Page 13 of 20
AS4.6-7 | Day Care Anaesthesia and Anaesthesia Outside the Operating Room — SDL Guide
CLINICAL SCENARIO
Modern healthcare has moved anaesthesia far beyond the operating theatre. Today, a patient receives propofol sedation for a colonoscopy in the endoscopy unit, undergoes a cardiac catheterisation under conscious sedation in the cath lab, gets a CT scan under general anaesthesia in the radiology department, and — if eligible — has a laparoscopic cholecystectomy and goes home the same afternoon. All of these scenarios share a common challenge: the anaesthetic environment is either temporary (the patient is not staying overnight) or remote from the resources of the main operating theatre, with its immediately accessible equipment, trained personnel, and emergency support systems. In both settings, a systematic approach — careful patient selection, standardised techniques, and structured recovery criteria — is what makes the difference between a safe efficient service and a preventable catastrophe.
WHY THIS MATTERS
AS4.6 requires you to observe and describe the principles and techniques of day care anaesthesia; AS4.7 covers anaesthesia outside the operating room (NORA — non-operating room anaesthesia). Together these two competencies reflect the expanding scope of modern anaesthetic practice. As a graduating doctor, you will encounter sedated and recovering patients in a wide range of settings — the endoscopy suite, the radiology department, the ICU, the emergency department, and the outpatient surgical facility. Understanding the principles of patient selection, fast-track anaesthetic techniques, and the specific hazards of remote locations is essential for safe clinical practice regardless of specialty.
RECALL
Before proceeding, recall: (1) ASA physical status classification I–VI — understanding which patients are suitable for day surgery depends on this; (2) the 2-4-6-8 fasting rule (clear fluids 2 h, breast milk 4 h, light meal 6 h, full meal 8 h); (3) propofol's key properties — rapid onset, smooth emergence, antiemetic effect, absence of hangover — which make it the cornerstone of day surgery anaesthesia; (4) PONV risk factors and prophylaxis (ondansetron, dexamethasone) since PONV is the leading cause of unanticipated admission after day surgery; (5) the Aldrete score for PACU discharge readiness.
Clinical Context and Indications: Why Day Care Anaesthesia?
Day care anaesthesia (day surgery, ambulatory anaesthesia) refers to planned surgical or procedural care in which the patient is admitted, receives anaesthesia, undergoes the procedure, and is discharged home on the same calendar day — without an overnight hospital stay. This model of care has expanded dramatically over the past three decades, driven by advances in short-acting anaesthetic agents (propofol, remifentanil, desflurane, sugammadex), minimally invasive surgical techniques, and evidence that carefully selected patients recover better in their home environment than in hospital wards.
The clinical rationale for day surgery is compelling from multiple perspectives. From the patient's perspective: reduced risk of hospital-acquired infection, preservation of normal sleep/eating patterns, psychological comfort of familiar surroundings, and faster return to normal function. From the healthcare system's perspective: reduced inpatient bed consumption, increased surgical throughput, and significant cost savings. From the anaesthesiologist's perspective: the constraints of day surgery — no overnight nursing observation, no ICU backup, limited rescue options if complications arise — mean that patient selection and technique selection must be more rigorous than for inpatient surgery. The imperative to do the case safely within the day-surgery framework, and not to compromise safety for throughput, is the defining clinical and ethical tension in this practice.
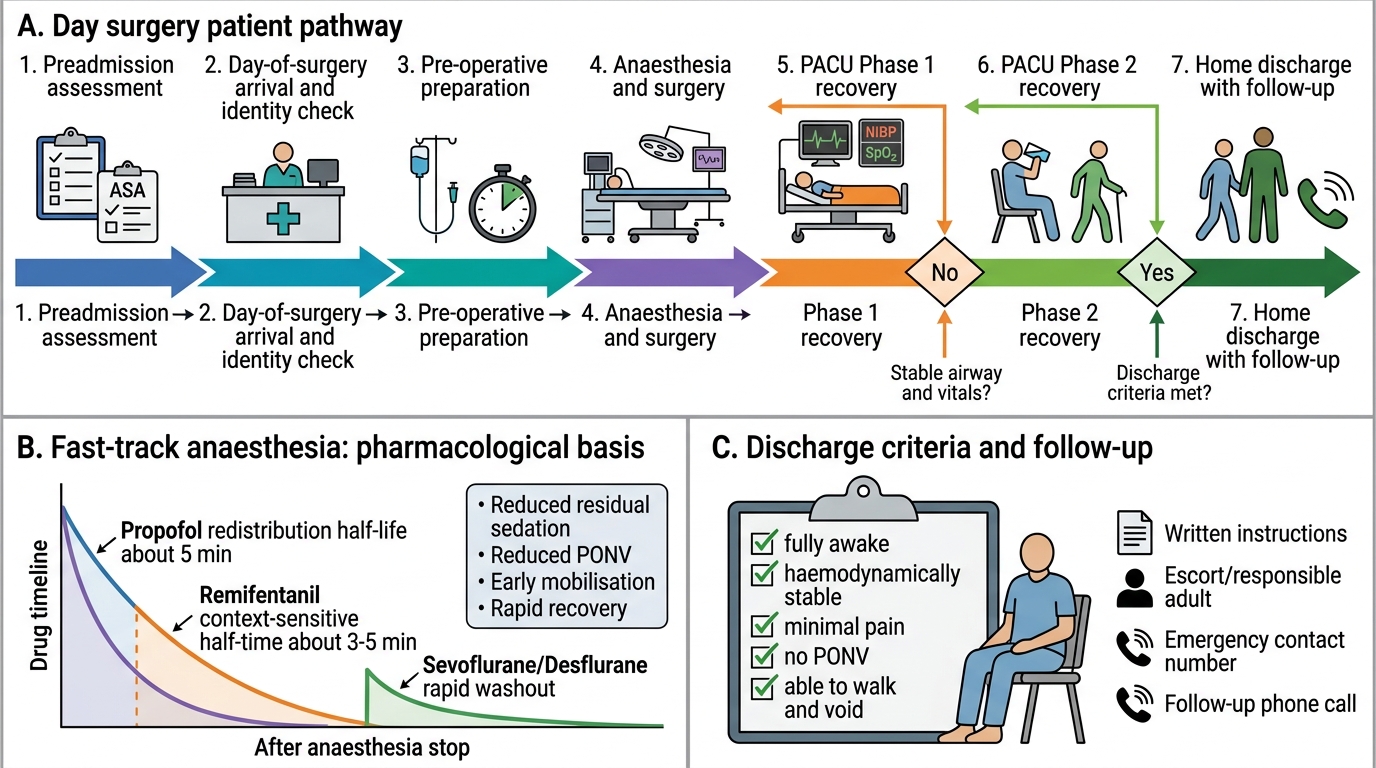
Day Surgery Patient Pathway and Fast-Track Anaesthesia
Physiological and Pharmacological Basis: Fast-Track Anaesthesia
The pharmacological foundation of day surgery anaesthesia is the concept of fast-track or enhanced recovery: techniques that minimise residual drug effects at the time of discharge, enabling patients to meet discharge criteria (fully awake, haemodynamically stable, minimal pain, no PONV, able to walk and void) within 2–4 hours of the procedure. This requires a fundamentally different pharmacological approach from inpatient anaesthesia, where residual sedation or nausea can simply be managed on the ward overnight.
The key pharmacokinetic requirement is short context-sensitive half-time — drugs that are metabolised or redistributed rapidly so that their clinical effect dissipates quickly and predictably after the infusion or dose is stopped. Propofol meets this criterion admirably: its clinical half-life after a single bolus is ~5 minutes (redistribution), and even after a prolonged infusion the context-sensitive half-time at clinically relevant concentrations remains short enough for same-day discharge. Remifentanil (ester hydrolysis, context-sensitive half-time ≈3–5 minutes regardless of infusion duration) is the opioid partner of choice for TIVA in day surgery. Volatile agents sevoflurane and desflurane have low blood-gas partition coefficients enabling rapid emergence — comparable to propofol TIVA for most day surgery cases.
Multimodal analgesia — combining paracetamol, NSAIDs (ibuprofen, ketorolac), local anaesthetic infiltration, and opioid only as rescue — minimises the sedation, nausea, and respiratory depression that opioid-heavy regimens produce. Reducing opioid consumption is one of the most effective single strategies for enabling fast-track discharge.
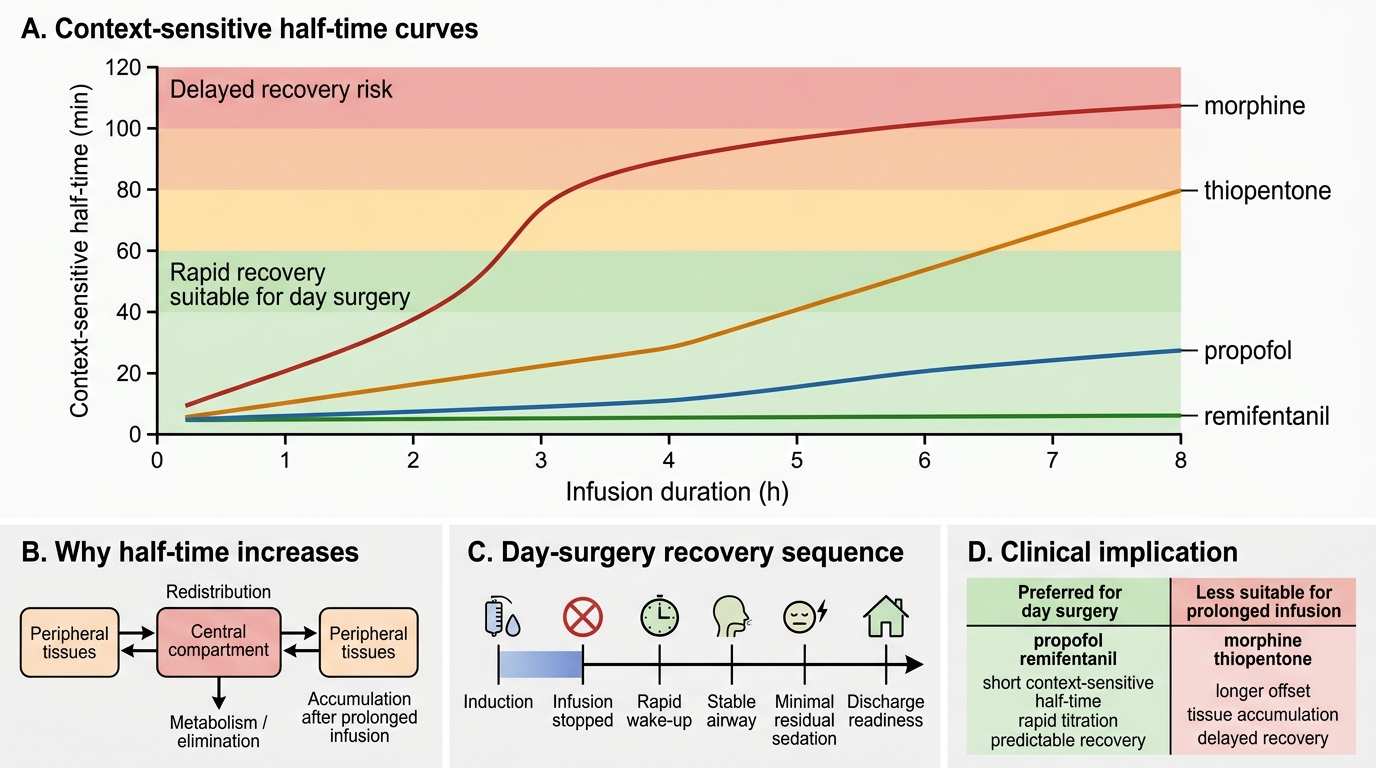
Context-Sensitive Half-Time and Day-Surgery Drug Choice
Assessment and Planning: Patient Selection for Day Surgery
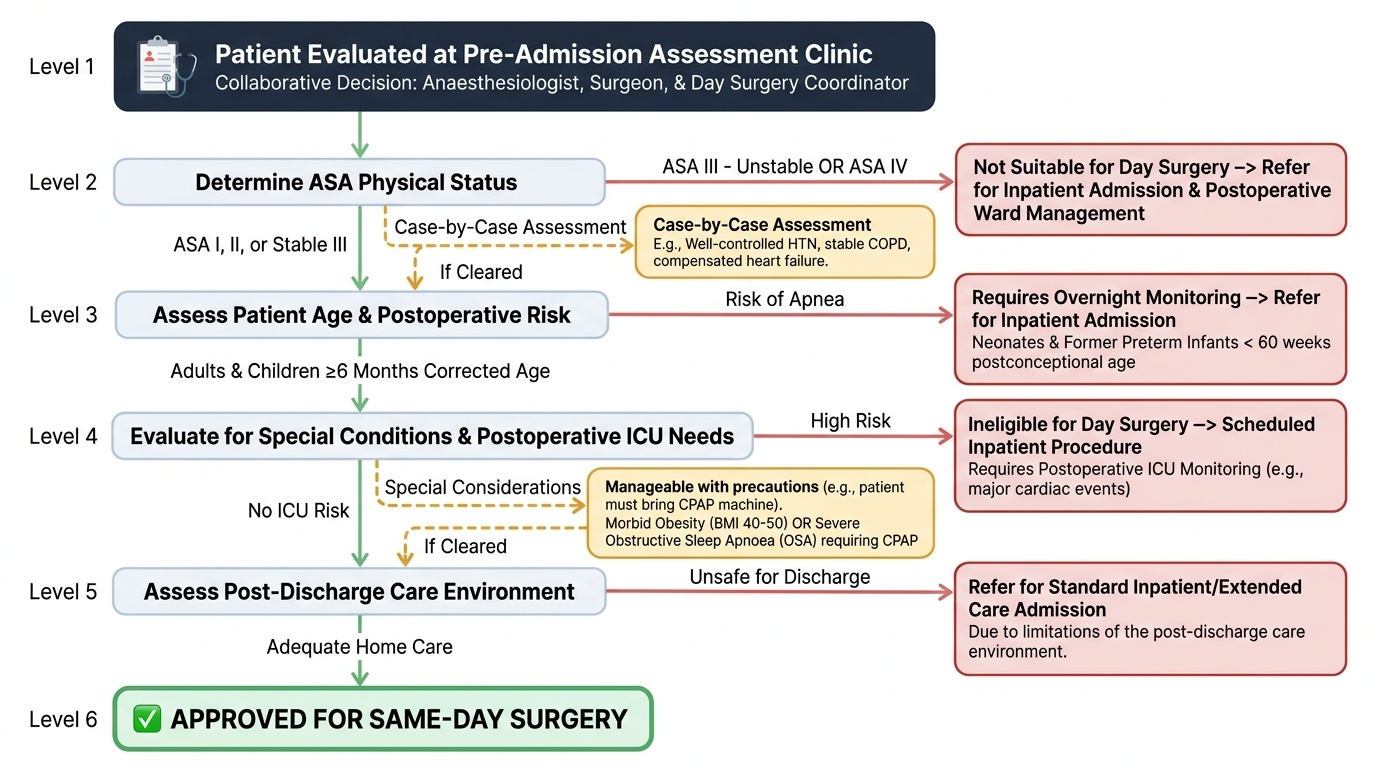
Appropriate patient selection is the single most important determinant of safe day surgery outcomes. Not every patient or procedure is suitable for same-day discharge, and the consequences of a wrong selection decision can be serious and medico-legally significant: an unanticipated admission requiring unplanned ward management, postoperative complications occurring at home without adequate nursing supervision, or a patient presenting to an emergency department at midnight with uncontrolled pain or haemorrhage. The anaesthesiologist shares responsibility for the selection decision with the surgeon and the day surgery unit coordinator — the pre-admission assessment clinic is the correct place to identify and resolve concerns, not the morning of surgery. Patient selection criteria must balance the genuine benefits of ambulatory care (reduced infection risk, patient preference, cost savings) against the risks imposed by the patient's comorbidities, the physiological demands of the planned procedure, and the limitations of the post-discharge care environment.
Provided image
General patient selection criteria for day surgery:
- ASA status I–III stable (ASA IV or unstable ASA III are generally not suitable for day surgery; some ASA III patients with well-controlled stable disease — e.g., well-controlled hypertension, stable COPD, compensated heart failure — are acceptable after case-by-case assessment)
- Adult patients: generally suitable; paediatric day surgery is well established for children ≥6 months corrected age; neonates and former preterm infants (<60 weeks postconceptional age) have apnoea risk postoperatively and require overnight monitoring
- No conditions requiring postoperative ICU monitoring — major cardiac events, severe obstructive sleep apnoea requiring CPAP (relative contraindication — can be managed with CPAP machine brought by patient), morbid obesity (BMI >40–50 is a relative contraindication for many units)
- Social suitability: responsible adult escort home and to stay with patient for 24 hours; phone access; ability to return to hospital within acceptable time if complication arises
- Procedure suitability: expected surgical time <2 hours for most day surgery units; procedure with predictable blood loss (not requiring transfusion); procedure not requiring prolonged immobility or complex wound care
Specific conditions requiring special consideration:
- Obstructive sleep apnoea (OSA): increased sensitivity to opioids and sedatives; postoperative apnoea risk; regional and local anaesthetic techniques preferred; multimodal analgesia minimising opioids; extended PACU observation; OSA STOP-Bang score ≥5 warrants caution
- Diabetes: early listing on surgical list preferred to minimise fasting hypoglycaemia; check blood glucose pre- and post-procedure; omit morning oral hypoglycaemics and long-acting insulin on day of surgery
- Hypertension: well-controlled hypertension is acceptable; systolic >180 or diastolic >110 on day of surgery may warrant postponement