Page 3 of 13
AS7.1-2 | ICU Organization, Functions and Admission-Discharge Criteria — SDL Guide (Part 3)
ICU Care Bundles and Communication: Management Standards
Within the ICU, certain recurring clinical scenarios require standardised management bundles that the whole team implements consistently. The ventilator care bundle for mechanically ventilated patients — head-of-bed elevation to 30-45 degrees to reduce aspiration and ventilator-associated pneumonia (VAP), daily sedation holiday to assess neurological status and readiness to wean, subglottic secretion drainage, oral care with chlorhexidine 0.12%, and peptic ulcer and deep-vein thrombosis prophylaxis — has been shown in multiple national programmes to reduce VAP rates by 50-66%. The central-line bundle mandates strict aseptic technique during insertion (full-barrier precautions: cap, mask, sterile gown, sterile gloves, large sterile drape), chlorhexidine skin preparation, optimal site selection (subclavian preferred over femoral for infection risk), daily need review, and prompt removal when no longer indicated, to minimise central-line-associated bloodstream infection (CLABSI). Communication in the ICU is a management responsibility as critical as the pharmacological interventions: daily structured family meetings (Update, Goals, Questions format) reduce family anxiety and facilitate informed consent for high-risk procedures. Formal withdrawal-of-care discussions, when clinically appropriate, require the ICU consultant, a senior nurse, and where available a palliative-care specialist. End-of-life care and ethical decisions — do-not-resuscitate (DNR) orders, withdrawal of life-sustaining treatment, organ donation conversations — are a recognised function of the ICU team and require documentation, multidisciplinary consensus, and clear family communication.
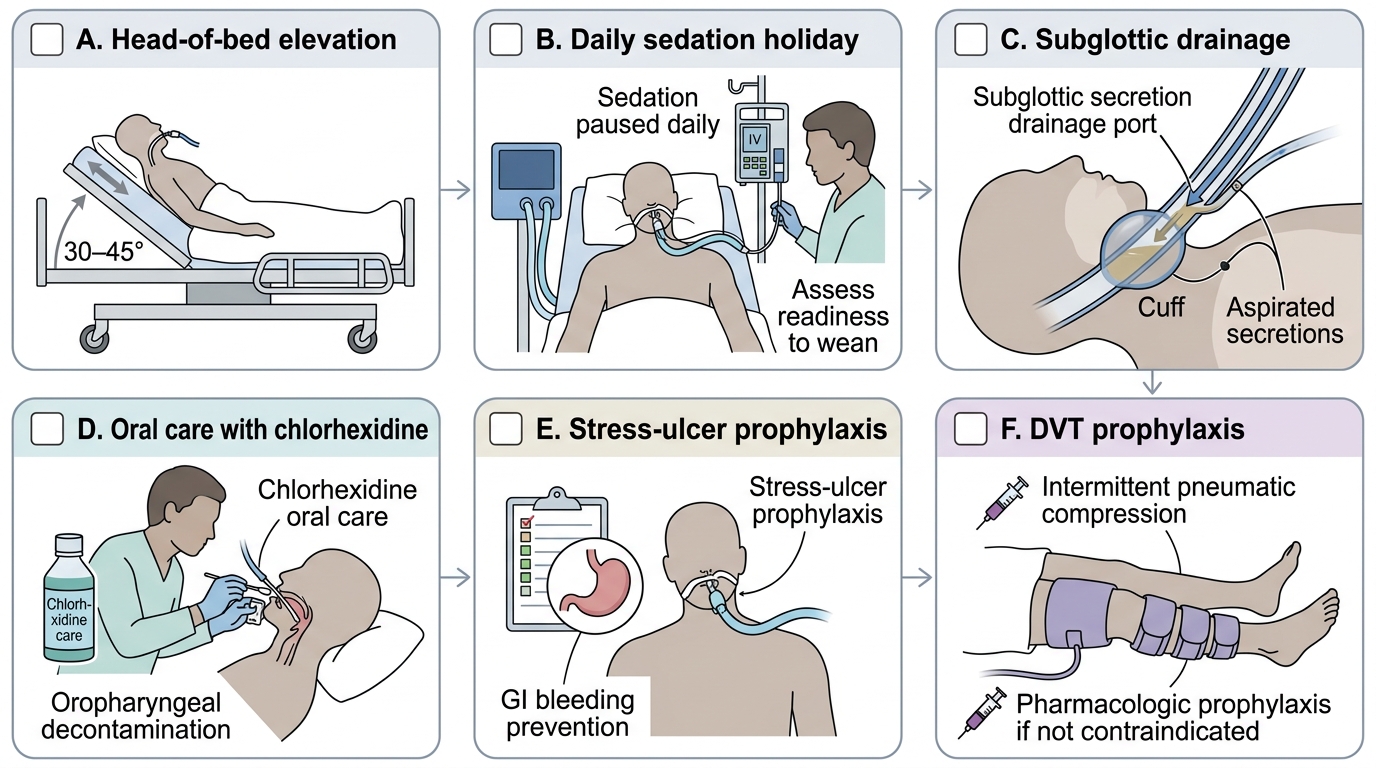
VAP Prevention Bundle: Six-Step ICU Checklist
CLINICAL PEARL
The ICU bounce-back rule: Any patient discharged from the ICU who returns within 48 hours has approximately 2-3 times higher in-hospital mortality than first-time ICU admissions. This underscores that discharge criteria should be met comfortably, not marginally. When in doubt about readiness, a one-day extension in the ICU is almost always safer than an unplanned readmission from the ward. Equally, the window of opportunity for organ-support initiation is narrow: physiological decompensation is far easier to prevent than to reverse — the patient who should have been admitted 4 hours ago will need twice the resources and time to stabilise.
SELF-CHECK
A post-laparotomy patient on the ward develops: BP 84/52 mmHg, HR 122 bpm, SpO2 92% on room air, GCS 13 (baseline 15), urine output 9 mL over 2 hours (body weight 70 kg). Which statement about ICU admission criteria is correct?
A. Only the blood pressure criterion (SBP < 90) is met; the other parameters do not independently reach threshold
B. Urine output meets the criterion because 9 mL in 2 h for 70 kg = 0.064 mL/kg/h, well below the 0.5 mL/kg/h threshold
C. GCS 13 does not meet the criterion because the threshold is GCS 8 or below
D. No single criterion alone mandates ICU admission; a combination of three or more is required
Reveal Answer
Answer: B. Urine output meets the criterion because 9 mL in 2 h for 70 kg = 0.064 mL/kg/h, well below the 0.5 mL/kg/h threshold
Urine output 9 mL in 2 h for a 70 kg patient = 4.5 mL/h = 0.064 mL/kg/h, far below the 0.5 mL/kg/h for 2 consecutive hours threshold. This alone meets an ICU admission criterion. Additionally, GCS drop of 2 or more points from baseline (15 to 13 = drop of 2) is also an independent trigger. SBP 84 mmHg unresponsive to fluids also qualifies. The rule is that each parameter independently can mandate ICU admission — it is not a combination requirement.
Self-Assessment: Applying ICU Criteria in Clinical Scenarios
Test your understanding of ICU organization and criteria by working through these self-assessment scenarios. Applying structured criteria to real clinical vignettes consolidates the conceptual knowledge from this module into practical decision-making skills that every graduating doctor needs regardless of specialty.
Scenario A — Admission decision: A 55-year-old man with known type 2 diabetes presents with fever (39.8 degrees C), confusion (GCS 11, baseline 15), BP 82/48 mmHg after 1 L fluid challenge, urine output 10 mL/h for 3 hours (weight 80 kg), lactate 4.2 mmol/L. Identify which objective criteria are met and name the disease-specific indication that applies. What level of ICU (I, II, or III) does this patient require, and why?
Scenario B — Discharge decision: A ventilated post-CABG patient is now day 5 in the ICU. Current status: extubated 24 hours ago, SpO2 97% on 4 L/min nasal prongs, BP 118/72 on no vasopressors for 36 hours, GCS 15, urine output 0.8 mL/kg/h, serum creatinine declining, blood glucose controlled on sliding-scale insulin. The family asks when transfer to the surgical ward can happen. Evaluate this patient against each discharge criterion domain (respiratory, cardiovascular, neurological, metabolic, organ support) and state whether they meet criteria for discharge.
Scenario C — Team and resource triage: A district hospital with a 4-bed ICU has all beds occupied by ventilated patients when two more critically ill admissions arrive simultaneously. As the registrar on call, what decision framework would you use to triage these patients, and what factors would influence whether transfer to a higher-level facility is warranted?
For each scenario: name the criteria framework you are applying (ISCCM guidelines), articulate the reasoning you would use in a handover to a senior colleague, and identify one key safety concern you would document.