Page 1 of 11
AS10.1-2 | Positioning Hazards and Perioperative Hazard Prevention — SDL Guide
CLINICAL SCENARIO
A 62-year-old man is placed in the lateral decubitus position for a left thoracotomy lasting four hours. When he is turned supine at the end of surgery, the anaesthesiologist notices that his right arm — which had been positioned on a padded arm-board — is weak, and he is unable to extend his wrist. The positioning-related brachial plexus stretch injury became apparent only after the drapes came down. For every hour a patient lies immobile on an operating table, the cumulative risk of pressure injury, nerve compression, vascular compromise, and vision loss silently rises. Anaesthesiologists and surgeons share the legal and professional responsibility for patient positioning — yet the harm is often attributed to causes other than the position itself because the injury declares itself after the patient wakes.
WHY THIS MATTERS
Positioning injuries are among the most preventable complications in perioperative care. The Indian Medical Council (Professional Conduct, Etiquette and Ethics) regulations and NMC GMER 2023 require that every practitioner minimise patient harm — which includes the hazards introduced by surgical positioning, equipment use, drug administration, and communication failures. AS10.1 and AS10.2 are Knowledge + Skills (KH) competencies that together form the foundation of patient safety practice in the operating theatre. Understanding these hazards is also a prerequisite for taking an informed consent, because the patient must be warned of position-related risks such as nerve injury and pressure sores. Finally, familiarity with perioperative hazards underpins the WHO Surgical Safety Checklist — now mandated in all accredited hospitals — which your team will run before every case.
RECALL
Before working through positioning hazards and their prevention, recall the following:
- Anatomy of vulnerable nerves: the brachial plexus (roots C5-T1) crosses the first rib and runs under the clavicle; the ulnar nerve is most exposed at the medial epicondyle; the common peroneal nerve wraps around the fibular head; the facial nerve exits the stylomastoid foramen.
- Pressure injury physiology: tissue ischaemia begins when capillary occlusion pressure (~32 mmHg) is exceeded, causing cellular hypoxia within 1–2 hours if unrelieved.
- Principles of blood flow: venous return depends on gravity — placing the operative site above the heart aids surgical exposure but impairs cerebral and venous pressure relationships.
- The ASA physical-status scale (I–VI): grades systemic disease severity; it is distinct from the Mallampati scale (I–IV), which grades oropharyngeal view and predicts difficult laryngoscopy.
- Basic pharmacology: muscle relaxants abolish protective muscle tone, so joints and nerves lose the stretch-reflex protection during prolonged positioning.
Anatomy and Classification of Patient Positioning Hazards (AS10.1)
Surgical positioning is not a passive act — it is a deliberate clinical intervention that alters the patient's normal anatomical relationships, redistributes blood flow, and subjects tissues to sustained mechanical forces far beyond what conscious self-protective reflexes would permit. The hazards of incorrect patient positioning are classified into four major categories: nerve injuries, pressure injuries, vascular complications, and respiratory/cardiovascular compromise.
Nerve injuries are the single largest category of positioning morbidity. The brachial plexus is the most commonly injured peripheral nerve complex during surgery, most often from arm abduction beyond 90° or from a downward shoulder stretch in the lateral position. The mechanism is either stretch (the nerve is placed under longitudinal tension) or compression (the nerve is compressed between a bony structure and a hard surface). The ulnar nerve is vulnerable at the medial epicondyle when the elbow rests unpadded on the table edge — this produces cubital tunnel syndrome with ring-finger and little-finger numbness and weakness of intrinsic hand muscles. The common peroneal nerve is at risk at the fibular head in the lithotomy position, producing foot drop if the stirrups compress laterally. The femoral nerve can be damaged in the lithotomy position by extreme flexion and external rotation of the hip, or from a self-retaining retractor placed too deep. The facial nerve is vulnerable in lateral positions where the face rests on an inadequately padded head ring.
Pressure injuries (formerly "decubitus ulcers" or "pressure sores") occur when capillary perfusion pressure is exceeded at a bony prominence. In the supine position, the heels, sacrum, occiput, and elbows are the primary sites; in the prone position, the forehead, chin, sternum, anterior iliac spines, and toes carry the load. The probability of pressure injury rises steeply with duration — within two hours of unrelieved pressure at 70 mmHg, histological damage is detectable; at 35 mmHg sustained for six hours, the same damage occurs. Moist skin (from prep solutions, perspiration, or blood) increases friction and shear, accelerating injury.
Vascular complications include deep-vein thrombosis (DVT) from venous stasis — particularly in lithotomy and prone positions where calf compression is greatest — and occlusion of brachial or radial artery from overzealous strapping of the extended arm on a board. Compartment syndrome can develop in limbs compressed against hard supports for prolonged periods, particularly the calves in lithotomy.
Respiratory and cardiovascular compromise arises from the mechanical effects of position on the thorax and diaphragm. The Trendelenburg position (head-down tilt) causes the viscera to press on the diaphragm, reducing functional residual capacity (FRC), increasing peak airway pressures, impairing venous drainage from the head (risk of facial and laryngeal oedema, raised intracranial pressure), and increasing venous return. The sitting or beach-chair position dramatically reduces venous return (risk of profound hypotension and venous air embolism through open dural venous sinuses). The prone position can impair venous return, compress the abdomen (raising intra-abdominal and intrathoracic pressure, reducing venous return), and cause severe hypotension on turning if not properly managed.
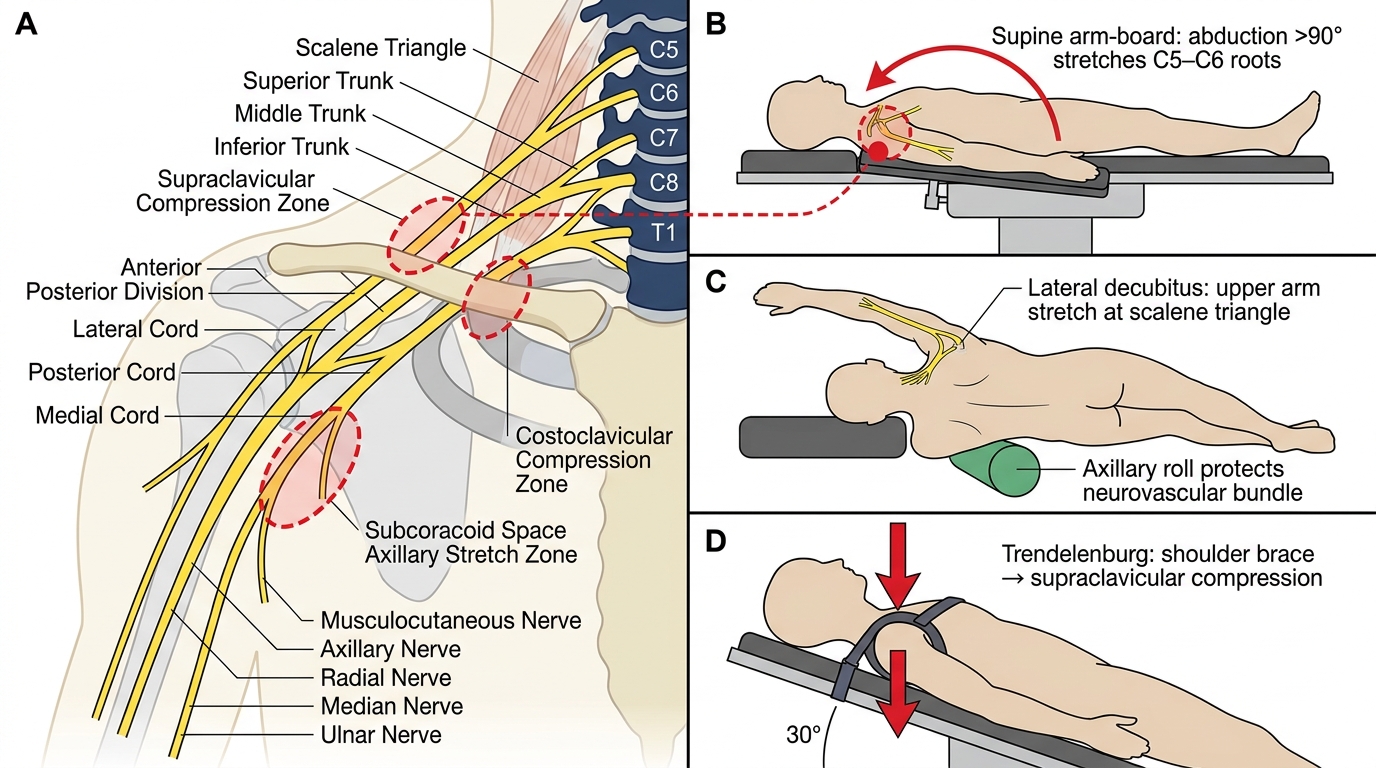
Brachial Plexus Anatomy and Position-Specific Injury Mechanisms
Ophthalmic hazards deserve special mention. Posterior ischaemic optic neuropathy (PION) and central retinal artery occlusion (CRAO) are rare but devastating causes of postoperative blindness. Risk factors include prone positioning, prolonged surgery (>6 hours), large blood loss, hypotension, and anaemia. Direct orbital pressure from a face mask or prone headrest that occludes the eye is the most preventable cause — the eye must be inspected and protected at all position changes. The anaesthesiologist must document that no direct eye pressure was present throughout the case.
Specific position hazards — a rapid reference:
- Supine: brachial plexus (arm abduction >90°), ulnar nerve (unpadded elbow), pressure sores at heels/sacrum/occiput, aortocaval compression in pregnancy (left-lateral tilt required after 20 weeks)
- Lateral decubitus: brachial plexus stretch (upper arm), peroneal nerve compression (lower leg), ear/eye pressure on dependent side, axillary roll incorrectly placed can compress the brachial neurovascular bundle
- Prone: eye pressure (direct occlusion → CRAO/PION), facial oedema, ulnar nerve at elbow, excessive abdominal compression reducing venous return and lung compliance, anterior knee and toe pressure injuries
- Lithotomy: common peroneal nerve at fibular head (most common peripheral nerve injury in obstetrics/gynaecology), femoral nerve from extreme flexion/external rotation, DVT from calf compression, compartment syndrome in prolonged cases, lumbar strain from hip-flexion discrepancy
- Trendelenburg (head-down): raised ICP, facial/laryngeal oedema, increased aspiration risk, reduced FRC and reduced pulmonary compliance
- Sitting (beach-chair): venous air embolism (VAE) from open dural sinuses (commonest in posterior cranial fossa surgery), hypotension, brachial plexus stretch if head is improperly rotated
Physiological Basis of Perioperative Hazards Beyond Positioning (AS10.2)
The perioperative period — from the decision to operate through the first 24–48 hours of recovery — is characterised by a convergence of physiological stresses that amplify one another. Understanding the pathophysiological basis of these hazards allows the anaesthesiologist to anticipate, detect, and mitigate them systematically rather than reacting to complications after they have declared themselves.
Thermoregulatory hazards are almost universal under general and neuraxial anaesthesia. Anaesthetic agents impair hypothalamic thermoregulatory control; vasodilation increases heat loss to the cool operating-theatre environment; uncovered body surfaces and cold intravenous fluids accelerate heat transfer. Hypothermia (core temperature <36°C) causes coagulopathy (platelet dysfunction and impaired enzyme kinetics of coagulation factors), myocardial irritability (increased risk of arrhythmia and post-operative shivering increasing oxygen demand), delayed drug metabolism (prolonged neuromuscular blockade, delayed awakening), surgical site infection (peripheral vasoconstriction impairs neutrophil function and tissue oxygen delivery), and impaired wound healing. Routine perioperative temperature monitoring and active warming (forced-air warming blankets, warming of IV fluids) are standard of care.
Thromboembolic hazards arise from Virchow's triad: venous stasis (from immobility, lithotomy position, raised intra-abdominal pressure), endothelial injury (from surgical trauma, central venous catheters), and a hypercoagulable state (surgical stress response, cancer, oral contraceptives, haematological disorders). Deep-vein thrombosis (DVT) is clinically silent in most patients; pulmonary embolism (PE) is a leading cause of preventable perioperative death. The Caprini risk-assessment model stratifies surgical patients into risk categories that guide thromboprophylaxis (LMWH timing, mechanical compression devices, graduated compression stockings).
Haemorrhagic hazards include both anticipated surgical blood loss and unexpected intraoperative bleeding. Coagulopathy may be pre-existing (liver disease, anticoagulant medications, inherited coagulation disorders) or acquired (massive transfusion dilutional coagulopathy, hypothermia-induced enzyme dysfunction, disseminated intravascular coagulation in obstetric catastrophes or sepsis). Point-of-care coagulation testing (TEG/ROTEM) and damage-control resuscitation principles (balanced transfusion of red cells : FFP : platelets in approximately 1:1:1 ratio) are standard in major haemorrhage.
Respiratory hazards in the perioperative period include atelectasis (the most common postoperative pulmonary complication — near-universal after general anaesthesia due to reduced FRC and supine positioning), aspiration of gastric contents (risk factors: full stomach, hiatus hernia, gastroparesis, emergency surgery, opioid-induced delayed gastric emptying), pneumonia (micro-aspiration from residual neuromuscular blockade impairing protective airway reflexes), and residual neuromuscular blockade (train-of-four monitoring mandatory; reversal with sugammadex or neostigmine).
Cardiovascular hazards include myocardial ischaemia triggered by the stress-response tachycardia and hypertension, postoperative arrhythmias (especially atrial fibrillation in thoracic and cardiac surgery), and cardiac failure from fluid overload or unrecognised hypovolaemia. Perioperative hypertension (particularly in hypertensive patients whose medications are omitted) and perioperative hypotension (from bleeding, neuraxial block, myocardial depression by anaesthetic agents) both carry organ injury risk.
Medication-related hazards are addressed in greater depth in the companion SDL (AS10.3/AS10.4). They include wrong drug, wrong dose, wrong route errors — amplified by the speed of intraoperative practice, syringe swaps (visual similarity of ampoules), look-alike/sound-alike drug names, and calculation errors for weight-based drugs.
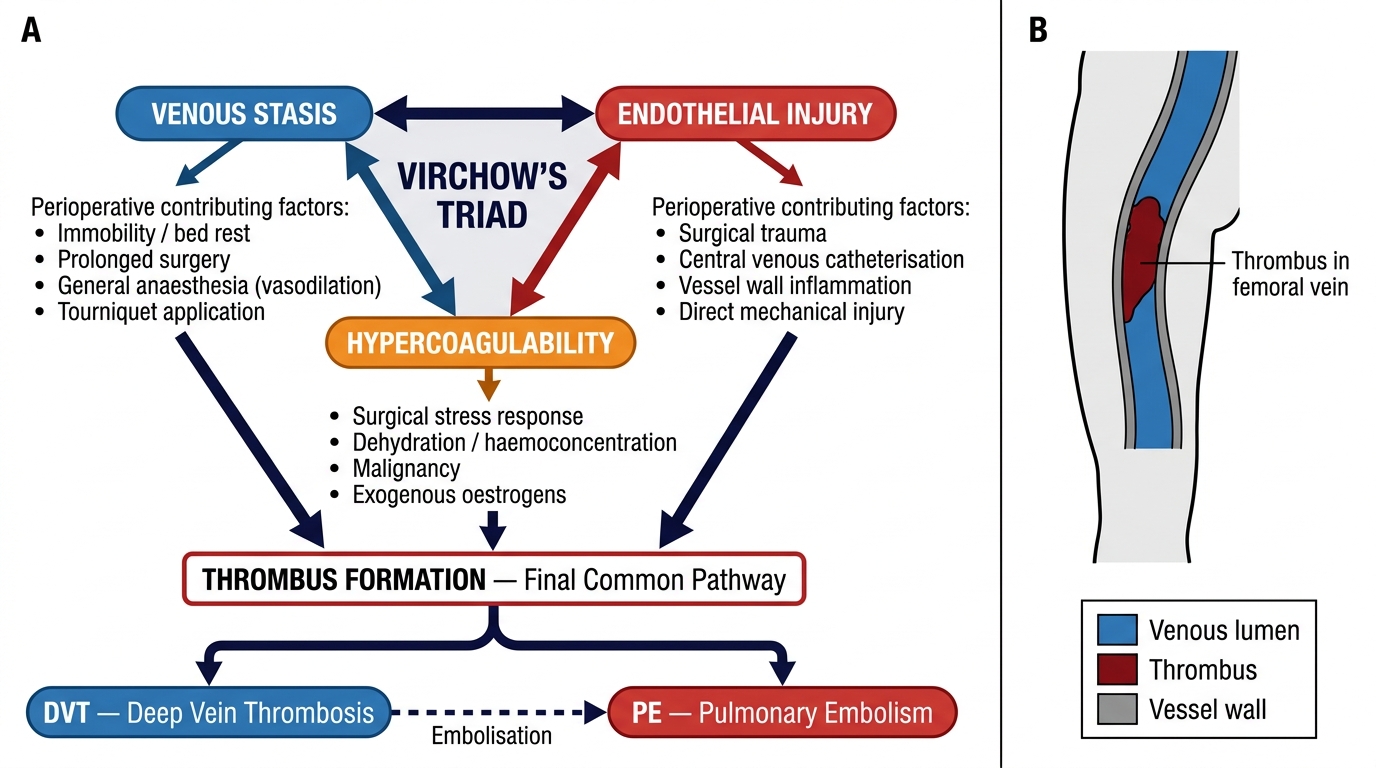
Virchow's Triad and Perioperative Risk Factors for DVT/PE
Risk Assessment and Systematic Planning for Perioperative Hazard Prevention
Hazard prevention begins not in the operating theatre but in the preoperative assessment clinic, where a structured approach identifies modifiable risks and plans mitigation strategies for the specific surgical and patient context. The anaesthesiologist's assessment is the primary checkpoint for perioperative safety because the anaesthesiologist has continuous responsibility for the patient from premedication through emergence and early recovery.
Positioning risk assessment must be documented before every case. The key questions are: (1) What position is required, and for how long? (2) What are this patient's anatomical vulnerabilities — pre-existing peripheral neuropathy, vascular disease, obesity, contractures, osteoporosis, or previous joint replacements that limit range of motion? (3) What padding and equipment are available, and are they in serviceable condition? (4) Who is responsible for positioning — typically surgeon, anaesthesiologist, and scrub team jointly; the responsibilities must be clearly assigned. The anaesthesiologist must document the position and the protective measures taken (padding sites, eye protection, arm position, presence of axillary roll if lateral) as part of the intraoperative record.
ASA Physical Status classification (I–VI, with 'E' suffix for emergency) systematically grades systemic disease burden. It is used as one input into the calculation of perioperative risk but does NOT grade operative difficulty or positioning risk specifically. Mallampati classification (I–IV) assesses the oropharyngeal view — Class I: full visibility of soft palate, fauces, uvula, pillars; Class IV: only hard palate visible — and is a predictor of difficult direct laryngoscopy. These two systems must not be conflated: ASA classifies the patient's overall health; Mallampati classifies the airway view.
Nutritional and skin assessment guides pressure-injury prevention. The Braden scale scores six domains (sensory perception, moisture, activity, mobility, nutrition, friction/shear) to stratify pressure injury risk. Patients with Braden scores ≤18 need additional padding, positioning-change protocols in recovery, and wound-care team notification.
Thromboprophylaxis planning: the Caprini score assigns point values to 40+ risk factors and groups patients into low (0–2 points), moderate (3–4), high (≥5) risk categories. High-risk non-orthopaedic patients should receive LMWH initiated 6–12 hours postoperatively (or 12 hours preoperatively if the surgical bleeding risk is low) in addition to mechanical compression devices. The timing of thromboprophylaxis is a shared anaesthesiology-surgery decision documented in the preoperative plan.
Temperature management planning involves pre-warming (forced-air warming 30 minutes preoperatively reduces the redistribution hypothermia that follows induction), warmed IV fluids for large-volume infusions, a warming blanket for all cases exceeding 30 minutes, and a core temperature target of ≥36.5°C at incision. In cardiac surgery, deliberate hypothermia is used as an organ-protective strategy — this is the specific exception to the rule, not the default.
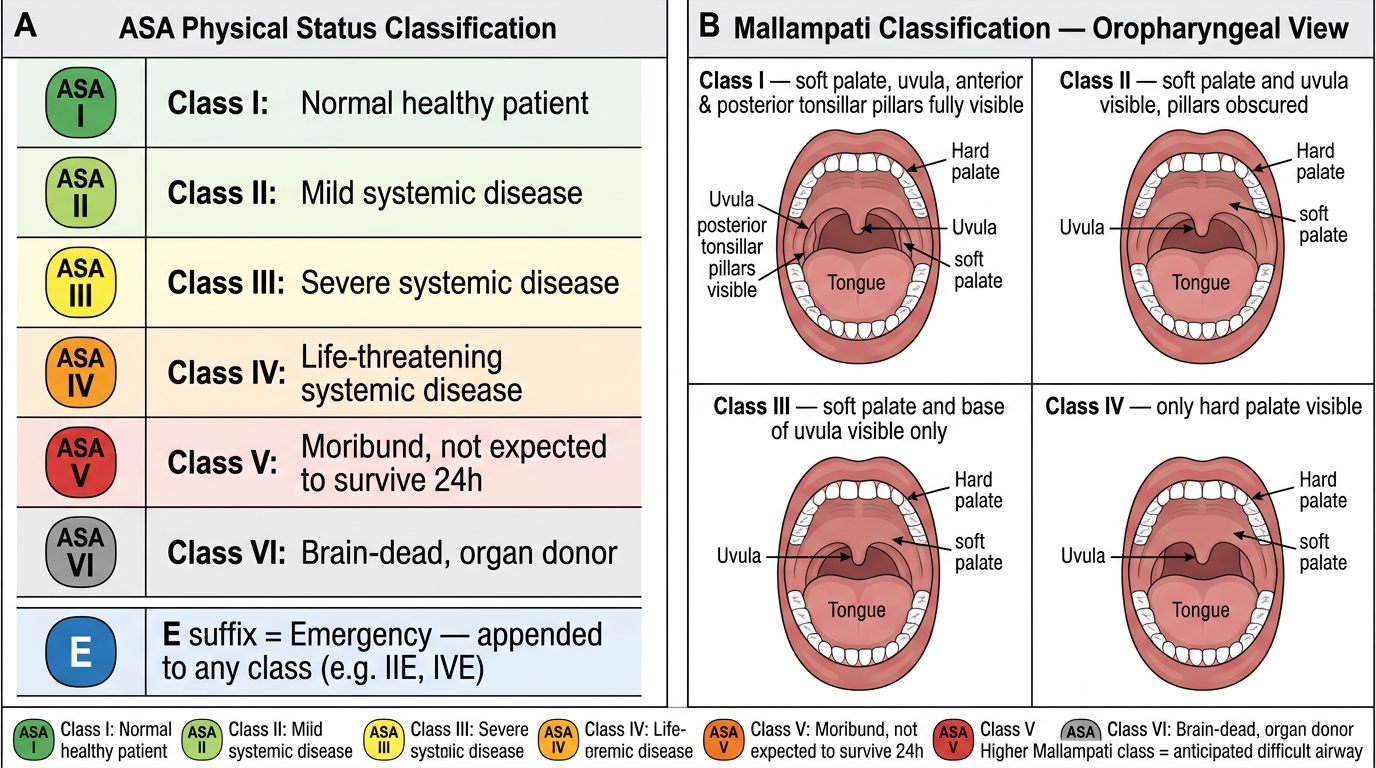
ASA Physical Status Classification and Mallampati Airway Assessment