Page 1 of 15
AS3.{1,4-5} | Principles, Testing and Fitness Decisions in Preoperative Evaluation — SDL Guide
CLINICAL SCENARIO
A 58-year-old man with poorly controlled hypertension and a recent history of angina is scheduled for an elective inguinal hernia repair. The surgeon asks whether the patient is 'fit for surgery.' As the anaesthesiologist, you must synthesise his cardiac status, exercise tolerance, current medications, and the physiological stress of the planned procedure into a single, defensible fitness decision — and communicate that decision clearly to the operating team. This is preoperative evaluation in practice: not a bureaucratic checklist, but a structured clinical reasoning exercise that directly determines whether the patient enters the operating room safely.
WHY THIS MATTERS
Preoperative evaluation is one of the few moments in a surgical patient's journey when the anaesthesiologist has full access to the patient, the time to ask detailed questions, and the authority to modify or defer a planned procedure. Studies consistently show that structured preoperative assessment reduces unexpected intraoperative events, shortens post-anaesthesia care unit (PACU) stays, and prevents cancellations on the day of surgery. For final-year MBBS students entering residency, understanding how to evaluate a patient before anaesthesia — identifying risk factors, ordering the right investigations, and making a defensible fitness decision — is foundational to safe surgical practice across every specialty.
References: Morgan & Mikhail's Clinical Anesthesiology; Ajay Yadav's Short Textbook of Anaesthesia; ASA Practice Advisory for Preanesthesia Evaluation (2012, reaffirmed 2019).
RECALL
Before proceeding, recall the following core concepts: (1) the physiological consequences of general anaesthesia — loss of protective airway reflexes, respiratory depression, cardiovascular depression, and blunting of the stress response; (2) the basic functional anatomy of the cardiovascular system, particularly the determinants of cardiac output (heart rate x stroke volume) and how afterload and preload are affected by anaesthetic drugs; (3) the concept of organ reserve — the difference between resting organ function and maximal capacity; and (4) the pharmacokinetic principle of context-sensitive half-life, which explains why a patient's renal or hepatic disease can dramatically prolong drug action and recovery time.
Principles of Preoperative Evaluation
The preoperative evaluation (also called the pre-anaesthetic assessment) is a systematic clinical appraisal conducted before any elective, urgent, or emergency procedure requiring anaesthesia. Its fundamental purpose is to identify conditions that increase anaesthetic and surgical risk, to optimise those conditions where time permits, and to formulate an individualised anaesthetic plan that accounts for the patient's current physiological state and the demands of the planned procedure.
Three interlocking principles underpin every preoperative evaluation. First, risk stratification: every patient carries some baseline risk that arises from their comorbidities, physiological reserve, and the magnitude of the planned surgical stress. This risk can rarely be eliminated, but it can be quantified, communicated, and in many cases reduced through targeted optimisation. Second, fitness versus risk: declaring a patient 'fit for anaesthesia' does not mean risk-free — it means the estimated benefit of the procedure outweighs the estimated risk of the anaesthetic-surgical combination. This is always a nuanced, patient-specific judgement, not a binary pass/fail. Third, the anaesthesiologist-surgeon partnership: the preoperative evaluation must produce information that is useful to the entire operating team. Concerns that cannot be resolved before surgery must be documented and communicated explicitly.
The scope of the preoperative evaluation covers: a structured history (including surgical history, anaesthetic history, medication history, and systems review); a focused clinical examination (airway, cardiovascular, respiratory, and other systems as indicated); targeted investigations selected by clinical need rather than routine policy; risk scoring using validated instruments; and a documented anaesthetic plan including the fasting instruction, premedication order, and consent discussion.
Two separate classification scales are routinely applied at the preoperative evaluation and are frequently confused. The ASA Physical Status classification (I-VI, with an 'E' suffix for emergency) grades the severity of a patient's systemic disease. It is used for risk communication and research stratification, but it does NOT directly grade operative difficulty or predict specific complications. The Mallampati classification (I-IV) grades the oropharyngeal view during mouth opening and is an airway predictor for laryngoscopy difficulty — it is an entirely different scale applied to an entirely different clinical question.
ASA Physical Status grades: ASA I — normal healthy patient; ASA II — mild systemic disease (well-controlled hypertension, mild asthma, BMI 30-40, pregnancy); ASA III — severe systemic disease (poorly controlled hypertension, COPD, morbid obesity BMI >40, ESRD on dialysis, MI/CVA/TIA >3 months ago); ASA IV — constant threat to life (recent MI/CVA/TIA within 3 months, severe valvular dysfunction, sepsis); ASA V — moribund patient unlikely to survive without the operation; ASA VI — brain-dead patient for organ donation. The E suffix (e.g. ASA IIE) denotes emergency surgery.
Preoperative fasting follows the ASA 2017 '2-4-6-8 rule': clear fluids (water, apple juice, black coffee, black tea) = 2 hours; breast milk = 4 hours; formula milk, non-human milk, or light meal = 6 hours; fatty or fried food, meat, heavy meal = 8 hours. A blanket 'nil by mouth after midnight' instruction is outdated and should not be used.
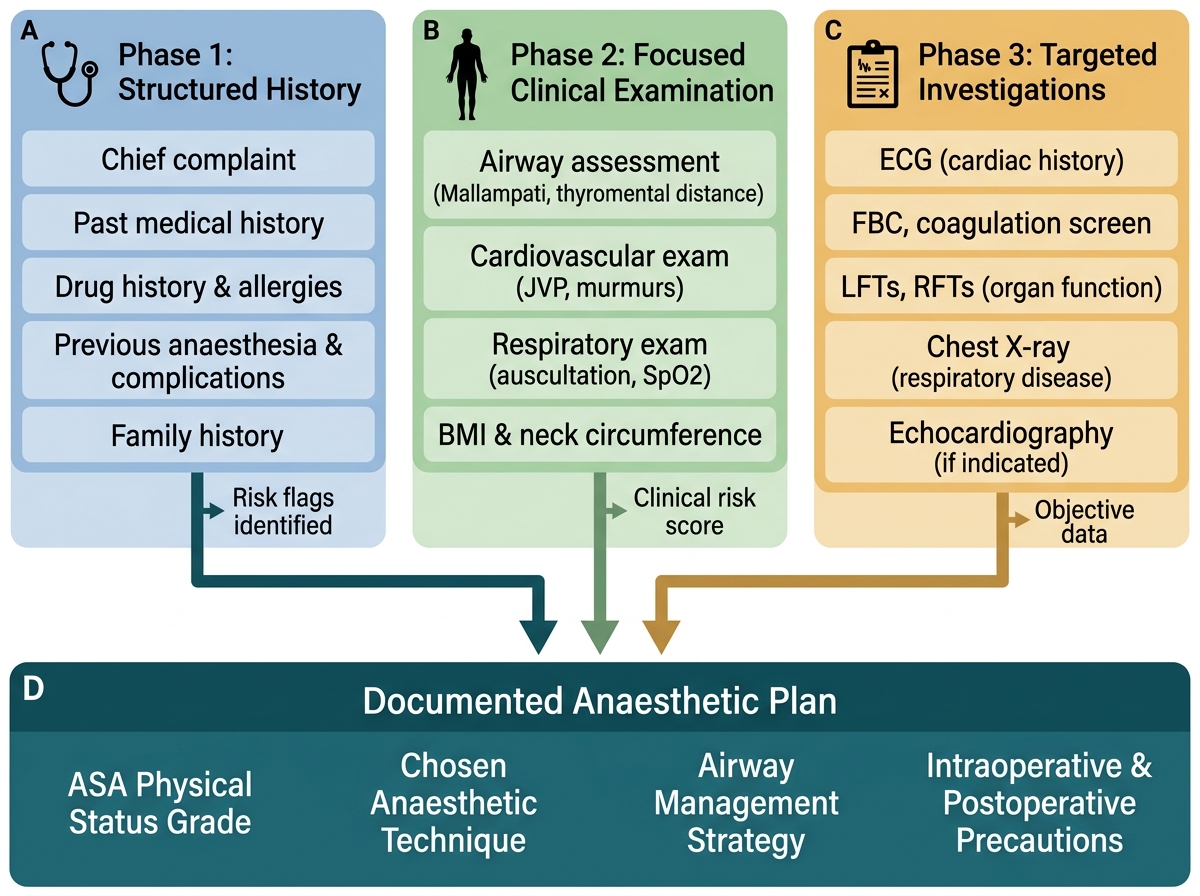
Three-Phase Preoperative Evaluation Framework and the Documented Anaesthetic Plan
Physiological Basis of Anaesthetic Risk
Understanding why certain patient conditions increase anaesthetic risk requires a working knowledge of how anaesthetic drugs and the surgical stress response interact with organ physiology. This section addresses the physiological and pharmacological basis of preoperative risk assessment.
General anaesthesia imposes four major physiological perturbations on every patient: (1) cardiovascular depression — most induction agents (propofol, thiopentone) cause dose-dependent vasodilation and myocardial depression, reducing systemic vascular resistance and cardiac output; in a patient with compromised ventricular function, this can precipitate haemodynamic collapse; (2) respiratory depression — anaesthetic agents blunt the hypoxic and hypercapnic ventilatory drive, necessitating mechanical ventilation; residual neuromuscular blockade in the recovery period can cause upper airway obstruction and hypoventilation, a particular risk in obese patients and those with obstructive sleep apnoea; (3) loss of protective airway reflexes — the cough and swallow reflexes are abolished, creating aspiration risk; this risk is amplified in patients with gastroparesis (as in diabetes mellitus), oesophageal disease, obesity, or acute abdomen where gastric emptying is delayed; (4) thermoregulatory impairment — anaesthetics abolish behavioural and autonomic thermoregulation, leading to hypothermia from radiation and convection in the open abdomen or cold operating theatre; hypothermia in turn causes cardiac arrhythmias, coagulopathy, and delayed drug metabolism.
The surgical stress response compounds these anaesthetic effects. Surgery triggers a catecholamine surge, increased cortisol and glucagon secretion, and a pro-inflammatory cytokine release. In healthy patients this response is self-limiting. In patients with limited cardiac, pulmonary, or renal reserve, the combination of anaesthetic-induced depression and the sympathetic surge of surgical stress can overwhelm organ function, precipitating myocardial ischaemia, heart failure, acute kidney injury, or respiratory failure.
This physiological framework directly explains why the preoperative evaluation focuses on the following high-yield systems: the heart (can it sustain output under anaesthetic depression and surgical stress?), the lungs (can they be mechanically ventilated, and can residual drug be cleared postoperatively?), the kidneys (will drug clearance be prolonged?), the liver (coagulation factor synthesis, drug metabolism), and the airway (can it be secured without difficulty?).
Organ reserve matters more than resting function. A patient with a resting ejection fraction of 45% and no symptoms at rest may decompensate under the combined stress of induction, intubation, and a 3-hour laparotomy. Functional capacity — expressed in metabolic equivalents (METs) — is a more predictive measure of perioperative cardiac risk than resting tests. One MET equals resting oxygen consumption (3.5 mL O2/kg/min). The ability to perform activities requiring 4 METs or more (climbing one flight of stairs, walking briskly on level ground, doing light housework) indicates adequate cardiorespiratory reserve for most non-cardiac surgeries.
Drug interactions and altered pharmacokinetics are a central concern. Patients on MAO inhibitors are at risk of hypertensive crisis with sympathomimetic vasopressors or serotonin syndrome with pethidine. Patients on lithium may have prolonged neuromuscular blockade. Patients on chronic opioids have opioid tolerance and need higher postoperative analgesic doses. These interactions must be identified preoperatively.
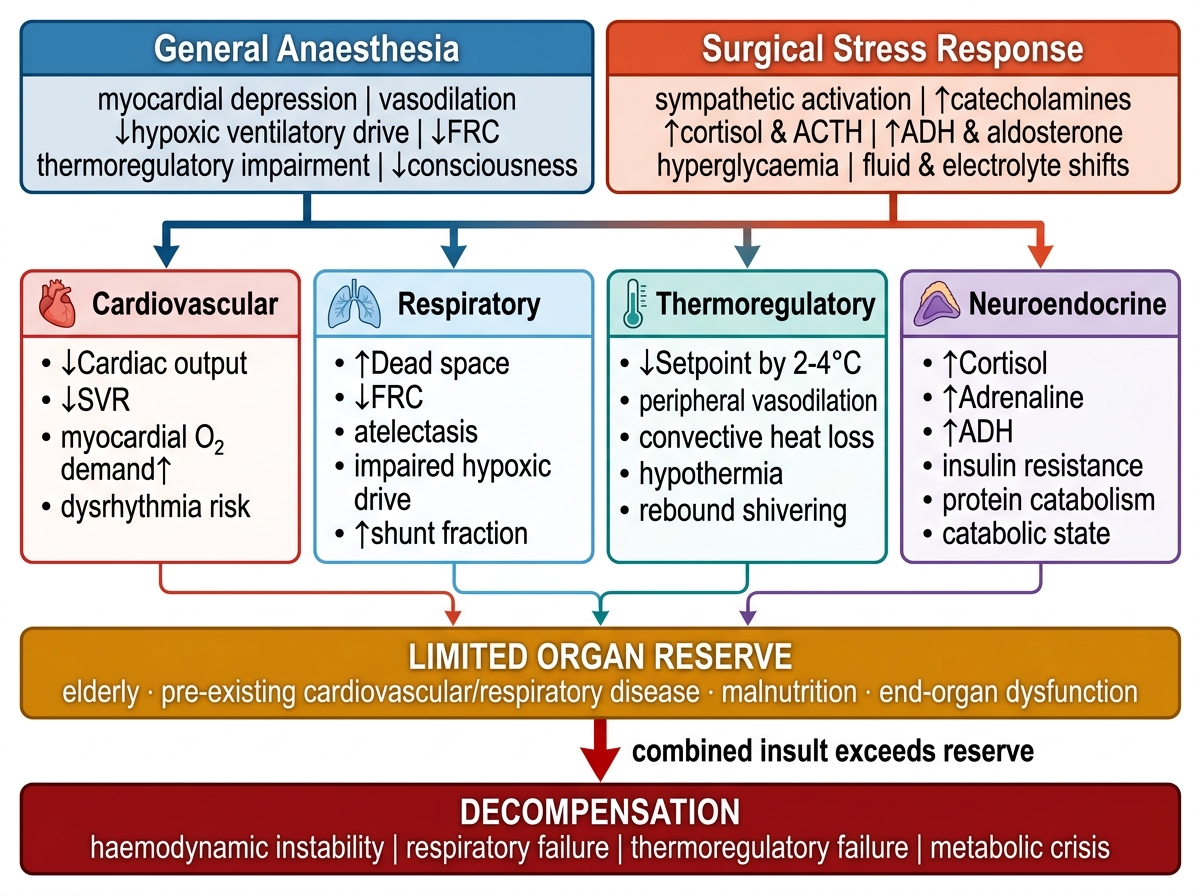
Anaesthesia and Surgical Stress: Converging Insults and the Path to Decompensation
Assessment: History, Examination, and Risk Scoring
The assessment phase of the preoperative evaluation integrates clinical history, physical examination, and risk stratification tools into an overall picture of the patient's perioperative risk. This section covers how to gather, synthesise, and score that information.
The structured history for anaesthetic assessment covers seven domains: (1) Current illness and planned surgery — is the procedure elective, urgent (within 24-48 h), or emergency? The urgency determines how much time is available for optimisation. (2) Anaesthetic history — previous anaesthetics uneventful? Difficult airway? History of PONV, malignant hyperthermia, or pseudocholinesterase deficiency in the patient or family? (3) Surgical history — previous abdominal surgeries affect laparoscopic access; previous spinal surgery affects regional anaesthesia; previous neck surgery affects airway management. (4) Drug history and allergies — name every medication including over-the-counter drugs, herbal preparations, and contraceptives; identify true allergies (anaphylaxis, urticaria) versus adverse effects; specifically ask about anticoagulants, antiplatelets, insulin, and antihypertensives. (5) Medical comorbidities — structured systems review covering cardiac (angina, dyspnoea, orthopnoea, syncope), respiratory (wheeze, nocturnal cough, sleep apnoea), renal (oliguria, dialysis), hepatic (jaundice, ascites), neurological (stroke, seizures), and endocrine (diabetes, thyroid). (6) Functional capacity in METs — 'Can you climb one flight of stairs without stopping?' translates directly to cardiac risk. (7) Social history — smoking (pack-years), alcohol (units/week), recreational drug use.
The clinical examination focuses on four areas. First, airway assessment — the most anaesthesia-specific part of the examination: mouth opening (inter-incisor distance ≥3 finger breadths = adequate), Mallampati class (I-IV, tongue protruded, no phonation), neck mobility (sniffing position), thyromental distance (≥6.5 cm favourable), beard, loose or missing teeth, and body habitus. Second, cardiovascular examination — pulse rate and rhythm, blood pressure in both arms, JVP, apex beat, heart sounds (murmurs by timing/site/radiation), and pedal oedema. Third, respiratory examination — respiratory rate, oxygen saturation on air, chest symmetry, percussion, and auscultation. Fourth, directed systems examination based on history findings.
The Mallampati classification grades the oropharyngeal view: Class I — soft palate, uvula, fauces, and pillars fully visible; Class II — soft palate, uvula, and fauces visible, pillars hidden; Class III — only soft palate and base of uvula visible; Class IV — only hard palate visible. Class III-IV predicts difficult laryngoscopy. Mallampati class is always combined with other predictors (inter-incisor distance, thyromental distance, neck movement) to form a composite airway risk assessment.
Risk stratification tools consolidate clinical findings into actionable scores. The Revised Cardiac Risk Index (RCRI) — also called the Lee index — assigns one point each for: high-risk surgery (intrathoracic, intraabdominal, or suprainguinal vascular), ischaemic heart disease, congestive heart failure, cerebrovascular disease, insulin-dependent diabetes mellitus, and preoperative serum creatinine >177 micromol/L (>2 mg/dL). Predicted MACE risk: RCRI 0 = approximately 0.4%, RCRI 1 = approximately 1%, RCRI 2 = approximately 2.4%, RCRI 3 or more = more than 5%. The RCRI guides the decision about additional cardiac workup before elective surgery.
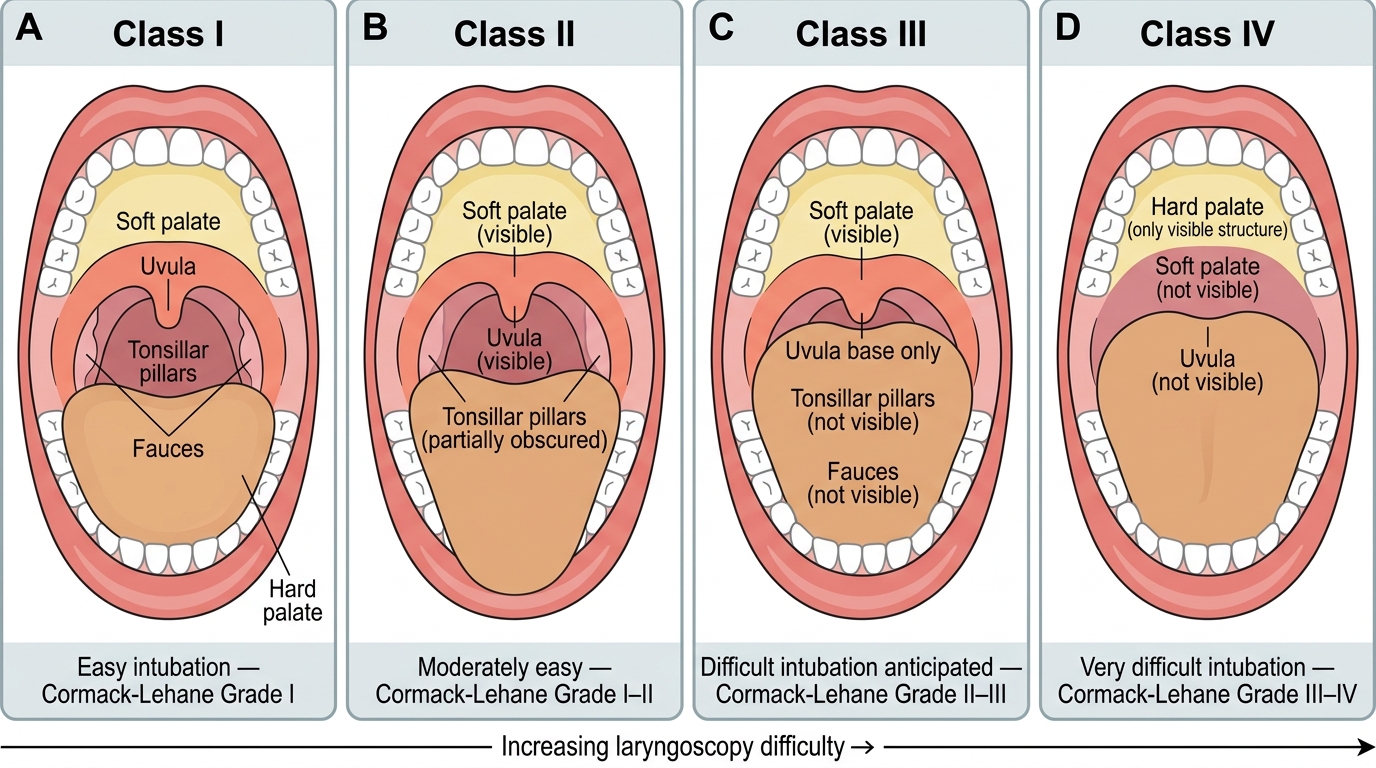
Mallampati Classification: Oropharyngeal Views and Predicted Laryngoscopy Difficulty (Classes I–IV)