Page 8 of 15
AS3.6 | Premedication Selection and Prescription for Surgical Patients — SDL Guide
CLINICAL SCENARIO
The night before surgery, a 42-year-old woman with severe dental anxiety is listed for a mandibular osteotomy under general anaesthesia. She is visibly trembling when you visit her on the ward. On the other side of the ward, a 68-year-old man with heart failure and COPD is listed for an inguinal hernia repair under spinal anaesthesia. Both patients will benefit from premedication — but the drugs, doses, and routes appropriate for one could be dangerous for the other. Premedication is not a single default prescription. It is a clinical decision that must match the drug's mechanism to the patient's need, comorbidities, and the planned anaesthetic technique. This module teaches you how to make and write that decision.
WHY THIS MATTERS
Premedication — the administration of drugs before the induction of anaesthesia — is one of the most individualised prescribing decisions in clinical medicine. A poorly chosen premedication can cause respiratory depression in a patient with COPD, prolong emergence in an elderly patient, or fail to prevent aspiration in a patient with gastro-oesophageal reflux. A well-chosen premedication reduces patient anxiety, blunts the haemodynamic stress of induction, prevents aspiration pneumonitis, and reduces postoperative nausea and vomiting. For a final-year MBBS student, the ability to select and write a correct premedication prescription reflects mastery of pharmacology, clinical judgement, and safe prescribing practice — skills that transfer directly to inpatient and emergency prescribing after graduation.
References: Morgan & Mikhail's Clinical Anesthesiology; Ajay Yadav's Short Textbook of Anaesthesia; Paul Barash's Clinical Anesthesia.
RECALL
Before proceeding, recall: (1) the major drug classes used in anaesthesia — induction agents, opioids, benzodiazepines, anticholinergics, and antiemetics — and their primary mechanisms; (2) the physiological consequences of preoperative anxiety — sympathetic activation, tachycardia, hypertension, and increased anaesthetic requirements; (3) the pharmacokinetic concepts of onset time, peak effect, and duration of action — critical for timing a premedication to the anticipated start of anaesthesia; (4) the concept of aspiration risk and why certain patients are at higher risk of gastric content aspiration under general anaesthesia.
Clinical Indication and Goals of Premedication
Premedication refers to any drug administered before the induction of anaesthesia with the aim of improving the patient's perioperative experience and reducing anaesthetic risk. The term encompasses a wide range of drug classes — from anxiolytics and sedatives to antacids and antiemetics — each targeting a specific clinical problem identified during the preoperative assessment. Premedication is not mandatory for every patient, but when it is indicated, the drug selection, dose, route, and timing must be specified precisely in a written prescription.
The clinical goals of premedication can be grouped into five categories, each corresponding to a specific patient need or anaesthetic concern. First, anxiolysis and sedation: preoperative anxiety is nearly universal and is associated with increased anaesthetic requirements, delayed recovery, and a higher incidence of postoperative psychological distress. Anxiolytics given 30-90 minutes before surgery attenuate the catecholamine surge associated with the pre-induction period, reduce the dose of induction agent needed, and improve the patient's experience. Second, analgesia: certain patients benefit from preoperative analgesia — particularly those with existing chronic pain, those undergoing procedures with significant postoperative pain, or those in whom multimodal analgesia (giving an analgesic before the painful stimulus) can reduce intraoperative and postoperative opioid consumption. Third, prevention of aspiration pneumonitis: patients at high risk of gastric content aspiration — those with gastro-oesophageal reflux disease (GORD), obesity, diabetes with gastroparesis, hiatus hernia, or emergency surgery — benefit from drugs that raise gastric pH or reduce gastric volume. Fourth, prevention of postoperative nausea and vomiting (PONV): prophylactic antiemetics given preoperatively reduce the incidence and severity of PONV, which is a major cause of postoperative distress, delayed discharge, and unplanned hospital admission after day surgery. Fifth, autonomic modification: in certain situations, drugs are given to modify autonomic tone — to reduce secretions (an anticholinergic before a fibreoptic bronchoscopy), to blunt the hypertensive response to laryngoscopy (a beta-blocker or opioid), or to prevent bradycardia during ophthalmic procedures.
Not every patient needs premedication for all five goals. The premedication prescription must be tailored to the individual patient's risk profile as identified at the preoperative assessment. A well-designed premedication prescription states: the drug name, dose, route of administration, and the time before anaesthesia induction at which the drug should be given.
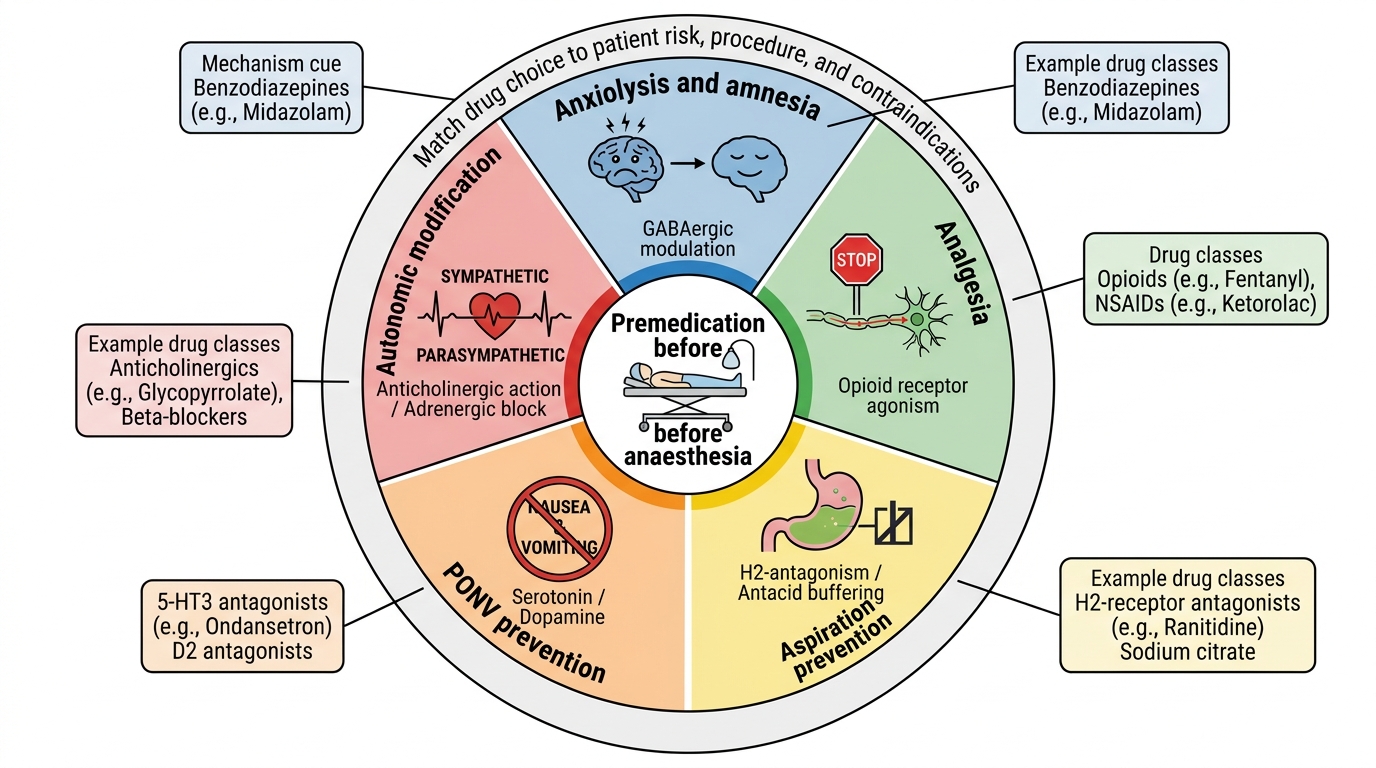
Five Goals of Premedication
Anatomy and Governing Pharmacological Principles
The pharmacological basis of premedication rests on the mechanisms of the drug classes most commonly used in the perioperative period. Understanding the mechanism of each drug class allows the prescriber to predict its effects, anticipate its interactions with anaesthetic agents, and avoid giving it to patients in whom it is contraindicated.
Benzodiazepines act by binding to the GABA-A receptor, enhancing inhibitory chloride channel conductance and producing anxiolysis, sedation, anterograde amnesia, and anticonvulsant effects. The key perioperative property is their ability to reduce preoperative anxiety and provide amnesia for the pre-induction period without causing significant respiratory depression at anxiolytic doses in healthy patients. However, in elderly patients and those with respiratory compromise, even modest benzodiazepine doses can cause significant respiratory depression and prolonged sedation. Midazolam is the benzodiazepine of choice for premedication because it has a short half-life (1-4 hours), rapid onset (15-30 minutes orally, 3-5 minutes IV), and high water solubility (can be given orally, intramuscularly, or intravenously). The oral route is most commonly used for premedication: 0.5 mg/kg up to a maximum of 15 mg in children; 5-7.5 mg in adults. Benzodiazepines are reversed by flumazenil (a competitive GABA-A antagonist) — but note that flumazenil has a shorter duration of action than midazolam, so re-sedation can occur.
Opioids used as premedication (morphine, pethidine, fentanyl, buprenorphine) act on mu, kappa, and delta receptors to produce analgesia, sedation, and euphoria. Preoperative opioids are used primarily to provide baseline analgesia before major surgery and to blunt the haemodynamic response to laryngoscopy. Their key adverse effects relevant to premedication are: nausea and vomiting (histamine release from morphine can trigger PONV — counterproductive if given to a high-PONV-risk patient), respiratory depression (particularly in opioid-naive elderly patients or those with sleep apnoea), and delayed gastric emptying (worsen aspiration risk). For these reasons, opioids are not used routinely as premedication and are reserved for specific indications.
Anticholinergic agents — atropine and glycopyrrolate — block muscarinic receptors, reducing salivary and bronchial secretions, preventing reflex bradycardia (particularly during ophthalmic procedures, laparoscopy, or paediatric anaesthesia where vagal stimulation is common), and producing bronchodilation. Glycopyrrolate is preferred over atropine in most situations because it does not cross the blood-brain barrier (so does not cause confusion or central anticholinergic syndrome) and has a more sustained antisecretory effect. Atropine is preferred when rapid reversal of severe bradycardia is needed, or when given to children in emergency settings. Anticholinergics are used selectively, not routinely.
Antacids and prokinetics target aspiration risk. Sodium citrate (0.3 M, 30 mL orally 15-30 minutes before induction) is a non-particulate antacid that rapidly raises gastric pH above 2.5 — the critical threshold for chemical pneumonitis if aspiration occurs. It is routinely used before emergency surgery and obstetric general anaesthesia. Ranitidine (H2 receptor antagonist) and omeprazole (proton pump inhibitor) reduce gastric acid secretion when given 60-90 minutes before surgery. Metoclopramide (a dopamine D2 antagonist with prokinetic properties) accelerates gastric emptying and raises the lower oesophageal sphincter tone — it is used in patients at high aspiration risk (obesity, GORD, diabetes with gastroparesis). Note: metoclopramide also has antiemetic properties via its central D2 antagonism.
Antiemetics used as premedication include: ondansetron (5-HT3 antagonist — the most widely used, minimal sedation, effective for opioid- and volatile-agent-related PONV), dexamethasone (corticosteroid — given intraoperatively at induction, reduces PONV and provides postoperative analgesia), metoclopramide (D2 antagonist — see above), and promethazine (phenothiazine antihistamine — sedation plus antiemetic, but causes prolonged sedation and extrapyramidal effects). Dexamethasone 4-8 mg IV at induction is one of the most effective single PONV prophylaxis measures and is widely used.
Beta-blockers and alpha-2 agonists can be given preoperatively to blunt the haemodynamic stress of induction and laryngoscopy. Esmolol (ultra-short-acting beta-1 blocker) given IV just before laryngoscopy attenuates tachycardia and hypertension. Clonidine (alpha-2 agonist) given orally 60-90 minutes before surgery reduces anaesthetic requirements, provides sedation and analgesia, and stabilises heart rate — useful in patients with ischaemic heart disease. Dexmedetomidine (highly selective alpha-2 agonist, IV infusion) provides titratable sedation without respiratory depression — useful for procedural sedation and ICU sedation but not typically used as oral premedication.
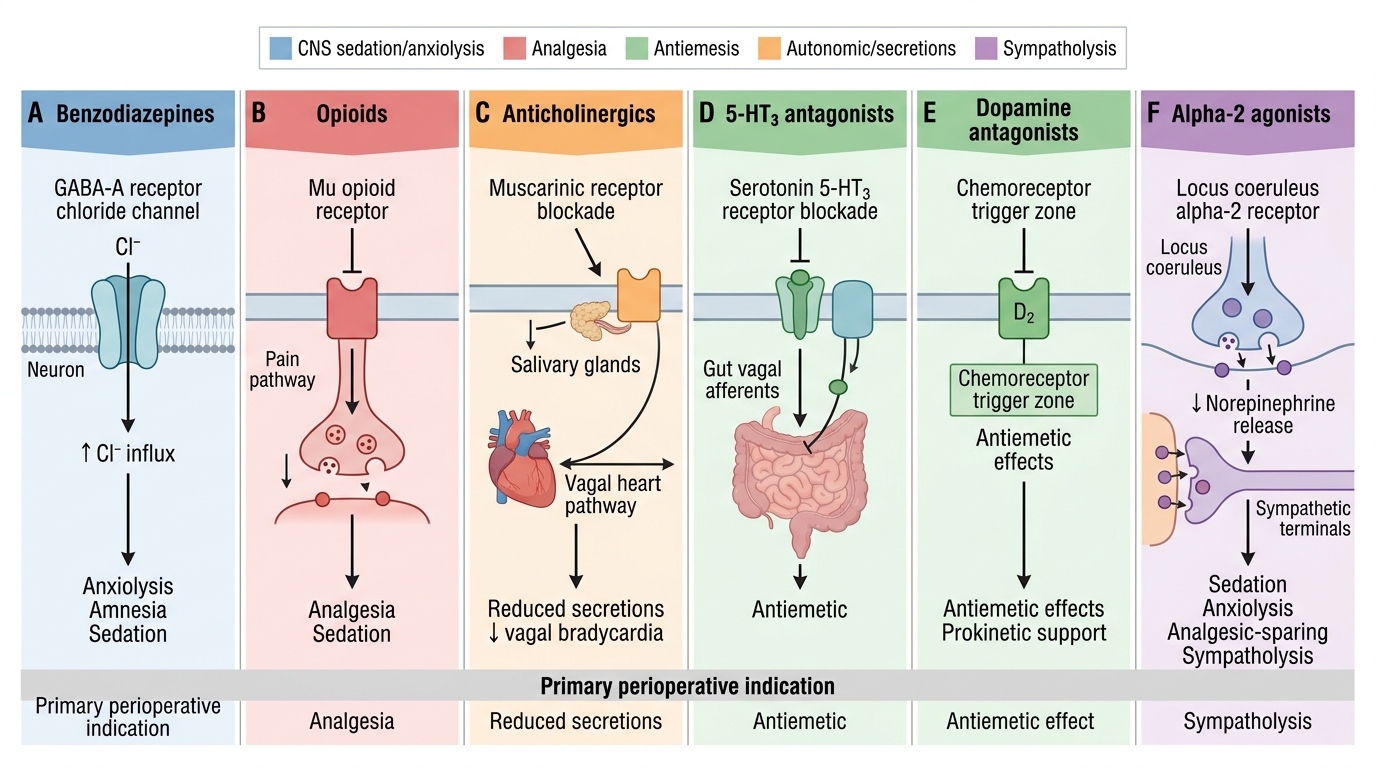
Premedication Drug Classes: Receptor Targets and Perioperative Effects
Drug Selection, Dosing, and Prescription Writing
Selecting the appropriate premedication requires integrating the patient's clinical profile — identified at the pre-anaesthetic assessment — with the pharmacological properties of available agents. This section covers the practical framework for drug selection and the correct format for a premedication prescription.
The selection framework proceeds in five questions. First, what is the primary indication for premedication? Anxiety and phobia — choose a benzodiazepine. High PONV risk — choose a prophylactic antiemetic. High aspiration risk — choose sodium citrate, ranitidine, or metoclopramide. Significant preoperative pain — consider an opioid or non-opioid analgesic. Second, are there contraindications to the first-choice agent? Benzodiazepines: avoid in severe respiratory failure (COPD with CO2 retention), liver failure (impaired metabolism), obstructive sleep apnoea (respiratory depression in recovery), and elderly patients with cognitive impairment (risk of paradoxical agitation and prolonged sedation). Opioids: avoid in opioid-naive patients with high aspiration risk or sleep apnoea. Third, what route of administration is appropriate? Oral is most common and acceptable for elective cases when there is sufficient time (30-90 minutes before induction). Intramuscular is used when oral absorption is unreliable or the patient is nil by mouth. Intravenous is reserved for administration in the anaesthetic room or theatre when rapid onset is needed. Fourth, what dose is appropriate for this patient's age, weight, and renal/hepatic function? Drug doses must be adjusted downward for the elderly (reduced hepatic metabolism, reduced renal clearance, increased brain sensitivity), for patients with hepatic impairment (benzodiazepine accumulation), and for patients at extremes of weight. Fifth, what is the timing? A premedication given too early peaks before induction; given too late it has not reached peak effect at the time of induction. Know the onset-to-peak times for each drug and route.
Common premedication prescriptions with appropriate clinical indications:
1. Anxiolysis (midazolam)
- Adult elective surgery with significant anxiety: Midazolam 5-7.5 mg orally, 30-60 minutes before anaesthesia induction
- Child: Midazolam 0.5 mg/kg orally (maximum 15 mg), 30-45 minutes before induction (pleasant-tasting syrup formulation available)
- Elderly or respiratory-compromised: midazolam dose should be reduced to 2.5-5 mg or avoided entirely
2. Aspiration prophylaxis (high-risk patient: GORD, obesity, emergency)
- Sodium citrate 0.3 M, 30 mL orally, 15-30 minutes before induction (non-particulate antacid, immediate pH effect)
- Ranitidine 150 mg orally (or 50 mg IV), 60-90 minutes before induction (H2 blocker, reduces acid production)
- Metoclopramide 10 mg orally or IV, 30-60 minutes before induction (prokinetic + antiemetic; avoid in Parkinson's disease and bowel obstruction)
3. PONV prophylaxis (high-risk: female, non-smoker, PONV history, long surgery)
- Ondansetron 4-8 mg IV at induction (or 8 mg orally 1 hour before)
- Dexamethasone 4-8 mg IV at induction (anti-inflammatory antiemetic; avoid in diabetics perioperatively as it causes hyperglycaemia)
- Combination is more effective than single agent for high-risk patients
4. Antisecretory/antisialogogue (for fibreoptic intubation, paediatric)
- Glycopyrrolate 0.2 mg IM, 30-60 minutes before procedure (preferred — does not cross blood-brain barrier)
- Atropine 0.6 mg IM (alternative — may cause central effects in elderly; preferred in severe bradycardia)
5. Analgesic premedication (multimodal)
- Paracetamol 1 g orally, 1 hour before surgery (effective, safe, no respiratory effects)
- Celecoxib 400 mg orally (COX-2 inhibitor; avoid in renal impairment, cardiovascular disease)
- Pregabalin 75-150 mg orally (neuropathic pain, reduces postoperative opioid requirements; caution for sedation in elderly)
Prescription format: Every premedication prescription must state: (1) the generic drug name; (2) the dose in mg (not 'one tablet'); (3) the route (oral, IM, IV); (4) the time before anticipated anaesthesia induction; (5) any conditional instruction ('only if patient is calm' or 'hold if SpO2 below 94%'). The prescribing clinician must sign, date, and designate their bleep/contact for queries.
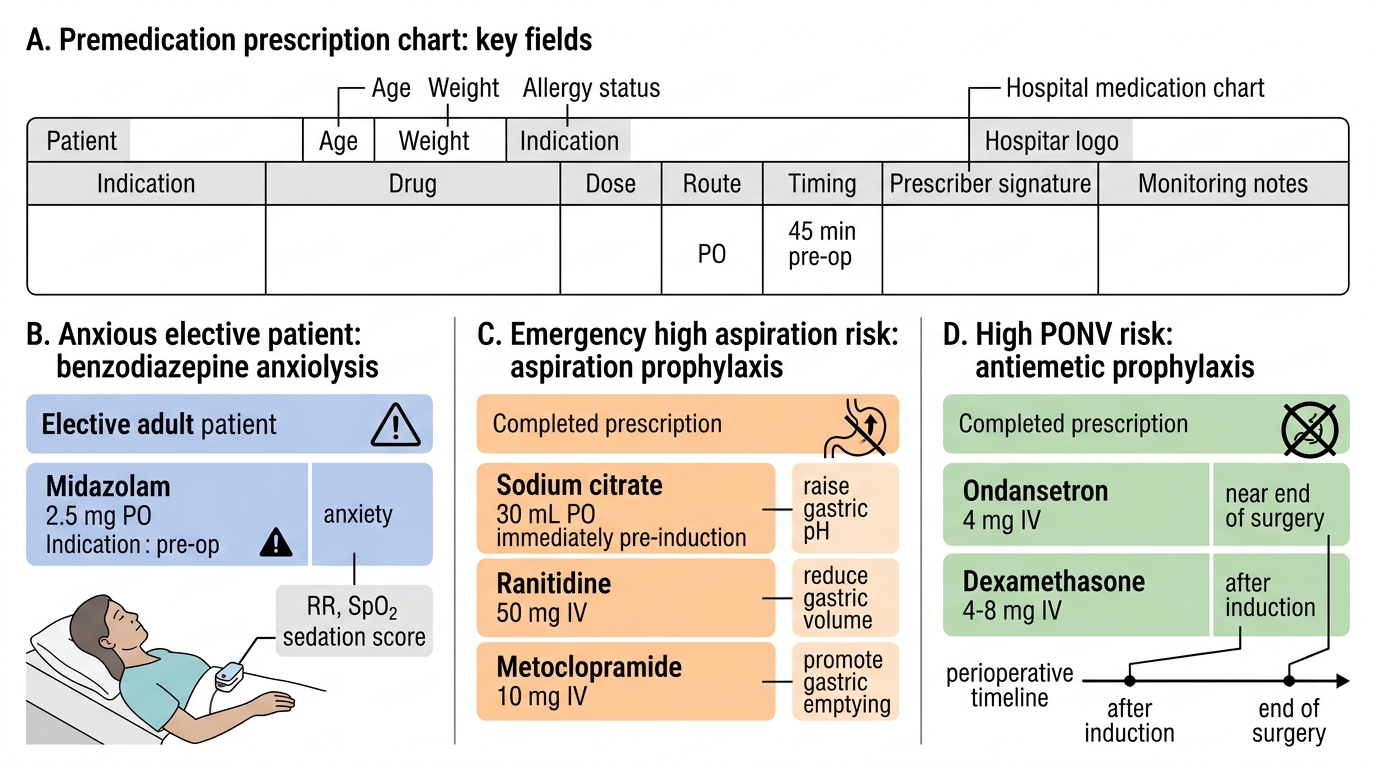
Sample Premedication Prescription Chart
SELF-CHECK
A 65-year-old woman with severe COPD (FEV1 45% predicted, resting SpO2 92%) is scheduled for elective cystoscopy under general anaesthesia. She is anxious about the procedure. Which premedication choice is MOST appropriate?
A. A. Midazolam 7.5 mg orally 45 minutes before surgery
B. B. Midazolam 2.5 mg orally 45 minutes before surgery with close monitoring
C. C. Morphine 10 mg IM 45 minutes before surgery for sedation and anxiolysis
D. D. No premedication — verbal reassurance and the presence of a nurse are sufficient if pharmacological options are contraindicated
Reveal Answer
Answer: B. B. Midazolam 2.5 mg orally 45 minutes before surgery with close monitoring
Standard adult midazolam doses (5-7.5 mg) are potentially dangerous in severe COPD with CO2 retention and a resting SpO2 of 92%, as benzodiazepines cause respiratory depression that can worsen hypercapnia and precipitate respiratory failure. However, if anxiolysis is genuinely needed, a reduced dose (2.5 mg) with close monitoring of respiratory rate and SpO2 is the most appropriate pharmacological option. Morphine 10 mg IM would cause significant respiratory depression and worsen PONV risk — clearly inappropriate. The question states pharmacological options are NOT contraindicated (option D is for cases where they are), so a reduced-dose benzodiazepine with monitoring is preferred over no medication. The key principle is dose reduction, not blanket avoidance, in respiratory compromise — matched to the degree of impairment.