Page 3 of 17
AS11.1-2 | Oxygen Delivery Devices and Oxygen Therapy Principles — SDL Guide (Part 3)
Safety Precautions, Complications, and Flow-Rate Adjustment
Oxygen is a powerful drug with well-documented risks when administered inappropriately, and competent oxygen therapy requires a thorough awareness of both over-oxygenation and under-oxygenation hazards. The history of medicine contains sobering examples of preventable harm from both extremes: the epidemic of retrolental fibroplasia causing blindness in preterm neonates in the 1950s resulted from liberal, unmonitored oxygen; conversely, delayed oxygen administration in acute myocardial infarction and pulmonary embolism contributes to preventable ischaemic death. In contemporary clinical practice, the most frequent error is over-oxygenation — especially in patients with COPD, where well-intentioned high-flow oxygen therapy precipitates hypercapnic respiratory failure through the Haldane effect and abolition of hypoxic pulmonary vasoconstriction. The physician who understands the physiological mechanisms underlying these hazards will prescribe oxygen precisely, titrate it to a target, and reassess regularly — treating it with the same rigor as any other drug with a narrow therapeutic window.
Risks of hyperoxia (too much oxygen):
• Absorption atelectasis — at high FiO₂, nitrogen (which normally splints alveoli open) is washed out. Poorly ventilated alveoli collapse as oxygen is absorbed faster than it is replenished.
• Oxygen toxicity — pulmonary oxygen toxicity occurs with prolonged exposure to FiO₂ >0.6 (tracheobronchitis, then diffuse alveolar damage resembling ARDS). Time-threshold is dose-dependent.
• Hypercapnia in COPD — the primary mechanism is not simply suppression of hypoxic drive (now considered a less dominant mechanism) but rather the Haldane effect (CO₂ released from carboxyhaemoglobin as haemoglobin becomes fully oxygenated) and worsening of ventilation-perfusion mismatch (as hypoxic pulmonary vasoconstriction is abolished by high FiO₂, blood flows to poorly ventilated areas, increasing dead space).
• Retinopathy of prematurity — in preterm neonates; avoid high SpO₂ targets.
Risks of hypoxia (too little or delayed oxygen):
• Delayed correction of life-threatening hypoxaemia causes hypoxic organ damage (brain, heart, kidney).
• Delayed pre-oxygenation before anaesthetic induction shortens the safe apnoea time during laryngoscopy.
Fire safety — oxygen enriches the environment and makes combustion more vigorous. All ignition sources (cautery, cigarettes) must be absent from the immediate vicinity. In the operating theatre, oxygen-enriched gases under drapes are a fire hazard with electrosurgical diathermy.
Flow-rate adjustment principles:
• Titrate upward in steps until the target SpO₂ is achieved; do not over-prescribe.
• In COPD, start at the lowest effective Venturi FiO₂ (24% or 28%) and check ABG within 30–60 minutes.
• If the target SpO₂ cannot be achieved on the current device, escalate to the next device tier (nasal cannula → simple mask → NRM → HFNC → non-invasive ventilation → mechanical ventilation).
• Always re-assess after any device change or clinical deterioration.
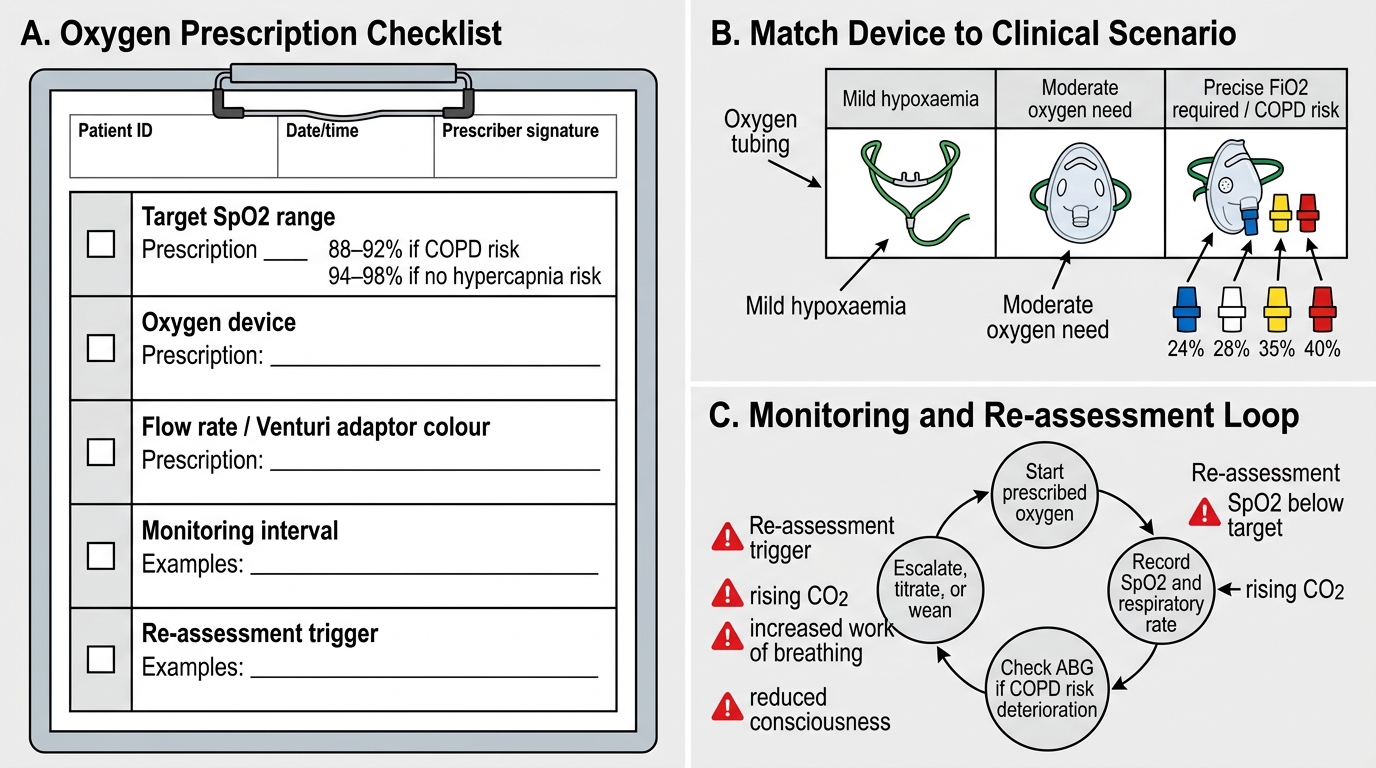
Ward Oxygen Prescription Checklist
Clinical Applications: Matching Device to Scenario
The practical application of oxygen therapy principles requires matching the device to the clinical scenario by synthesising the severity of hypoxaemia, the need for FiO₂ precision, and the patient's respiratory effort. The following framework, consistent with both Morgan & Mikhail's Clinical Anesthesiology and Ajay Yadav's Short Textbook of Anaesthesia, covers the most common clinical situations a graduating doctor will encounter.
Scenario 1 — Pre-oxygenation before anaesthetic induction: A well-fitting NRM with oxygen flowing at 15 L/min for 3–5 minutes achieves an FiO₂ close to 1.0, filling the functional residual capacity (FRC) with oxygen. This extends the safe apnoea time from approximately 1 minute on room air to 8–10 minutes in a healthy adult. In obese patients or those with reduced FRC (pregnant, supine), adding head-up positioning further improves preoxygenation. The NRM seal must be tight — any leak significantly reduces the achieved FiO₂.
Scenario 2 — COPD exacerbation with chronic hypercapnia: Start with a 24% or 28% Venturi adaptor and target SpO₂ 88–92%. Check ABG at 30–60 minutes. Titrate Venturi adaptor upward only if SpO₂ remains below 88% and CO₂ is not rising. Never start with an NRM in this population — the resulting high FiO₂ can precipitate life-threatening hypercapnia. If ventilatory failure occurs despite controlled oxygen, non-invasive ventilation (NIV/BiPAP) is the next step.
Scenario 3 — Acute severe hypoxaemia (ARDS, pneumonia, PE): Apply NRM at 15 L/min immediately to achieve highest possible FiO₂ (60–90%) while arranging ABG, chest X-ray, and ICU review. HFNC is an effective next step if NRM is insufficient and the patient remains alert and cooperative. SpO₂ target ≥94%.
Scenario 4 — Carbon monoxide poisoning: Apply NRM at 15 L/min regardless of apparent SpO₂ (which will be falsely reassuring because pulse oximetry cannot distinguish carboxyhaemoglobin from oxyhaemoglobin). High FiO₂ shortens the half-life of carboxyhaemoglobin from ~5 hours on room air to ~60–90 minutes on 100% O₂. ABG with co-oximetry or co-oximetry is the only reliable measure of carboxyhaemoglobin.
Scenario 5 — Postoperative care: Most postoperative patients receive nasal cannula at 2–4 L/min. Escalate to simple mask or NRM if SpO₂ falls below 94%. Inspect for airway obstruction, pain splinting, opioid respiratory depression, or residual neuromuscular blockade before attributing hypoxaemia to primary lung disease.
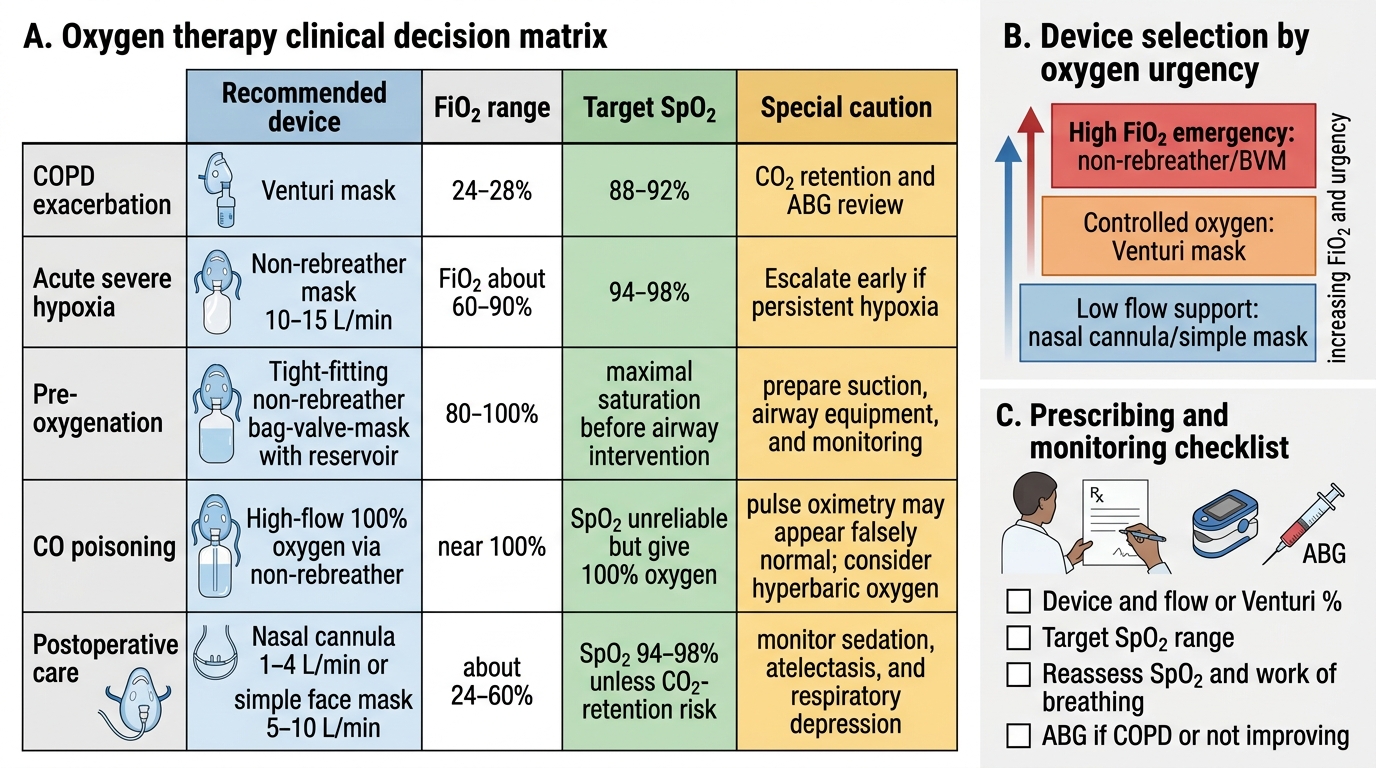
Oxygen Therapy Device Selection Matrix
Self-Assessment: Consolidating Device Selection and Prescribing Principles
Having worked through the classification of oxygen delivery devices, the principles governing FiO₂ delivery, the monitoring requirements during oxygen therapy, and the clinical applications across five common scenarios, this self-assessment section gives you the opportunity to consolidate the key decision points and identify any gaps before clinical practice. The ability to rapidly select the correct device, set the appropriate flow rate or Venturi adaptor, prescribe the right target SpO₂, and know when to escalate is a fundamental clinical competency that will be tested formally in OSCEs and assessed on every ward round. Spending ten minutes now working through the questions below — before consulting the explanations — is far more effective preparation than passive re-reading. Active recall promotes durable retention and surfaces the specific knowledge gaps that passive review conceals. Treat each question as a mini-OSCE station: state your answer out loud, then check.
Core questions to test yourself:
1. A patient's SpO₂ is 86% on room air. What device would you apply first if the patient has no known lung disease? What if the patient has known COPD?
2. What is the minimum flow rate for a simple face mask, and why? What happens if you set it lower?
3. A Venturi mask has a blue adaptor. What FiO₂ does it deliver, and what flow rate must be set?
4. Why does pulse oximetry give a falsely normal reading in carbon monoxide poisoning? What test do you order?
5. A preoperative patient needs pre-oxygenation before rapid sequence induction. Which device, what flow, and for how long?
6. What are three mechanisms by which high FiO₂ worsens hypercapnia in COPD?
For each question, apply the framework from this module: identify the clinical scenario, determine whether FiO₂ precision is required, select the device, specify the flow rate or Venturi adaptor colour, state the target SpO₂, and identify the monitoring parameter you will check at 30 minutes. Practising this systematic approach — even on paper before your clinical postings — builds the automatic fluency you need when seconds matter.
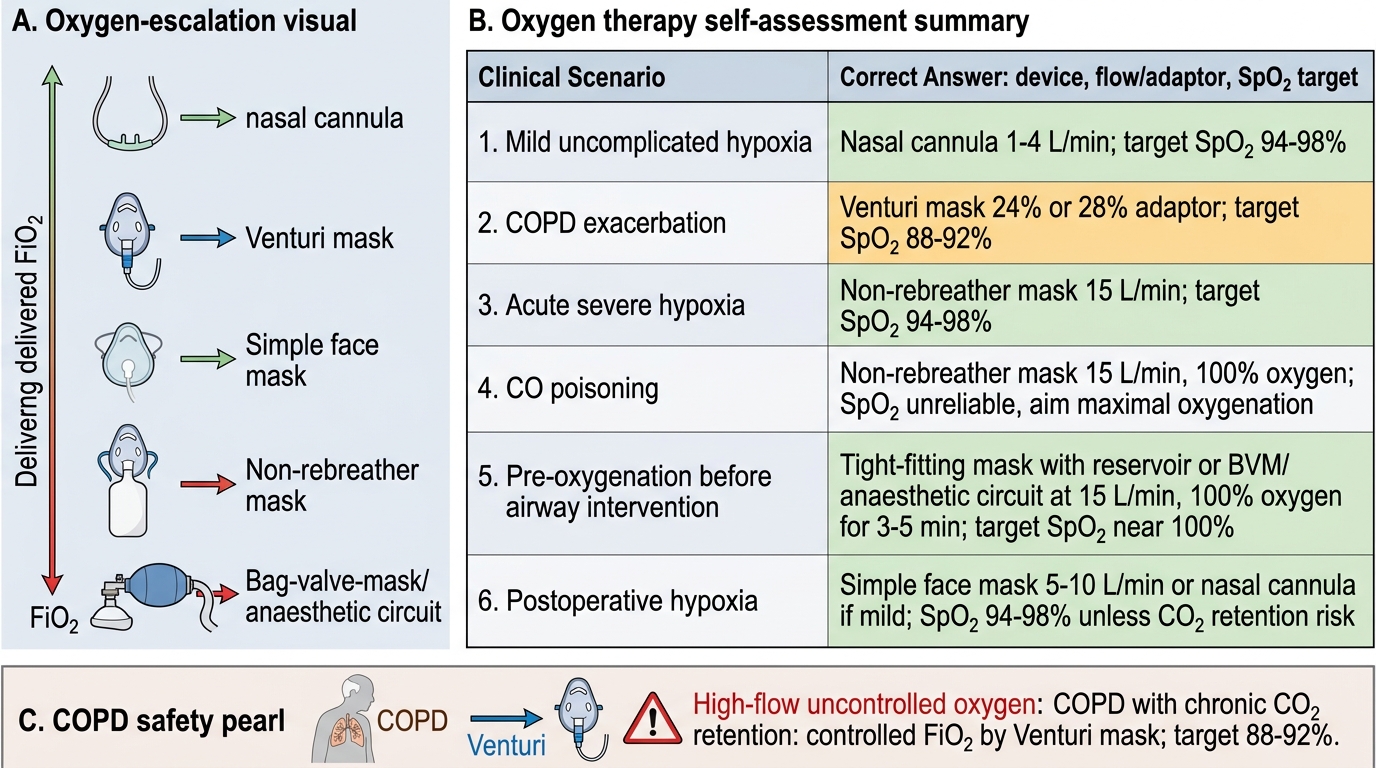
Oxygen Therapy Device and SpO2 Target Summary
SELF-CHECK
A 72-year-old woman with severe COPD and an SpO₂ of 80% is brought to the emergency department. Which oxygen delivery device and target SpO₂ are most appropriate for initial management?
A. Non-rebreather mask at 15 L/min; target SpO₂ ≥94%
B. Venturi mask with 24% adaptor; target SpO₂ 88–92%
C. Simple face mask at 8 L/min; target SpO₂ ≥94%
D. Nasal cannula at 6 L/min; target SpO₂ 88–92%
Reveal Answer
Answer: B. Venturi mask with 24% adaptor; target SpO₂ 88–92%
In COPD with chronic CO₂ retention, a Venturi mask with the 24% or 28% adaptor is the device of choice because it delivers a fixed, controlled FiO₂ that can be precisely titrated. The target SpO₂ in COPD is 88–92%, not the standard ≥94%, because a higher target can suppress hypoxic drive and worsen hypercapnia via the Haldane effect and V/Q mismatch. A non-rebreather mask delivers uncontrolled high FiO₂ (60–90%) and risks precipitating hypercapnic respiratory failure. A nasal cannula at 6 L/min delivers variable FiO₂ (~44%) and provides no FiO₂ precision — also unsuitable for a patient at risk of CO₂ retention.
CLINICAL PEARL
Venturi mask = fixed performance, not 'Venturi effect for all flows.' The FiO₂ delivered by a Venturi mask is precisely controlled only at the flow rate specified on the adaptor. If you increase the flow rate beyond the specified value, the entrainment ratio changes and the delivered FiO₂ rises above the labelled value — the mask is no longer fixed-performance. Always use the exact flow rate printed on the colour-coded Venturi adaptor. Similarly, the NRM's reservoir bag must remain at least one-third inflated throughout the respiratory cycle; a fully collapsed bag means the patient is not receiving the intended FiO₂. Check the bag visually before leaving the bedside.