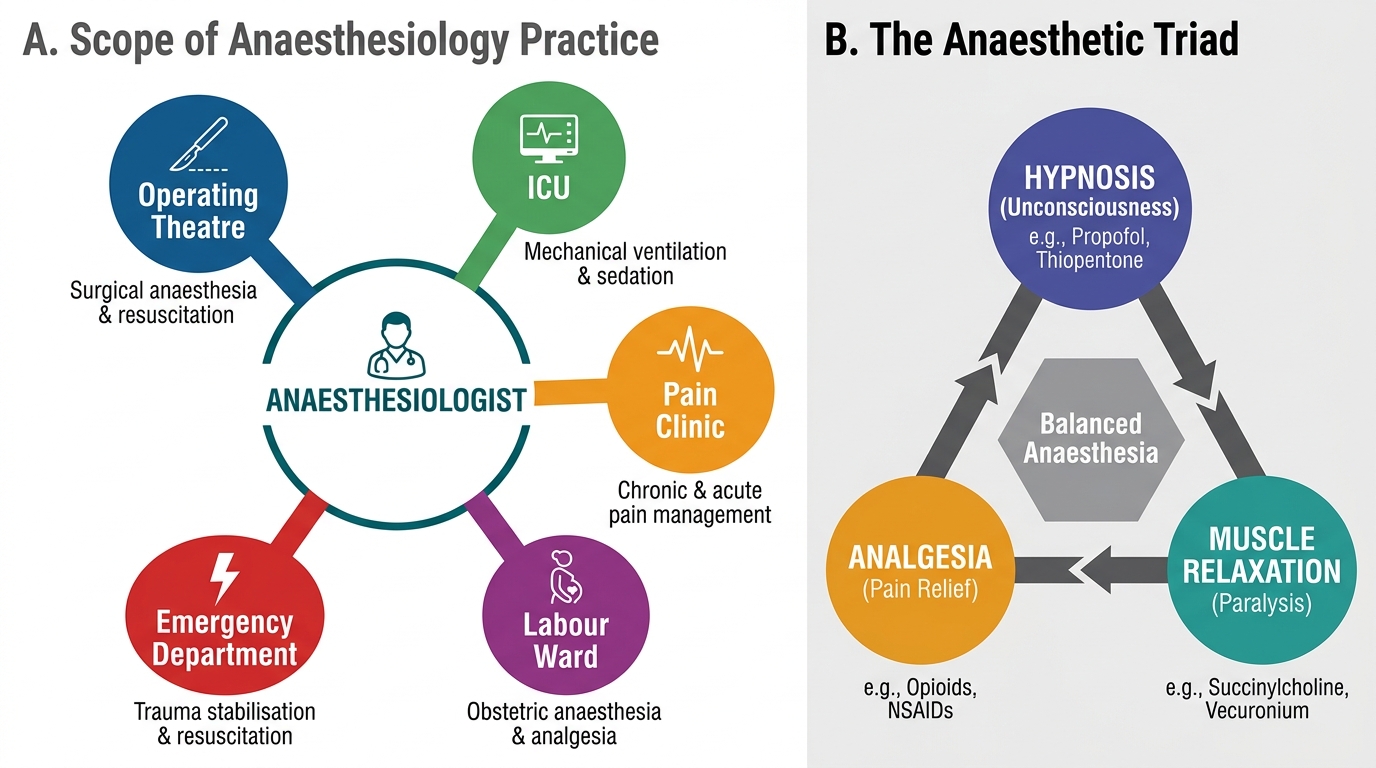
Anaesthesiology is the medical specialty concerned with the total care of the patient before, during, and after surgical, obstetric, or investigative procedures, as well as the management of acute and chronic pain and the resuscitation of the critically ill. The word derives from the Greek an- (without) and aisthesis (sensation), yet the modern specialty encompasses far more than the abolition of sensation. The anaesthesiologist must maintain the patient's physiological homeostasis — cardiovascular stability, respiratory adequacy, fluid and electrolyte balance, temperature regulation, and coagulation — throughout a period of profound pharmacological intervention and surgical stress that the patient could not survive without expert support.
The clinical relevance of this orientation cannot be overstated. Surgical procedures account for a substantial proportion of all hospital activity, and every such procedure requires anaesthetic care. According to estimates cited in Morgan & Mikhail's Clinical Anesthesiology, more than 300 million surgical procedures are performed worldwide annually, and anaesthetic complications remain a leading cause of preventable perioperative mortality. In India, the National Medical Commission (NMC) 2024 curriculum recognises anaesthesiology as a Phase III specialty taught in the final clinical year because its concepts — airway management, shock, resuscitation, pain — cut across every branch of medicine. The anaesthesiologist is therefore not a peripheral figure who merely "puts the patient to sleep"; rather, as Ajay Yadav's Short Textbook of Anaesthesia emphasises, the specialty constitutes the backbone of surgical and critical care infrastructure in any modern hospital.
Scope of Anaesthesiology and the Anaesthetic Triad
Key orientating facts about Anaesthesiology:
- It is both a clinical and a procedural specialty — requiring diagnostic reasoning AND manual skill
- The NMC 2024 curriculum assigns competency codes AS1–AS14 spanning specialty orientation, pharmacology, airway management, regional anaesthesia, monitoring, intensive care, pain, and resuscitation
- The specialty operates under the three pillars of the anaesthetic triad: unconsciousness (hypnosis), analgesia, and muscle relaxation — each requiring separate pharmacological management
- In India, the National Board of Examinations awards the DNB (Anaesthesiology) as the primary postgraduate qualification; MD Anaesthesiology is awarded by university-affiliated medical colleges
Evolution of Anaesthesiology: From Surgical Nightmare to Modern Specialty
The history of Anaesthesiology is one of the most dramatic transformation stories in medicine, spanning less than two centuries from primitive intoxication to precisely controlled pharmacological science. Understanding this evolution is essential not merely as historical trivia but because each milestone represents a solved problem — a physiological or pharmacological challenge that clinicians identified, studied, and resolved — and that intellectual tradition continues today in the form of ongoing patient-safety research.
The pre-anaesthetic era (before 1846) was characterised by speed and brutality. Surgeons were valued for their rapidity; the legendary Scottish surgeon Robert Liston could amputate a limb in under two minutes. Patients were restrained or rendered insensible by alcohol, opium, or hypnosis — none reliably sufficient. The suffering was immense, and many patients died from shock or sepsis, limiting surgery to the most desperate life-threatening conditions.
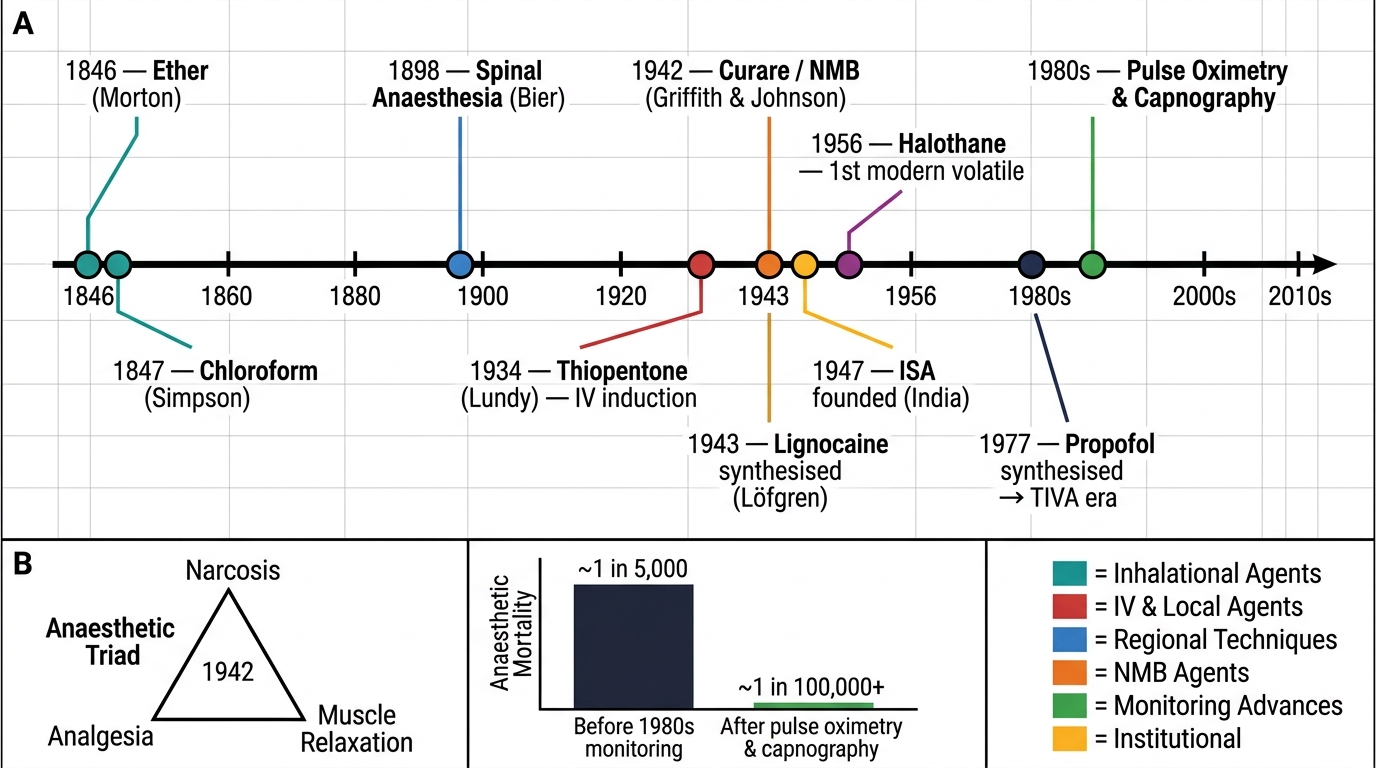
The ether milestone (1846) was the turning point. Crawford Long had used ether for minor procedures privately since 1842, but Morton's public demonstration on 16 October 1846 — the date now celebrated internationally as World Anaesthesia Day — established that safe, reproducible surgical anaesthesia was possible. Chloroform followed rapidly in 1847, introduced by James Young Simpson, who famously administered it to Queen Victoria during the birth of Prince Leopold in 1853, conferring royal legitimacy on anaesthesia.
Evolution of Anaesthesiology: Key Milestones 1846–Present
Key evolutionary milestones in Anaesthesiology:
- 1898 — August Bier performs the first spinal anaesthesia using cocaine; regional techniques expand the scope of surgery without general anaesthesia
- 1934 — thiopentone (thiopental) introduced by John Lundy; intravenous induction replaces inhalational induction as the clinical standard
- 1942 — Harold Griffith and Enid Johnson use curare (tubocurarine) for muscle relaxation; the anaesthetic triad concept formalised (narcosis + analgesia + relaxation)
- 1943 — lignocaine (lidocaine) synthesised by Nils Löfgren; becomes the prototype local anaesthetic for comparison
- 1956 — halothane introduced as the first modern volatile anaesthetic; safer than chloroform and ether; replaced by isoflurane, sevoflurane, and desflurane over subsequent decades
- 1977 — propofol synthesised; by the 1980s–90s it becomes the dominant induction agent and the backbone of total intravenous anaesthesia (TIVA)
- 1980s — pulse oximetry and capnography introduced into routine monitoring; anaesthetic mortality drops from ~1 in 5,000 to ~1 in 100,000 or better
- In India — the Indian Society of Anaesthesiologists (ISA) was founded in 1947, the same year of Independence, reflecting the importance placed on the specialty from the outset; Indian anaesthesiologists have since contributed to landmark research in spinal anaesthesia for obstetrics and regional blocks in resource-limited settings
The trajectory of the specialty mirrors the maturation of clinical pharmacology, monitoring technology, and patient-safety science. Each generation of anaesthesiologists solved the most pressing mortality problem of its era — from respiratory depression to awareness under anaesthesia to perioperative cardiac events — and this commitment to measurable safety outcomes remains the specialty's defining intellectual character.
Roles of the Anaesthesiologist: A Multi-Domain Specialty
The NMC competency AS1.2 requires you to describe the roles of the anaesthesiologist across multiple clinical domains. This is a particularly important competency because medical students — and even some clinicians — commonly underestimate the scope of the specialty, perceiving the anaesthesiologist solely as an intraoperative technician. The reality is strikingly broader: the modern anaesthesiologist is better described as a peri-operative physician whose clinical responsibility spans the continuum from the pre-admission clinic to the post-anaesthesia care unit, and extends well beyond the operating complex into the intensive care unit, labour ward, chronic pain clinic, and emergency resuscitation team.
Each role domain represents a distinct body of knowledge and a distinct set of procedural and cognitive skills. You will encounter anaesthesiologists in each of these settings during your clinical postings, and understanding their function in each context will make you a more effective team member and a safer doctor.
Five Role Domains of the Modern Anaesthesiologist
The five major role domains and their defining responsibilities are:
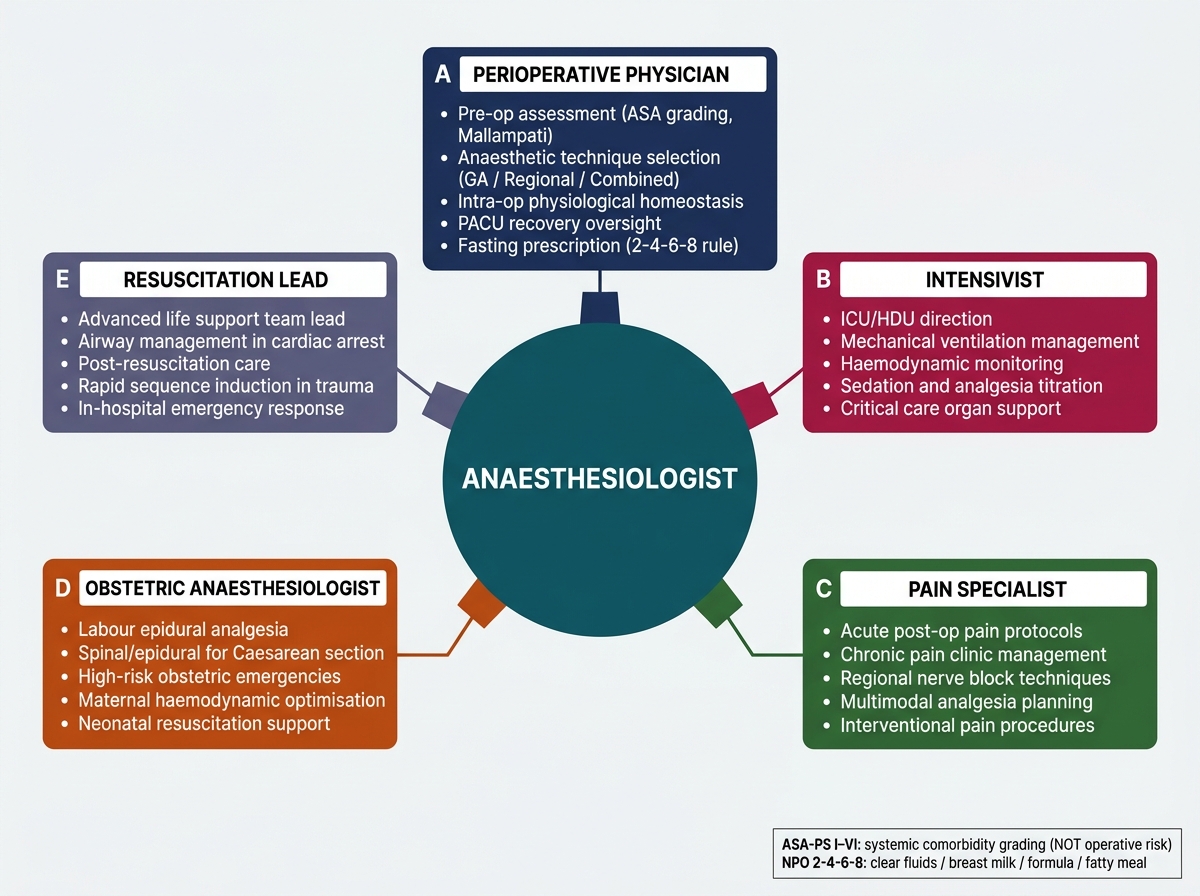
1. Peri-operative Physician (Surgical Anaesthesia)
This is the most visible and historically primary role. The anaesthesiologist conducts pre-operative assessment (medical history, examination, risk stratification using the ASA Physical Status Classification System, airway assessment including Mallampati grading), selects and administers the anaesthetic technique (general, regional, or combined), maintains the patient's physiological homeostasis intra-operatively, and oversees recovery in the Post-Anaesthesia Care Unit (PACU). Critically, the ASA Physical Status grades the patient's systemic comorbidity (I = healthy, VI = brain-dead donor) and is NOT a measure of operative risk or anaesthetic difficulty — a common source of confusion. Pre-operative fasting (the ASA "2-4-6-8" rule: clear fluids 2 h, breast milk 4 h, formula 6 h, fatty meal 8 h) is the anaesthesiologist's domain to prescribe and verify.
2. Intensivist (Intensive Care Unit and High Dependency Unit)
Anaesthesiologists are among the most common specialists directing Intensive Care Units (ICUs) globally, because their training in airway management, mechanical ventilation, haemodynamic monitoring, pharmacological sedation/analgesia, and resuscitation maps directly onto the skills required for critically ill care. In India, many government hospitals designate the anaesthesia department as the administrative home of the ICU. HDUs (High Dependency Units) provide an intermediate level of care for patients requiring close monitoring but not full ICU interventions.
3. Acute and Chronic Pain Specialist
Pain management is a rapidly growing subspecialty. Acute pain services manage post-operative pain (epidural infusions, patient-controlled analgesia, peripheral nerve blocks) to reduce opioid consumption and facilitate early rehabilitation. Chronic pain clinics address conditions such as neuropathic pain, complex regional pain syndrome, cancer pain, low-back pain, and headache syndromes — using pharmacological, interventional (nerve blocks, spinal cord stimulation), and multidisciplinary approaches. Labour analgesia (most commonly epidural analgesia in the second stage of labour) is a high-volume, high-impact service that significantly reduces maternal suffering without adversely affecting foetal outcomes when managed correctly.
4. Obstetric Anaesthesiologist
Obstetric anaesthesia requires specialist knowledge because the parturient represents two patients simultaneously. General anaesthesia in pregnancy carries an elevated risk of pulmonary aspiration (Mendelson's syndrome) and difficult airway; regional techniques are therefore strongly preferred. The anaesthesiologist must understand uteroplacental physiology, the effects of anaesthetic agents on the foetus and neonate, and emergency management of obstetric crises (massive haemorrhage, eclampsia, amniotic fluid embolism).
5. Resuscitation Lead
Anaesthesiologists are uniquely positioned to lead resuscitation of the acutely ill. Their familiarity with airway management (including rapid sequence intubation), vasoactive drugs, defibrillation, and circulatory support makes them natural leaders of in-hospital cardiac arrest teams. Adult Basic Life Support — chest compressions at 100–120/min, depth 5–6 cm, ratio 30:2, defibrillation for shockable rhythms (VF/pulseless VT) only, NOT for asystole or PEA — is a core competency explicitly defined within the AS curriculum.