Page 3 of 9
AS6.1-3 | Recovery Room Monitoring, Crash Cart Readiness and Complication Management — SDL Guide (Part 3)
Self-Assessment: Applying PACU Principles in Clinical Practice
Having worked through the principles of PACU monitoring, crash cart readiness, and complication management, it is now time to consolidate your understanding by applying these concepts to structured self-assessment questions that mirror the clinical reasoning required in the recovery room setting.
Case-based reasoning exercise: A 68-year-old woman with known ischaemic heart disease undergoes an open hysterectomy under general anaesthesia lasting three hours. She receives fentanyl 250 mcg total intraoperatively and two litres of Hartmann's solution. On PACU arrival, her SpO₂ is 95% on 6 L/min oxygen, she moves all four limbs, her BP is 145/92 (pre-operative baseline 138/85), she is calling out loudly and trying to remove her oxygen mask, her respiratory rate is 20/min, and her temperature is 35.4°C. Work through the following questions before reading the discussion:
- What is her Aldrete score? (Activity=2, Respiration=2, Circulation=2, Consciousness=2, SpO₂=1 — total 9; note: SpO₂ 95% requires supplemental O₂ → score 1, not 2)
- Is she ready for ward discharge? (Borderline: Aldrete score 9 is at threshold, but she is agitated, hypothermic, and borderline hypertensive — further assessment required before discharge)
- What is the most dangerous explanation for her agitation that you must rule out first, and what is the single bedside test you would perform immediately? (Rule out hypoxia: check SpO₂ on supplemental oxygen and assess respiratory rate; if SpO₂ adequate, proceed to pain assessment and check for urinary retention)
- Her temperature is 35.4°C. What active warming measure would you initiate, and which drug could you give if shivering becomes severe? (Forced-air warming blanket; pethidine 25 mg IV for shivering if required)
Conceptual self-check: Without looking at the SDL, attempt to list: the five parameters of the Aldrete Score and their scoring levels; the three pharmacological reversal agents used in the PACU and their primary indications; the stepwise management of laryngospasm from mild (stridor) to severe (silent chest); and the five most important items you would confirm are present when checking a crash cart at the start of a shift.
Integration check — connecting arc steps: The arc of this SDL moves from the clinical rationale for the PACU (step 1) through the physiological vulnerabilities that make the recovery room dangerous (step 2), to the systematic tools for detection (Aldrete score and monitoring parameters, step 3), to the management of the complications those tools detect (step 4), and now to self-assessment of your ability to integrate all four (step 5). Ask yourself: in a patient presenting with agitation, decreased SpO₂, and bradypnoea, can you construct the clinical reasoning path from recognition → differential (airway obstruction vs laryngospasm vs opioid depression) → confirmatory bedside manoeuvre → initial treatment → escalation trigger? If you can do that fluidly, you have satisfied the AS6.1–AS6.3 competencies.
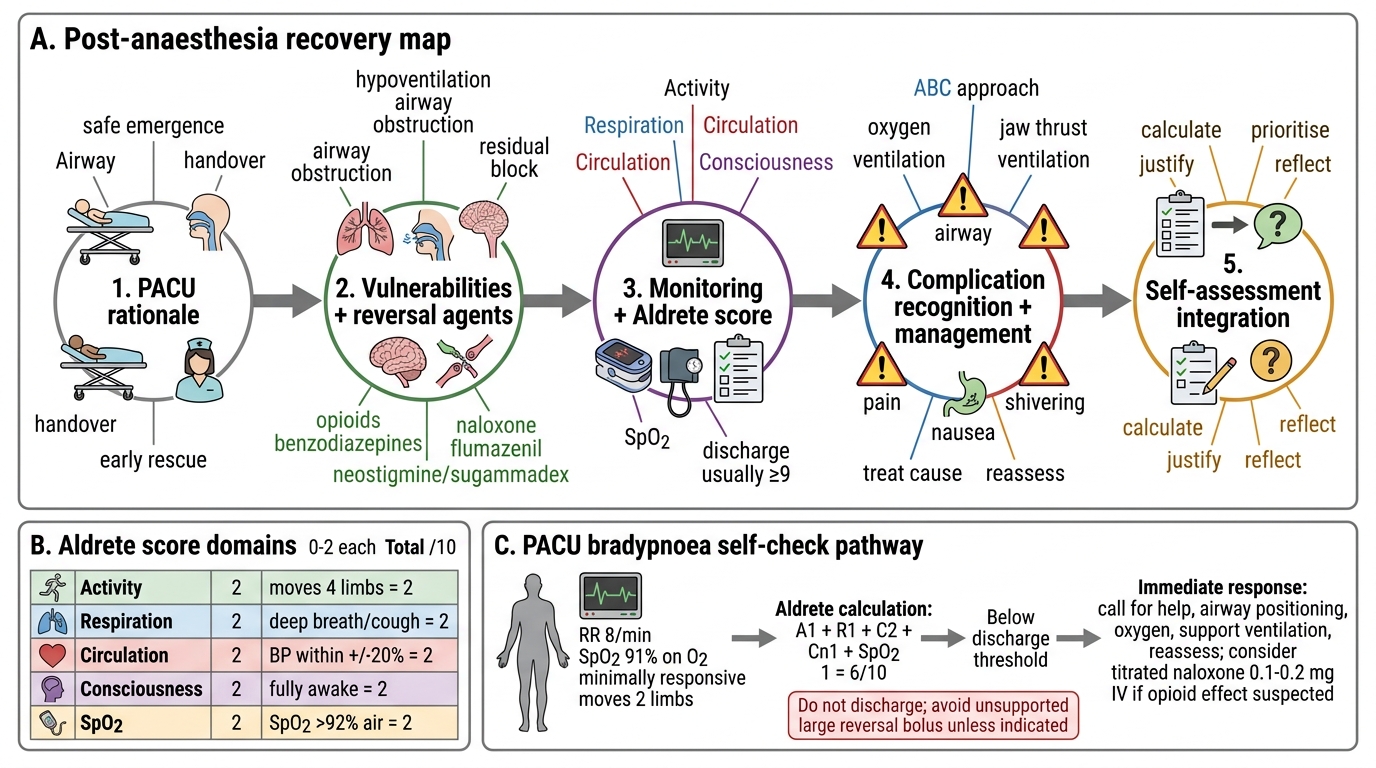
Post-Anaesthesia Recovery: AS Arc Concept Map
SELF-CHECK
A 45-year-old man arrives in the PACU following laparoscopic surgery under general anaesthesia. He is minimally responsive to calling, has a respiratory rate of 8 breaths per minute, SpO₂ is 91% on 6 L/min oxygen, BP is 118/72 mmHg (baseline 125/80), and moves two limbs to command. What is his Aldrete score, and what is the MOST appropriate immediate action?
A. A. Aldrete score 7; titrate naloxone 0.1–0.2 mg IV increments and reassess
B. B. Aldrete score 8; give flumazenil 0.2 mg IV to reverse residual sedation
C. C. Aldrete score 7; give full-dose naloxone 0.4 mg IV bolus immediately
D. D. Aldrete score 9; discharge to the ward with supplemental oxygen
Reveal Answer
Answer: A. A. Aldrete score 7; titrate naloxone 0.1–0.2 mg IV increments and reassess
Aldrete scoring for this patient: Activity=1 (moves two limbs to command), Respiration=1 (respiratory rate 8/min — shallow/limited), Circulation=2 (BP 118/72 is within ±20% of baseline 125/80), Consciousness=1 (minimally responsive = arousable on calling), SpO₂=1 (91% on supplemental O₂ = >90% but requiring O₂) — total = 6. This is well below the discharge threshold of ≥9. The clinical picture — bradypnoea (8/min), minimal responsiveness, and hypoxia on 6 L/min oxygen — is classic post-operative opioid-induced respiratory depression. The correct management is TITRATED naloxone in increments of 0.1–0.2 mg IV every 2–3 minutes, not a 0.4 mg bolus. A bolus causes abrupt opioid reversal with a catecholamine surge, acute pulmonary oedema, and severe uncontrolled pain. Flumazenil (option B) would be appropriate only if benzodiazepine excess were suspected. Discharge (option D) is absolutely contraindicated with this Aldrete score.
CLINICAL PEARL
The PACU is where the anaesthetist's job is most invisible and most important. The three most time-critical errors in recovery room management are: (1) giving 0.4 mg naloxone as a bolus instead of titrating 0.1–0.2 mg increments — abrupt reversal causes pulmonary oedema and catecholamine surge; (2) missing the early signs of laryngospasm (high-pitched inspiratory stridor) before it progresses to complete obstruction and silent chest; and (3) failing to recognise that a 'waking up' patient's restlessness is actually hypoxia, not simple emergence agitation. Always assess SpO₂ and respiratory rate FIRST before attributing agitation to behaviour. An Aldrete score of ≥9 is not a bureaucratic hurdle — it is the evidence base for safe discharge, validated against re-admission and adverse event rates. The crash cart seal number documented at the start of every shift is your last check that the cart has not been partially restocked incorrectly after a previous use.