Page 2 of 17
AS5.1-2 | Principles, Indications and Anatomy for Regional Anaesthesia — SDL Guide (Part 2)
Correlative Anatomy: The Brachial Plexus
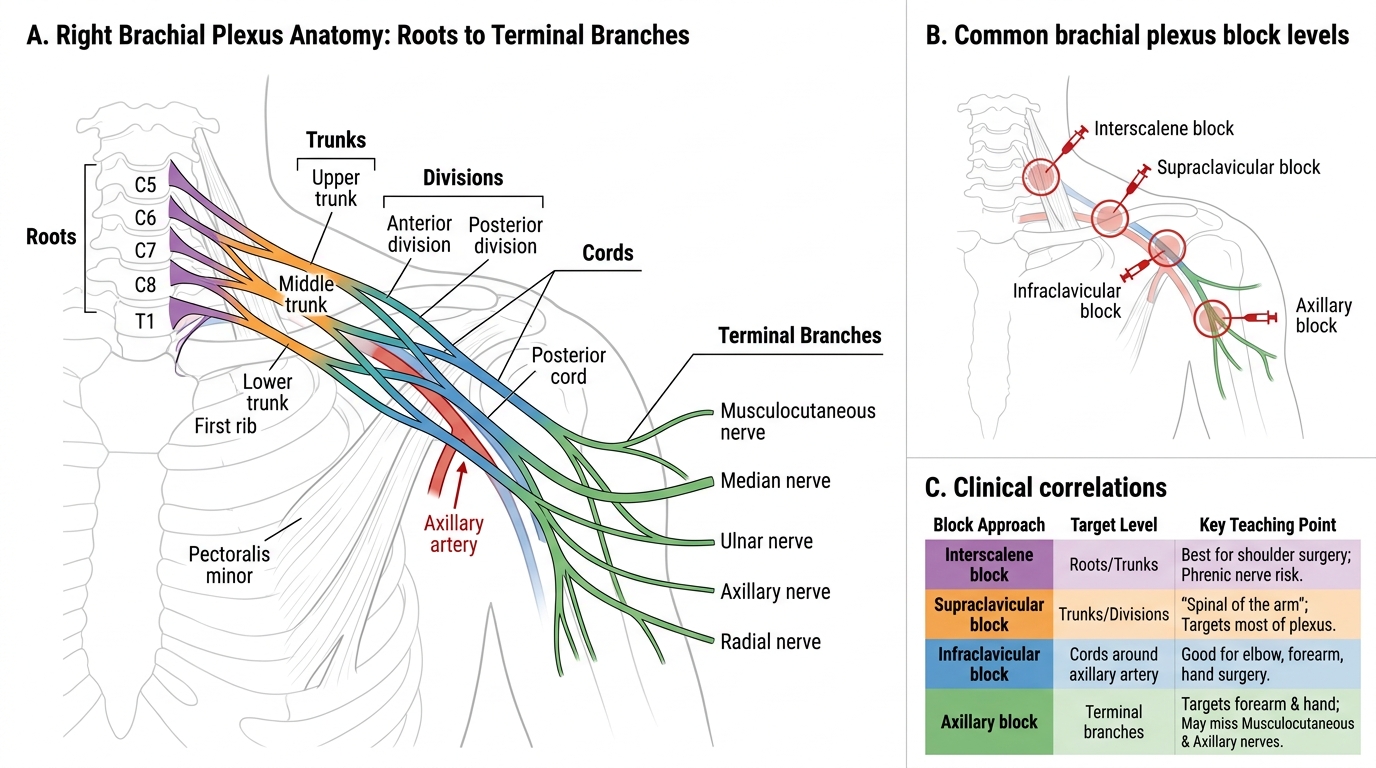
The brachial plexus is the neural network supplying the entire upper limb and much of the shoulder. It arises from the anterior primary rami of C5, C6, C7, C8, and T1 (the "Roots"), which emerge from the intervertebral foramina and pass between scalenus anterior and scalenus medius (the "interscalene groove"). From the roots, the plexus is organised as Roots → Trunks → Divisions → Cords → Terminal branches — a sequence worth memorising with the mnemonic Robert Taylor Drinks Cold Beer.
Trunks: The roots combine into three trunks in the posterior triangle of the neck. C5+C6 form the upper trunk, C7 continues as the middle trunk, and C8+T1 form the lower trunk. The upper and middle trunks travel superficially and are easily accessible for supraclavicular block; the lower trunk lies deep near the subclavian artery and first rib.
Brachial Plexus Anatomy and Regional Block Sites
Cords: The six divisions (anterior and posterior from each trunk) reconverge beneath the clavicle, lateral to the axillary artery, into three cords named for their relationship to the second part of the axillary artery — lateral, posterior, and medial cords. The cords are enclosed within the brachial plexus sheath, a fascial extension of the prevertebral fascia. This sheath continuity is clinically important: a single injection of LA into the sheath can produce complete plexus anaesthesia if the volume is sufficient, as in the axillary approach.
Terminal branches arise from the cords distal to the pectoralis minor. The median nerve (C5–T1), ulnar nerve (C8–T1), radial nerve (C5–T1), musculocutaneous nerve (C5–C7), and axillary nerve (C5–C6) are the five main terminal nerves. The musculocutaneous and axillary nerves leave the plexus proximal to the axilla, which is why an axillary block does not reliably anaesthetise the lateral forearm (musculocutaneous territory) without a specific supplement.
Clinical mapping: Interscalene block targets roots/trunks — ideal for shoulder surgery but risks phrenic nerve block (always unilateral, not safe if contralateral phrenic is compromised). Supraclavicular block targets the trunks — the "spinal of the arm" as it reliably covers the entire upper limb. Infraclavicular and axillary blocks target cords and terminal nerves — suitable for elbow, forearm, and hand surgery with less respiratory risk.
SELF-CHECK
A patient receives a subarachnoid block with a hyperbaric bupivacaine solution in the sitting position and is immediately laid supine with head slightly down (Trendelenburg). What is the expected direction of spread of the block?
A. The block will remain confined to the perineal (saddle) region because the injection is complete
B. The block will spread cephalad because the hyperbaric solution is denser than CSF and moves with gravity towards the head
C. The block will spread caudad because the Trendelenburg position lowers the feet
D. The baricity is irrelevant once the patient is supine
Reveal Answer
Answer: B. The block will spread cephalad because the hyperbaric solution is denser than CSF and moves with gravity towards the head
Hyperbaric solutions are denser than CSF (specific gravity > 1.008) and migrate toward the dependent (lowest) part of the subarachnoid space. In the Trendelenburg position, the head is lower than the buttocks, so gravity pulls the hyperbaric solution cephalad, spreading the block. If the anaesthetist wants to limit spread (e.g., saddle block), the patient must remain sitting for 3–5 minutes after injection before lying down.
Pharmacology of Local Anaesthetics for Regional Techniques
Local anaesthetics produce reversible blockade of voltage-gated sodium channels, preventing action potential propagation. Their clinical behaviour is characterised by onset speed, duration, potency, and toxicity profile — all of which guide agent selection for specific techniques.
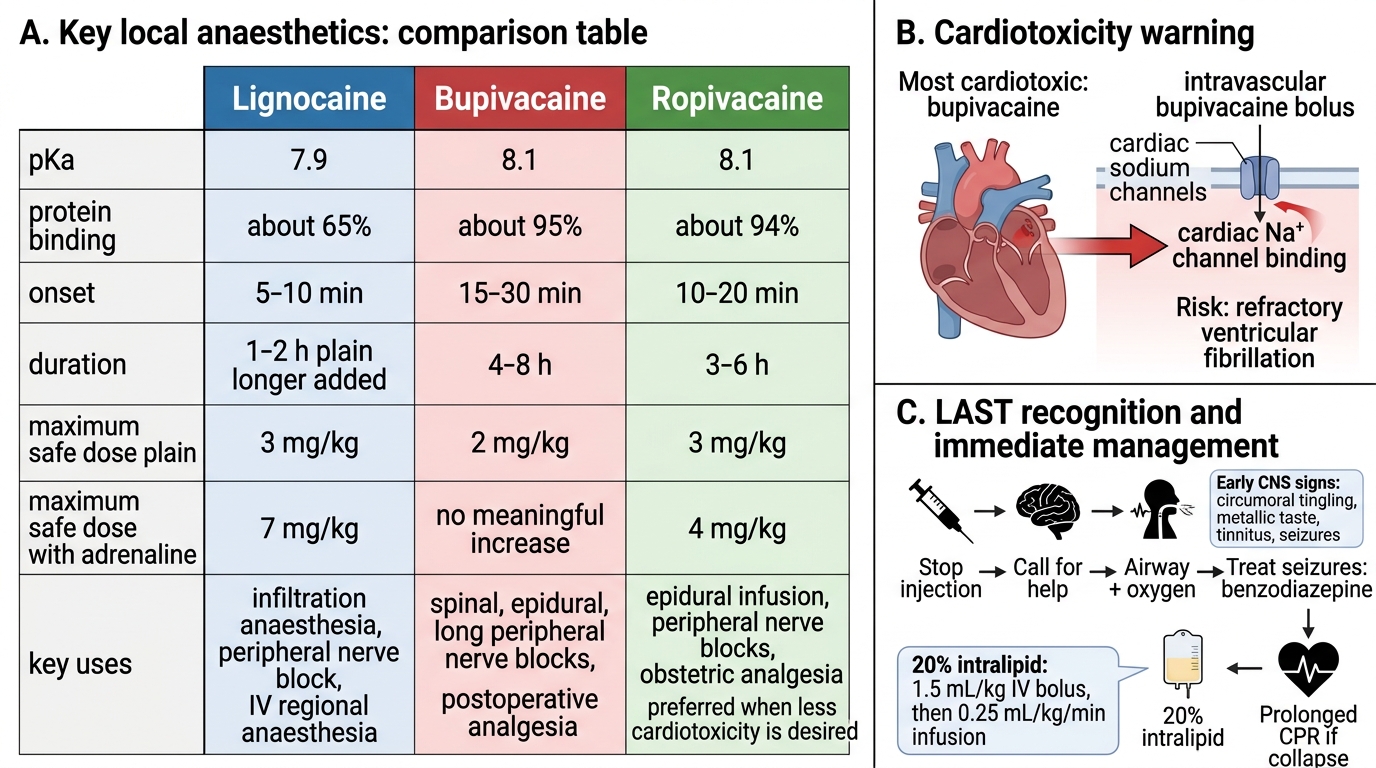
Onset speed is primarily determined by pKa. An LA with a pKa close to physiological pH (7.4) exists largely in the uncharged (base) form, which crosses the nerve membrane easily. Lignocaine (pKa 7.9) has a faster onset than bupivacaine (pKa 8.1) because a greater proportion is uncharged at pH 7.4. This explains why lignocaine is preferred when speed of onset is critical.
Duration is related to protein binding and lipid solubility. Bupivacaine and ropivacaine are highly protein-bound and lipid-soluble, producing long-duration blocks (2–4 hours for bupivacaine spinal, 12–24 hours epidural infusion with top-ups). Lignocaine is intermediate.
Key Local Anaesthetics and LAST Safety
Maximum safe doses are essential knowledge to prevent local anaesthetic systemic toxicity (LAST):
- Lignocaine: 3 mg/kg plain; 7 mg/kg with adrenaline.
- Bupivacaine: 2 mg/kg (no increase with adrenaline; most cardiotoxic LA — avoid intravenous injection absolutely). Bupivacaine's cardiotoxicity is due to its very high protein binding to cardiac sodium channels; even a small intravascular bolus can cause refractory ventricular fibrillation.
- Ropivacaine: 3 mg/kg plain; 4 mg/kg with adrenaline — less cardiotoxic than bupivacaine, now preferred for epidural infusions in many centres.
LAST management: The first sign is usually CNS excitation (circumoral tingling, metallic taste, tinnitus, seizures). Cardiovascular collapse follows with high doses. Treatment: stop injection immediately, call for help, maintain airway, treat seizures with benzodiazepine, and administer 20% intralipid (a lipid emulsion that acts as a "lipid sink," sequestering free bupivacaine away from cardiac tissue). The standard Intralipid regimen: 1.5 mL/kg bolus IV, then infusion at 0.25 mL/kg/min. CPR protocols for LAST recommend prolonged resuscitation as the lipid sink gradually reverses toxicity.
SELF-CHECK
A surgeon performing a digital nerve block uses 8 mL of 2% lignocaine (plain, no adrenaline) for a 50 kg patient. What is the maximum safe dose of plain lignocaine, and has it been exceeded?
A. Maximum 100 mg (3 mg/kg × 50 kg = 150 mg); 8 mL of 2% = 160 mg — this EXCEEDS the safe dose
B. Maximum 150 mg (3 mg/kg × 50 kg); 8 mL of 2% = 160 mg — this EXCEEDS the safe dose
C. Maximum 350 mg (7 mg/kg × 50 kg); 8 mL of 2% = 160 mg — within safe dose
D. Lignocaine has no maximum dose for digital blocks because it is rapidly metabolised locally
Reveal Answer
Answer: B. Maximum 150 mg (3 mg/kg × 50 kg); 8 mL of 2% = 160 mg — this EXCEEDS the safe dose
3 mg/kg × 50 kg = 150 mg maximum for plain lignocaine. 2% lignocaine = 20 mg/mL; 8 mL = 160 mg. This marginally exceeds the maximum dose. Importantly, for digital blocks, adrenaline-containing solutions are CONTRAINDICATED (end-artery territory — vasoconstriction risks digit ischaemia), so the plain dose limit of 3 mg/kg applies. The anaesthetist should either reduce the volume or use a lower concentration (e.g., 1% lignocaine).
Assessment and Planning for Regional Anaesthesia
Safe regional anaesthesia begins well before the needle is placed. A structured preoperative assessment for RA differs from a routine general anaesthetic work-up in several important respects, each designed to identify patients at elevated risk for block-specific complications. Systematic assessment allows the anaesthetist to select the most appropriate technique, anticipate difficulties, mitigate risks, and obtain valid informed consent — all of which are professional and medico-legal obligations.
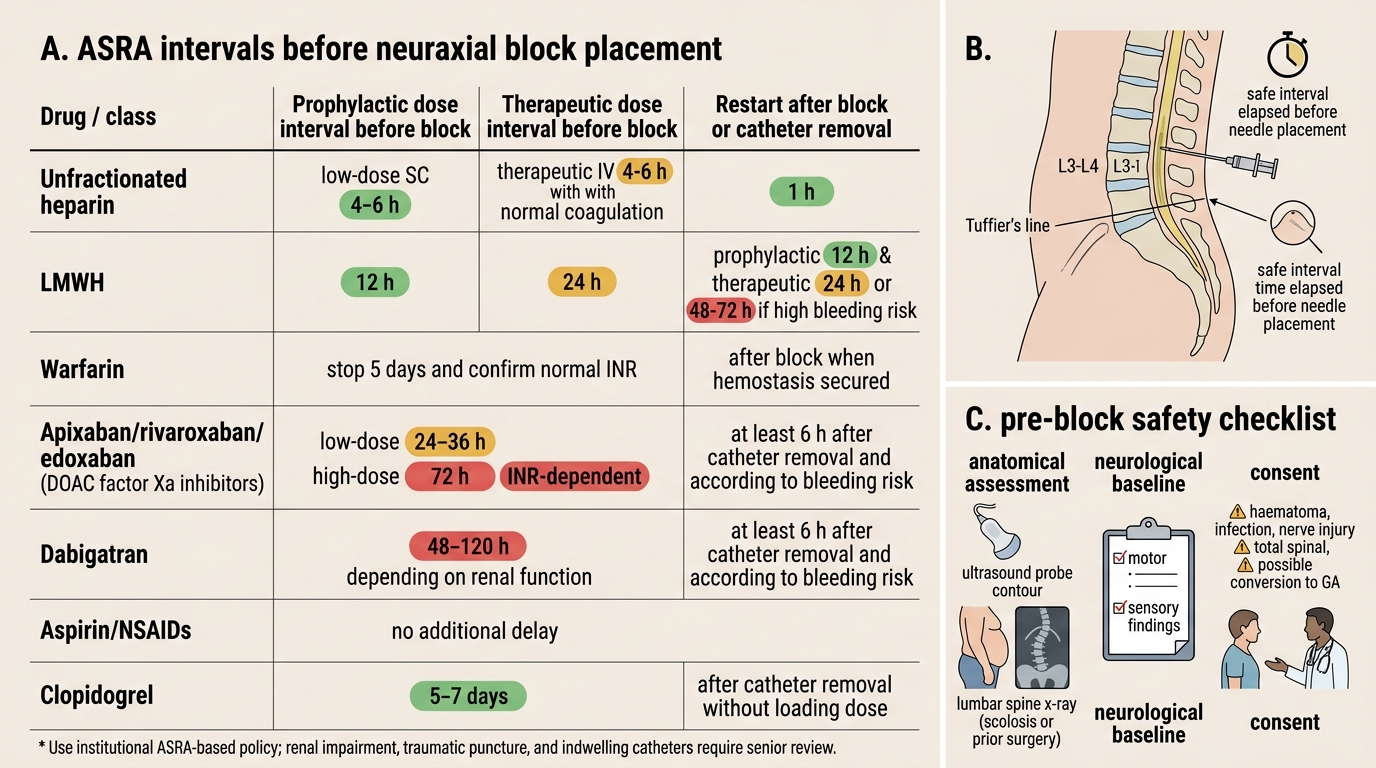
Coagulation status is paramount for neuraxial blocks. The ASRA (American Society of Regional Anesthesia) guidelines specify minimum time intervals that must elapse between the last dose of anticoagulant and neuraxial needle placement. Violation risks spinal or epidural haematoma — a neurosurgical emergency causing cord compression. Key intervals: unfractionated heparin prophylaxis — 4 hours; LMWH prophylaxis — 12 hours; LMWH therapeutic — 24 hours; warfarin — INR must be ≤ 1.4; clopidogrel — 7 days; aspirin alone is safe for neuraxial blocks in current guidelines.
ASRA Timing Intervals for Neuraxial Block
Anatomical assessment: Lumbar spine imaging (if available) for conditions such as scoliosis, previous spinal surgery, or deformity can alert the anaesthetist to potential difficulties. Landmark palpation in the preoperative area — identifying L3/L4 interspace at the level of the iliac crests (Tuffier's line) — confirms feasibility. Obesity may require ultrasound guidance.
Neurological baseline: Any pre-existing neurological deficit must be documented before RA. While not an absolute contraindication, a new neurological sign postoperatively is difficult to attribute definitively to the block rather than positioning or surgery without a documented baseline.
Consent and explanation: Patients must understand what the block entails — sensations during administration, expected area of numbness, duration, the possibility of incomplete block requiring supplementation or conversion to GA, and rare but serious complications (haematoma, infection, nerve injury, total spinal). Informed consent for regional anaesthesia is as important as consent for surgery.