Page 1 of 20
AS4.1 | Pharmacology of Drugs Used in General Anaesthesia — SDL Guide
CLINICAL SCENARIO
A 45-year-old man is brought to the operating theatre for an emergency laparotomy. Within minutes of induction, the anaesthesiologist must select agents to render the patient unconscious, paralysed, and insensitive to pain — and then maintain that state safely for two hours while vigilantly managing his physiology. Every drug chosen has a precise pharmacological rationale: its onset, duration, site of action, and adverse-effect profile determine whether the patient wakes up smoothly or encounters a life-threatening complication. Understanding this pharmacology is not an academic exercise — it is the mechanistic basis of every anaesthetic decision made at the table.
WHY THIS MATTERS
AS4.1 asks you to describe and discuss the full pharmacological spectrum of agents used in general anaesthesia: intravenous and inhalational induction agents, opioid and non-opioid analgesics, depolarising and non-depolarising muscle relaxants, and anticholinesterases. This SDL equips you to understand the why behind clinical choices — why propofol is preferred over thiopentone in most elective cases, why suxamethonium remains irreplaceable for rapid-sequence induction despite its adverse-effect profile, and why neostigmine must always be paired with an anticholinergic. This underpins everything from safe drug administration to recognising and managing complications such as malignant hyperthermia.
RECALL
Before proceeding, recall the following concepts from pharmacology and physiology: (1) the mechanism of the neuromuscular junction — acetylcholine released from motor nerve terminals binds nicotinic receptors on the motor end-plate to produce depolarisation and muscle contraction; (2) how ionisation and lipid solubility govern a drug's ability to cross the blood-brain barrier; (3) the concept of minimum alveolar concentration (MAC) as a measure of inhalational agent potency; (4) the pharmacokinetic concepts of redistribution (explains why thiopentone's clinical effect is short despite a long elimination half-life) and context-sensitive half-time (why propofol infusions are more predictable than thiopentone infusions for maintenance).
Intravenous Induction Agents
Intravenous induction agents are highly lipid-soluble drugs administered as a bolus to produce rapid loss of consciousness, typically within one arm-brain circulation time (approximately 30 seconds). The speed and quality of induction, as well as the subsequent recovery profile, are determined by each drug's pharmacokinetic and pharmacodynamic properties. Understanding these differences is essential for choosing the appropriate agent for any given clinical context.
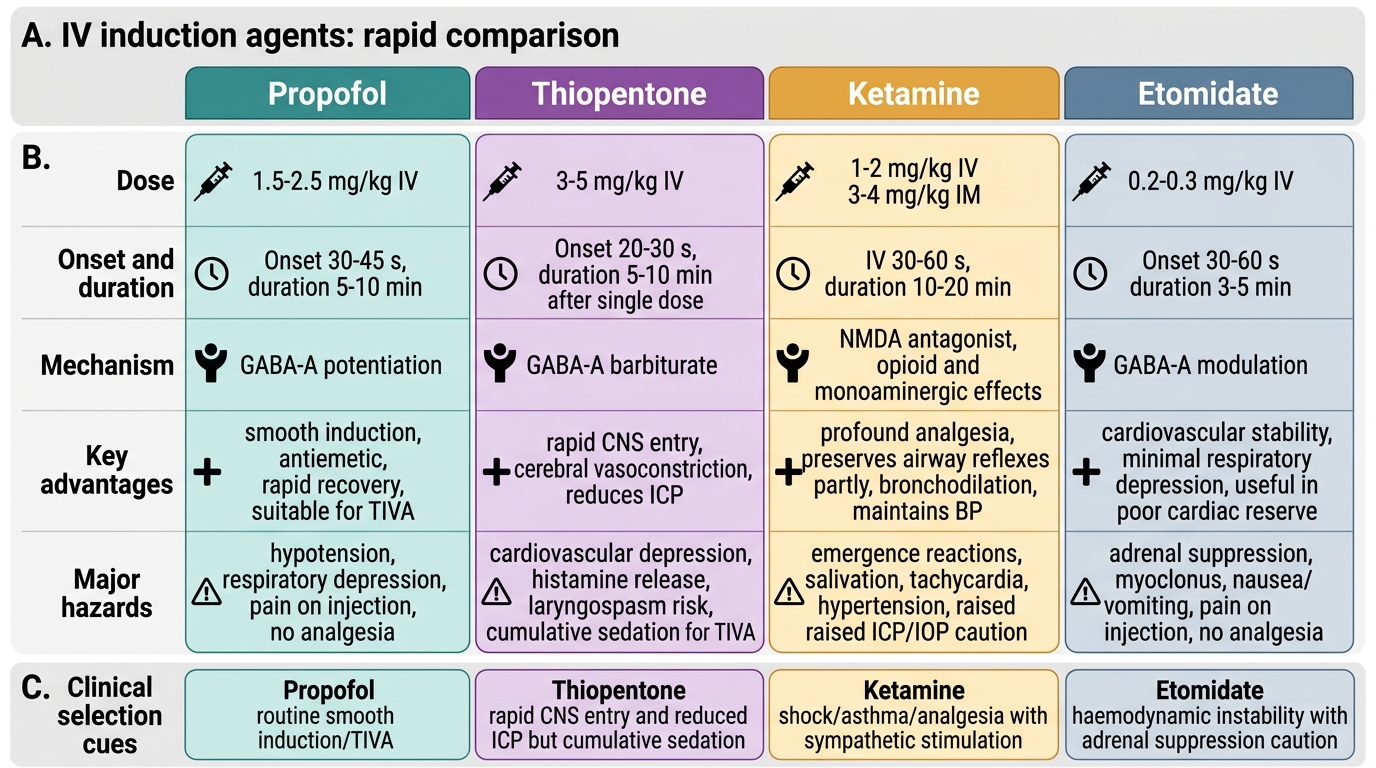
Propofol (2,6-diisopropylphenol) is the most widely used induction agent today. It is administered intravenously at a dose of 1.5–2.5 mg/kg (lower doses in elderly or haemodynamically compromised patients, higher in anxious or robust patients). Propofol potentiates GABA-A receptor activity, enhancing chloride conductance and suppressing neuronal excitability. Its key advantages include smooth, rapid induction and an exceptionally pleasant emergence without hangover, nausea, or dysphoria — a property linked to its antiemetic effects, possibly mediated by dopamine D2 receptor antagonism. On the debit side, propofol causes dose-dependent cardiovascular depression: systemic vascular resistance falls, cardiac output decreases, and blood pressure drops — particularly pronounced in elderly, hypovolaemic, or cardiac patients. It also produces pain on injection (mitigated by prior lidocaine 20–40 mg or choosing a larger antecubital vein). Propofol is presented as a 1% or 2% emulsion in soybean oil and egg lecithin — a contraindication in egg-phospholipid allergy (soy allergy alone is not an absolute contraindication per current evidence). It can be used for both induction and total intravenous anaesthesia (TIVA) maintenance by continuous infusion.
Comparison of IV Induction Agents
Thiopentone (sodium thiopentone, a barbiturate) was the gold standard for decades; its dose is 3–5 mg/kg IV. Like propofol, it acts at GABA-A receptors. Its speed of action is due to high lipid solubility allowing rapid CNS entry; termination of effect is by redistribution from brain to skeletal muscle and fat (not by metabolism), so repeated doses cause cumulative sedation. Thiopentone is a potent cerebral vasoconstrictant and reduces ICP, making it historically useful in neuroanaesthesia. However it causes laryngeal sensitivity (pharyngeal reflexes are heightened just before unconsciousness, predisposing to laryngospasm), it is a significant cardiovascular depressant, and it causes histamine release. It cannot be used for TIVA. Because of supply issues and the superiority of propofol for most purposes, thiopentone use has declined markedly.
Ketamine is a phencyclidine derivative that produces dissociative anaesthesia — a trancelike cataleptic state with profound analgesia, amnesia, and immobility while pharyngeal reflexes may remain partially intact. The dose for induction is 1–2 mg/kg IV (3–4 mg/kg IM for uncooperative patients or paediatric use). Ketamine is a non-competitive NMDA receptor antagonist and also acts at opioid receptors and monoaminergic systems. Its unique haemodynamic profile is one of sympathomimetic stimulation: heart rate, blood pressure, and cardiac output all increase, making ketamine the induction agent of choice in haemodynamically unstable or hypovolaemic patients (e.g., trauma, septic shock). It is also a potent bronchodilator, ideal for asthmatic patients requiring emergency anaesthesia. Critical contraindications or cautions: ketamine raises ICP and intraocular pressure — it must be used with extreme caution (or avoided) in head injury, intracranial hypertension, or open-eye injury. It produces psychotomimetic emergence reactions (vivid dreams, hallucinations), mitigated by co-administering a benzodiazepine. Salivation is increased — use with an anticholinergic.
Etomidate is an imidazole derivative producing rapid unconsciousness at 0.2–0.3 mg/kg IV. Its defining feature is cardiovascular stability — it produces minimal change in heart rate, blood pressure, or myocardial contractility, making it preferred in patients with severe cardiac disease. However, etomidate suppresses adrenocortical function by inhibiting 11β-hydroxylase — a single induction dose can cause 24 hours or more of cortisol suppression, which is clinically significant in critically ill patients. It frequently causes involuntary myoclonic movements and moderate pain on injection. Because of adrenal suppression, etomidate is generally avoided for prolonged infusion or in septic patients.
Inhalational Anaesthetic Agents
Inhalational agents are volatile liquids or gases used to maintain (and sometimes induce) general anaesthesia. Their potency is measured by the minimum alveolar concentration (MAC) — defined as the alveolar concentration of anaesthetic at which 50% of patients do not move in response to a standard surgical stimulus (skin incision) at 1 atmosphere of pressure. A lower MAC means a more potent agent.
Provided image
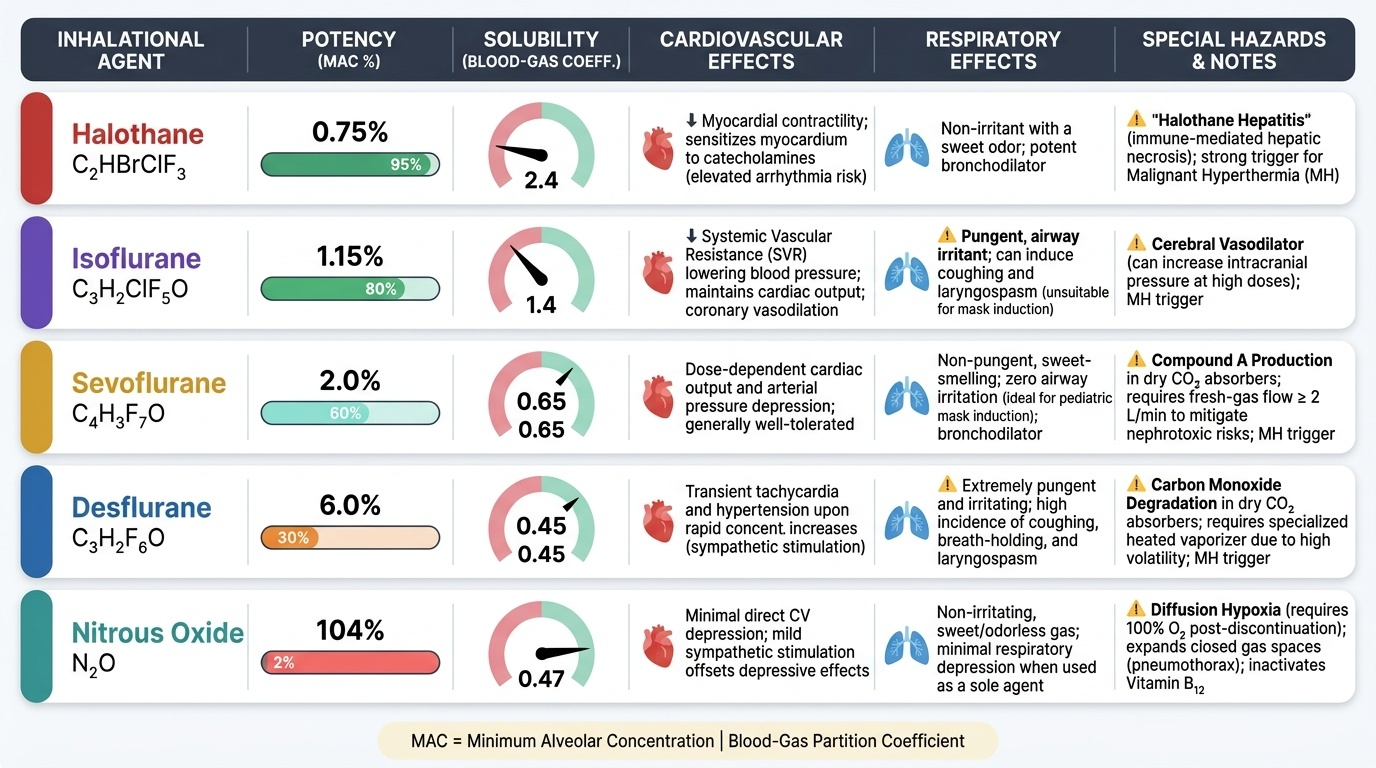
The mechanism of action of inhalational agents is not fully established, but GABA-A receptor potentiation, glycine receptor modulation, and inhibition of NMDA receptors all contribute. The rate of onset and offset of inhalational agents depends critically on the blood-gas partition coefficient: a low value means the agent is relatively insoluble in blood, so alveolar concentration equilibrates quickly with blood, enabling rapid induction and rapid elimination. This is why desflurane (blood-gas partition coefficient 0.45) and sevoflurane (0.65) produce faster, smoother emergence than isoflurane (1.4) or halothane (2.4).
Sevoflurane is the most widely used agent for both paediatric inhalational induction (sweet, non-pungent smell; no breath-holding or laryngospasm) and adult maintenance. MAC is 2.0–2.5% (in oxygen). It produces dose-dependent cardiovascular and respiratory depression but is generally well tolerated. Sevoflurane is metabolised to fluoride ions and compound A (a nephrotoxic degradation product with soda-lime/barium lime absorbers) — clinically significant nephrotoxicity at low fresh-gas flows has been debated, but clinical practice recommends maintaining adequate fresh-gas flow (≥2 L/min with sevoflurane).
Isoflurane has a higher blood-gas partition coefficient (1.4), producing slower emergence than sevoflurane. MAC = 1.15%. It is an excellent cerebral vasodilator and was once the agent of choice in neuroanaesthesia. It is pungent, causing cough and laryngospasm — unsuitable for inhalational induction. Desflurane has the lowest blood-gas solubility among the halogenated agents, enabling very fast emergence — useful in day surgery. However, it is profoundly pungent and is an airway irritant, making inhalational induction impossible; it requires a heated vaporiser because of its low boiling point (23.5°C). Desflurane has significant environmental impact (high global warming potential).
Nitrous oxide (N₂O) is an inorganic gas (MAC ≈ 105% — it cannot produce surgical anaesthesia alone at atmospheric pressure) used as a carrier gas and analgesic adjunct. It reduces the required concentration of potent agents (the second-gas effect). Its mechanism includes NMDA receptor antagonism. Critical hazards: N₂O is 34× more soluble in blood than nitrogen and diffuses into air-filled cavities — it causes expansion of pneumothorax, bowel loops, middle ear, and intravascular air emboli. It is absolutely contraindicated in intestinal obstruction, pneumothorax, severe bullous disease, and after eye surgery with gas tamponade. Prolonged or repeated exposure inhibits methionine synthase (vitamin B₁₂-dependent enzyme) and impairs DNA synthesis — an occupational hazard requiring trace-gas scavenging.
Halothane, now largely replaced in high-income settings but still used in some resource-limited contexts, carries the rare but serious complication of halothane hepatitis (immune-mediated, incidence 1:35,000; fulminant hepatic necrosis). Halothane sensitises the myocardium to catecholamines, predisposing to ventricular arrhythmias — epinephrine doses must be strictly limited during halothane anaesthesia.
Opioid and Non-Opioid Analgesics in General Anaesthesia
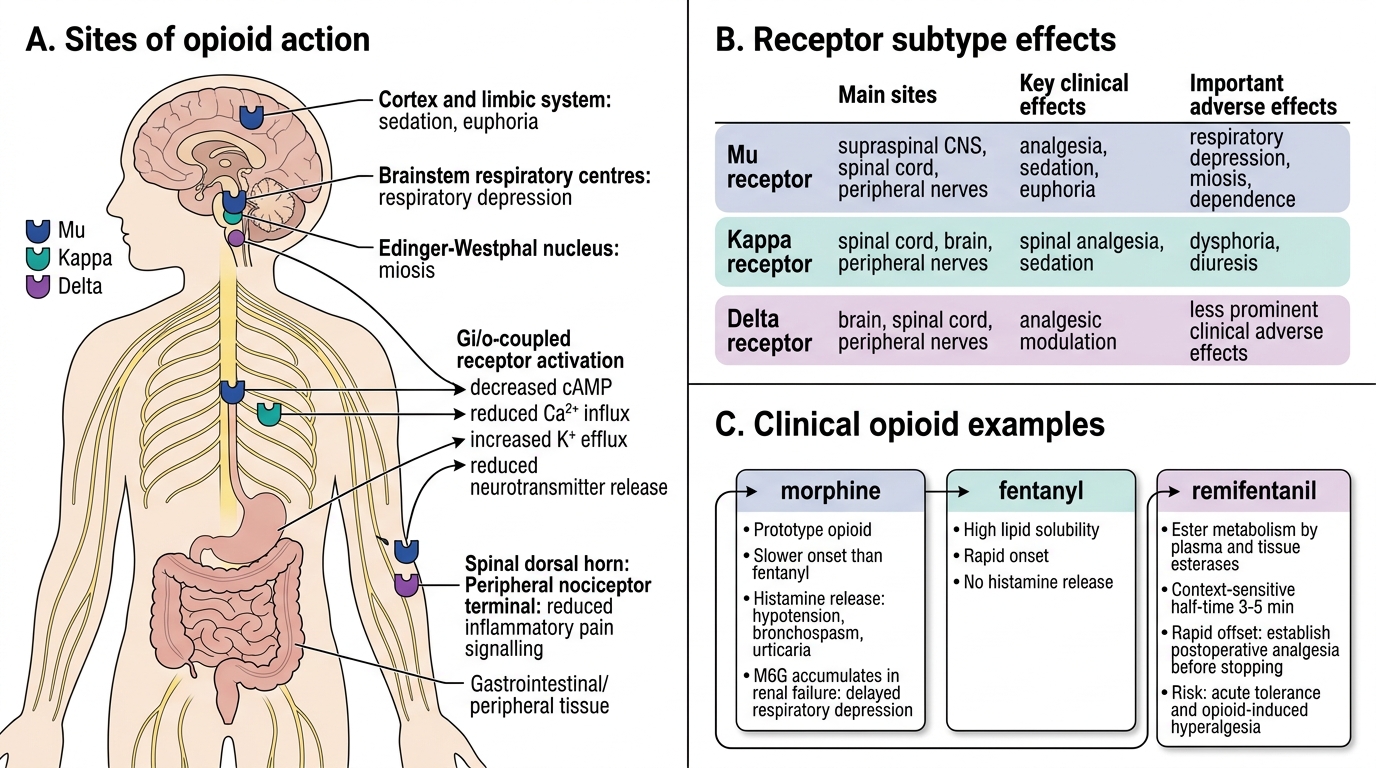
Opioids are essential components of balanced anaesthesia, reducing the requirement for induction and maintenance agents, attenuating the haemodynamic stress response to laryngoscopy and surgical stimulation, and providing intraoperative and postoperative analgesia. They act primarily at mu (μ), kappa (κ), and delta (δ) opioid receptors — mu receptors mediate the predominant analgesic, euphoric, and respiratory-depressant effects.
Fentanyl is the most widely used intraoperative opioid. It is a synthetic phenylpiperidine with high lipid solubility and rapid onset. For induction analgesia it is typically given at 1–3 mcg/kg IV; continuous intraoperative infusion of 1–3 mcg/kg/hour is common. Its duration of action after a single bolus is 30–60 minutes (primarily by redistribution). A major advantage of fentanyl over morphine is minimal histamine release and haemodynamic stability at routine doses. Respiratory depression is the principal hazard — fentanyl reduces respiratory rate and tidal volume; the dose-response relationship is steep, particularly in opioid-naive patients.
Opioid Receptor Subtypes: Sites, Effects, and Clinical Examples
Morphine is the prototype opioid and reference standard. It has a slower onset than fentanyl because of lower lipid solubility. Unlike fentanyl, morphine releases histamine from mast cells — this can cause hypotension, bronchospasm, and urticaria, limiting its use as an induction bolus. However, its longer duration of action makes it useful for postoperative analgesia. Active metabolite morphine-6-glucuronide (M6G) provides prolonged analgesia but can accumulate in renal failure, causing delayed respiratory depression.
Remifentanil is an ultra-short-acting opioid ester metabolised by non-specific plasma and tissue esterases — its context-sensitive half-time is consistently 3–5 minutes regardless of infusion duration, a pharmacokinetic property unique among opioids. This makes remifentanil ideal for procedures requiring intense short-duration analgesia (e.g., laryngoscopy, sternotomy) and for TIVA where rapid offset is needed (e.g., awake fibreoptic intubation, neurological monitoring). A critical pitfall is acute opioid tolerance and opioid-induced hyperalgesia with prolonged high-dose infusion — and its very rapid offset means post-infusion analgesia must be established before discontinuation.
Non-opioid analgesics used adjunctively in general anaesthesia include: paracetamol (IV or oral; central cyclooxygenase inhibition, reduces opioid requirement by 20–30% as part of multimodal analgesia); NSAIDs (ketorolac, diclofenac — peripheral COX inhibition, anti-inflammatory, useful for orthopaedic and visceral pain; caution with renal impairment, peptic ulcer disease, platelet effects); ketamine at sub-anaesthetic doses (0.1–0.5 mg/kg as an analgesic adjunct — NMDA blockade attenuates central sensitisation; reduces opioid consumption); and dexmedetomidine (alpha-2 adrenergic agonist, sedation + analgesia + sympatholysis without respiratory depression, often used as an adjunct in intensive care or as an opioid-sparing agent intraoperatively).