Page 9 of 17
AS5.5 | Caudal Epidural Technique in Adults and Children — SDL Guide
CLINICAL SCENARIO
A three-year-old child is scheduled for a unilateral inguinal hernia repair. After inhalational induction of general anaesthesia, the anaesthetist inserts a 22G needle through the sacrococcygeal membrane in under 90 seconds. Three minutes later, 0.7 mL/kg of 0.25% bupivacaine has been deposited into the caudal epidural space. The child wakes up from anaesthesia comfortable, with no crying, no request for analgesia, and is discharged two hours later. In paediatric surgery, the caudal epidural block is so reliable and so transformative that it is the most commonly performed regional technique in children worldwide. In adults, the caudal route provides sacral and low lumbar epidural access with unique indications — particularly for perianal, perineal, and lower sacral surgery. This SDL covers the anatomy, technique, and applied practice for caudal epidural in both populations (AS5.5).
WHY THIS MATTERS
The caudal epidural block exploits a natural opening in the sacrum — the sacral hiatus — to enter the epidural space from below, avoiding the lumbar approach entirely. For paediatric anaesthesia, understanding caudal technique is not optional: it is the foundational regional skill, taught before any other block, because the anatomy is consistent, the failure rate is low, and the benefit-to-risk ratio is excellent. For adult practice, knowing the anatomy and indications of the caudal route expands the anaesthetist's toolkit for sacral pain, coccydynia, and surgery on the perineum where lumbar neuraxial block may be technically difficult or produce an unnecessarily high level. This SDL prepares the student to observe and describe caudal block with full understanding of what is being done and why.
RECALL
Recall the following before proceeding:
- Sacral anatomy: the sacrum is a triangular fusion of S1–S5 vertebrae; the sacral canal is the continuation of the spinal canal into the sacrum; the sacral hiatus is an opening in the posterior wall of the sacrum at S4–S5 level, covered by the sacrococcygeal membrane.
- Epidural space anatomy: extends from the foramen magnum to the sacral hiatus; contains fat, veins, and nerve roots; targeted by epidural injection at all spinal levels.
- LA pharmacology: bupivacaine 2 mg/kg maximum dose; lignocaine 3 mg/kg plain / 7 mg/kg with adrenaline; LAST management with 20% intralipid.
- Paediatric dose calculations: unlike adults, paediatric caudal volumes are weight-based — understanding that LA doses in children are weight-dependent and that underdosing and overdosing carry different risks.
Clinical Indication and Relevance of Caudal Epidural Block
The caudal epidural block is a neuraxial technique that targets the sacral and low lumbar nerve roots by depositing local anaesthetic in the epidural space via the sacral hiatus. It occupies a unique niche: it accesses the epidural space from its most inferior end, making it particularly suited to surgical and analgesic indications in the sacral and lower lumbar dermatomes.
In paediatric practice, the caudal block is the most widely used regional technique in children under 8 years, primarily as an adjunct to general anaesthesia for postoperative pain control. The primary indication is any surgery below the umbilicus performed under general anaesthesia, including: inguinal herniotomy, orchidopexy, circumcision, hypospadias repair, anal fistula repair, lower limb orthopaedic procedures, and sacral skin lesion excision. The block dramatically reduces or eliminates postoperative crying, reduces opioid requirements, lowers emergence agitation, and enables day-surgery. In children under 1 year, caudal morphine (preservative-free) can provide extended analgesia for major abdominal and thoracic surgery, although this requires postoperative monitoring for respiratory depression.
Posterior Sacral Anatomy for Caudal Epidural Block
In adult practice, the caudal route is used less frequently than lumbar or thoracic epidural, but has specific indications:
- Perianal and perineal surgery (haemorrhoidectomy, anal fissure repair, pilonidal sinus) — sacral dermatome coverage without unnecessary lumbar block.
- Coccydynia and sacral pain syndromes — caudal steroid injections (methylprednisolone or triamcinolone with LA) are a common pain management intervention.
- Failed lumbar epidural — when the lumbar epidural space is inaccessible due to previous surgery, calcified ligamentum flavum, or severe scoliosis, the caudal route may succeed.
- Paediatric surgeons in low-resource settings — where ultrasound-guided caudal is performed as the sole anaesthetic for older children or short procedures.
The primary limitation in adults is anatomical variability: the sacral hiatus is impalpable or absent in 5–10% of adults due to sacral fusion or sacral bone spur formation, making the block impossible or unsafe by landmark technique alone.
Anatomy of the Sacrum and Sacral Hiatus
Mastery of caudal block begins with a thorough understanding of sacral anatomy, because every step of the technique — from patient positioning to needle angle to depth estimation — is governed by the bony landmarks of the sacrum and coccyx.
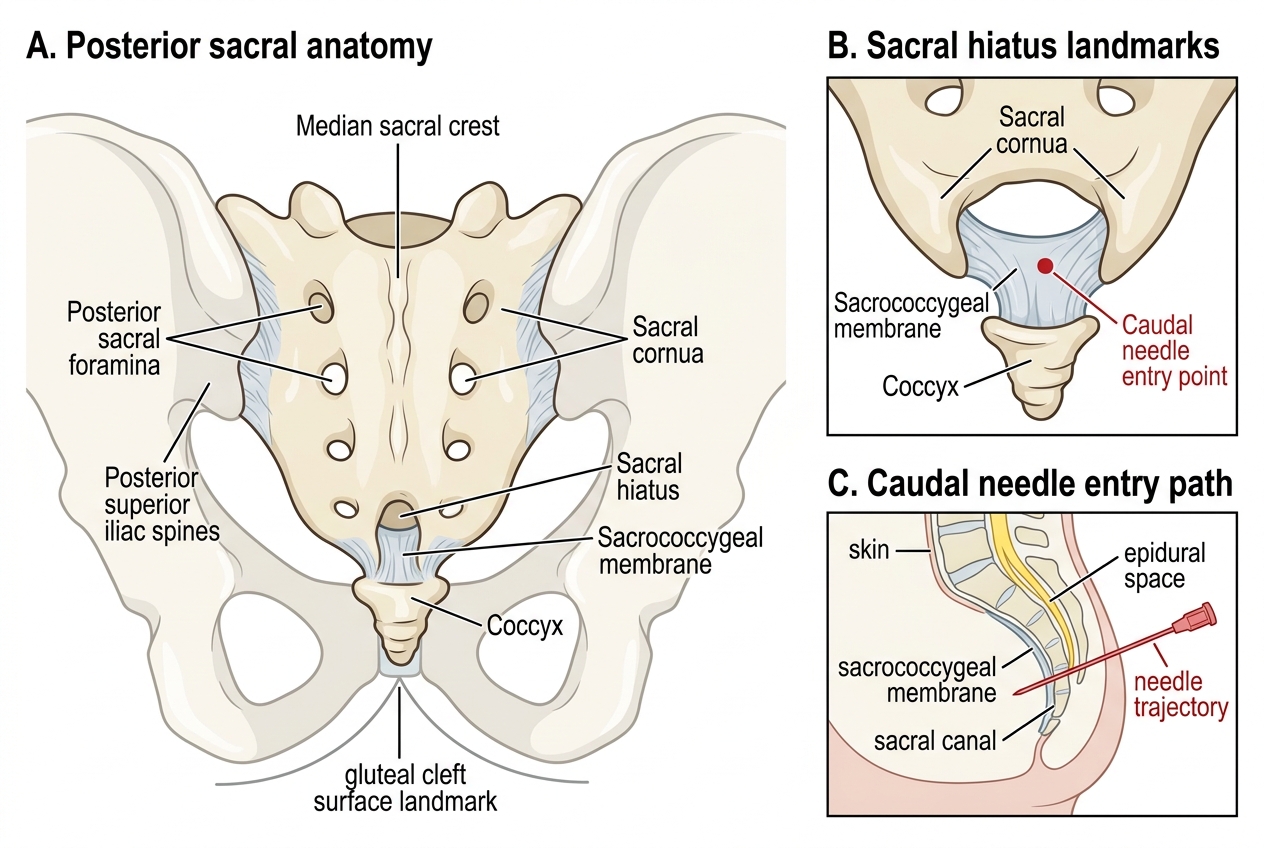
The sacrum is a triangular bone formed by the fusion of the five sacral vertebrae (S1–S5). Its posterior surface has a midline ridge (the median sacral crest — fused spinous processes) flanked by the posterior sacral foramina (for S1–S4 nerve roots) and the sacral cornua — paired bony prominences at the inferior tip of the sacrum that represent the rudimentary inferior articular processes of S5. The sacral canal is the continuation of the spinal canal within the sacrum, containing the terminal dural sac (which ends at S2 in adults, at S3 in neonates — an important safety detail), the sacral and coccygeal nerve roots, the filum terminale, and the caudal epidural venous plexus.
The sacral hiatus is a U- or V-shaped opening in the posterior wall of the sacral canal at the level of S4–S5, formed by the failure of the S4 laminae to fuse in the midline. It is bounded laterally by the sacral cornua and covered posteriorly by the sacrococcygeal membrane — a fibrous sheet analogous to the ligamentum flavum at other levels. This membrane is the target of caudal needle penetration. In children, the sacral hiatus is easily palpable, the sacrococcygeal membrane is thin and offers a clear "pop" on needle penetration, and the angle of the sacral canal is relatively shallow. In adults, the hiatus may be deeper, narrowed, or partially fused, and the overlying fat makes palpation less reliable.
Caudal Epidural Block: Sacral Anatomy and Dural Sac Safety
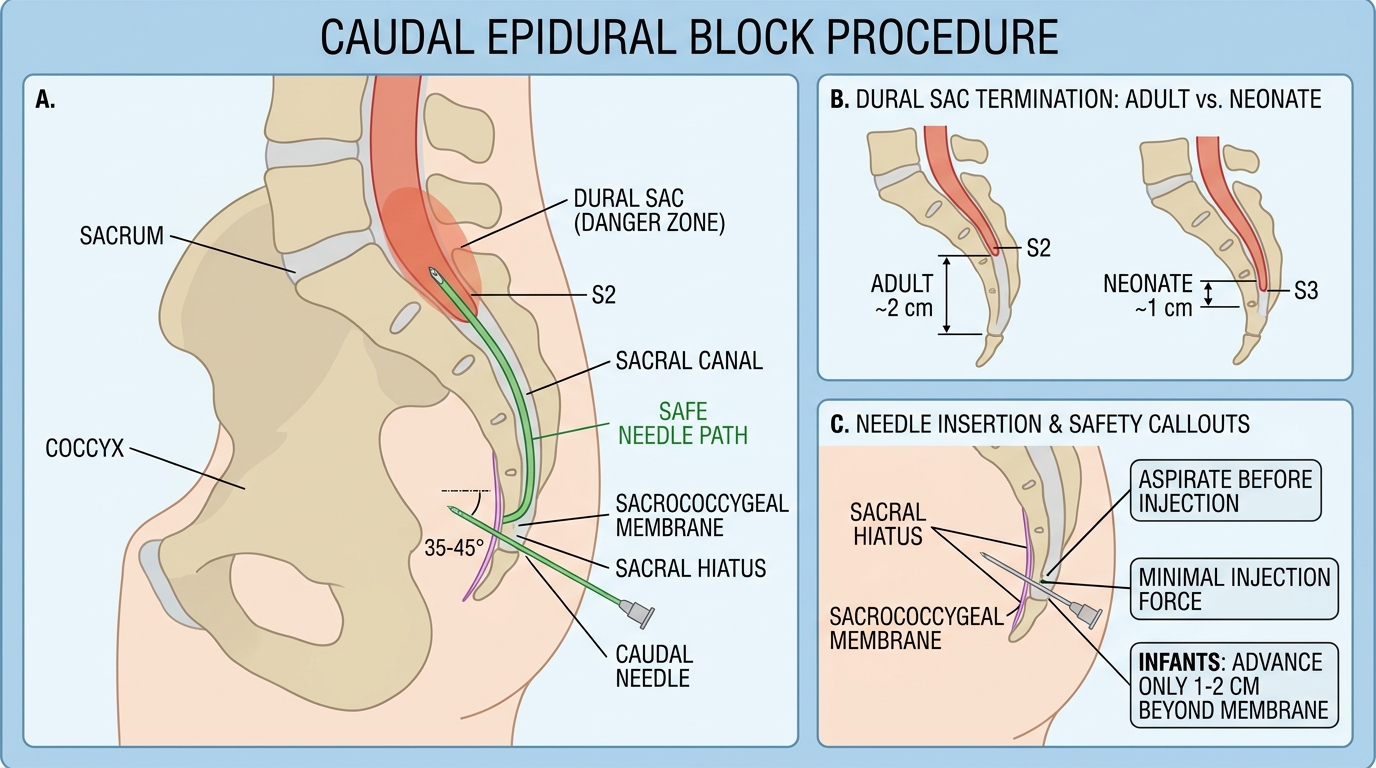
Critical safety relationship: In adults, the dural sac ends at approximately S2 (at the level of the posterior superior iliac spine). In neonates and infants, it extends to S3 or even S4. This means a needle advanced too deeply through the sacrococcygeal membrane risks puncturing the dural sac, which in adults lies at least 2 cm beyond the hiatus, but in neonates may be only 1 cm away. The caudal needle must never be advanced more than 1–2 cm beyond the sacrococcygeal membrane in infants, and the drug must always be injected with minimal force — aspiration first to exclude dural tap or intravascular placement.
Technique: Caudal Epidural Block in Children
The paediatric caudal block is performed under general anaesthesia (typically at the end of induction, before surgical preparation), because children cannot remain still for neuraxial procedures when awake. This is a fundamental distinction from adult neuraxial practice and is universally accepted as safe. The anaesthetist works at the foot of the table while the surgical team prepares the field.
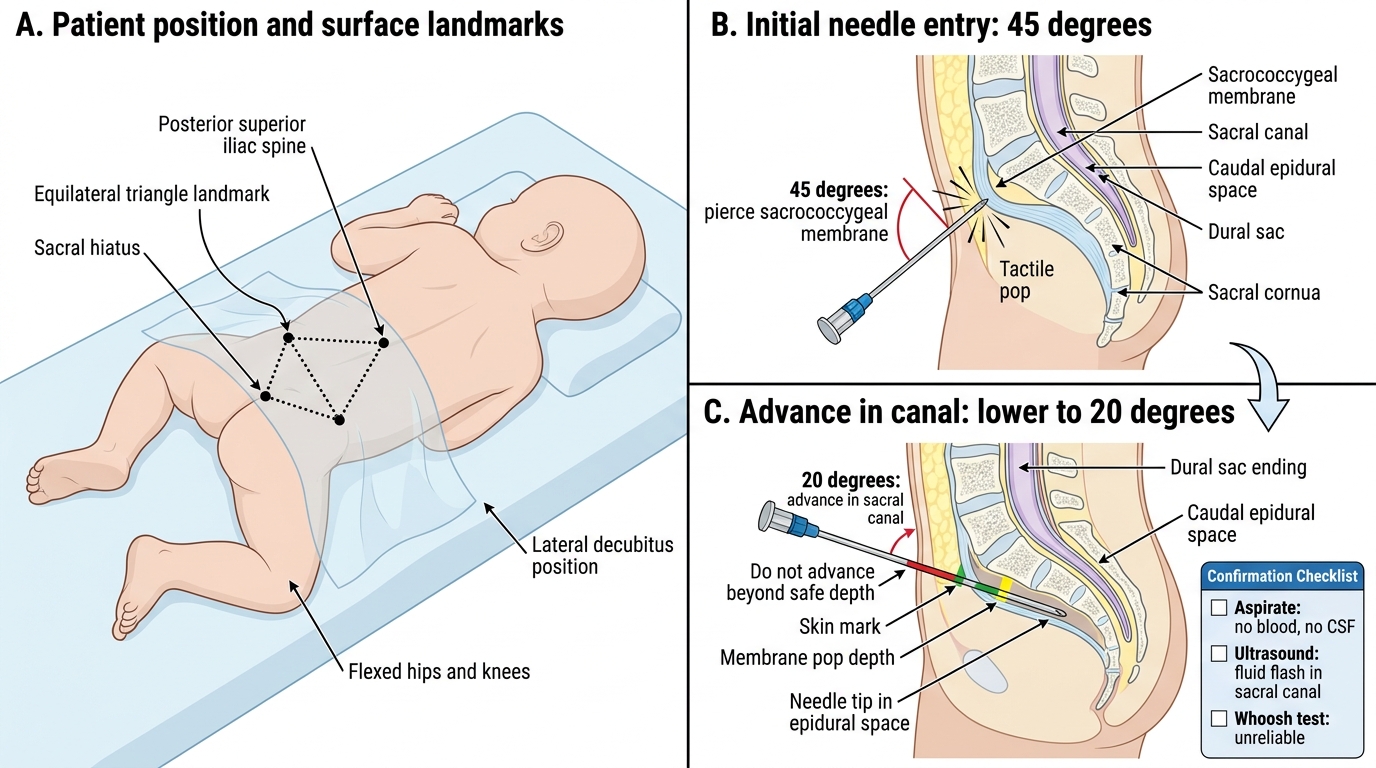
Patient positioning: Lateral decubitus (left or right, either works), hips and knees flexed to 90° — the "foetal position" — which opens the sacral hiatus and flattens the natal cleft, improving access. Alternatively, prone with a roll under the pelvis. Lateral is preferred for intraoperative use as it does not require patient repositioning for most inguinal or scrotal procedures.
Landmark identification (under aseptic technique): Palpate the posterior superior iliac spines — the line joining them passes over the S2 posterior sacral foramen, establishing the upper limit of safe needle placement. Move caudally to the tip of the sacrum — the sacral cornua are felt as two bony bumps flanking the sacral hiatus. The hiatus is the depression between the cornua, at the base of the triangle formed by the two posterior superior iliac spines and the coccyx. This is the equilateral triangle landmark for the sacral hiatus.
Needle insertion: A 22G (in small children) or 23G hypodermic needle is introduced at 45–60° to the skin surface, aiming cephalad through the sacrococcygeal membrane. A distinct "pop" or loss of resistance is felt as the needle pierces the membrane. The needle is then lowered (flattened) to approximately 20–30° and advanced 1–2 mm further into the sacral canal — no more. The short bevel must not enter the sacral canal beyond the membrane–to–dural sac distance, which in neonates can be as little as 1 cm.
Paediatric Caudal Block Technique
Confirmation tests before injection: (1) Aspiration — no blood (epidural vein puncture) and no CSF (dural tap). (2) The "whoosh test" — placing a stethoscope over the thoracolumbar spine while injecting a small air bolus (1–2 mL): a transmitted "whoosh" confirms intraspinal placement. However, this test is not universally reliable. (3) Ultrasound — in training settings, place the ultrasound probe in the midline just above the hiatus and observe a "flash" of fluid spreading into the sacral canal during injection. This is now the gold-standard confirmation method in paediatric regional anaesthesia.
Drug and volume selection (the Armitage formula): The volume of LA determines the spread (cephalad extent of block). The widely used Armitage formula:
- 0.5 mL/kg → sacral block (S3–S5)
- 1.0 mL/kg → lumbo-sacral block (L1 and below)
- 1.25 mL/kg → lower thoracic block (T10 and below)
Concentration: 0.25% bupivacaine is standard for most paediatric cases, staying well within the 2 mg/kg maximum. For inguinal herniotomy in a 10 kg child: 1.0 mL/kg × 0.25% = 2.5 mg/kg — this exceeds the maximum; therefore the dose must be calculated first and the concentration reduced to 0.2% if needed. Always calculate dose (mg/kg) before volume (mL/kg) — the volume formula alone is not a safety check.
SELF-CHECK
A 10 kg child undergoes inguinal herniotomy. The anaesthetist plans a caudal block using the Armitage formula for lumbo-sacral block (1.0 mL/kg) with 0.25% bupivacaine. What is the calculated dose in mg/kg, and is it within the safe limit?
A. 1.0 mL/kg × 0.25% = 2.5 mg/kg — exceeds the bupivacaine maximum of 2 mg/kg; use 0.2% or reduce volume
B. 1.0 mL/kg × 0.25% = 2.5 mg/kg — within the safe limit of 3 mg/kg for bupivacaine
C. 1.0 mL/kg × 0.25% = 25 mg — safe because it is less than 20 mL total volume
D. Concentration does not matter for caudal block because absorption from the caudal space is negligible
Reveal Answer
Answer: A. 1.0 mL/kg × 0.25% = 2.5 mg/kg — exceeds the bupivacaine maximum of 2 mg/kg; use 0.2% or reduce volume
0.25% bupivacaine = 2.5 mg/mL. At 1.0 mL/kg, this gives 2.5 mg/kg — which exceeds the maximum safe dose for bupivacaine of 2 mg/kg. The correct approach is to reduce the concentration to 0.2% bupivacaine (= 2.0 mg/mL × 1.0 mL/kg = 2.0 mg/kg, at the limit) or to reduce the volume. This is a common exam question and a real-world calculation error — always calculate mg/kg first from the proposed volume × concentration before proceeding.