Page 7 of 13
AS7.3-5 | Unconscious Patient Care, Ventilator Setup and ICU Monitoring — SDL Guide (Part 3)
Putting It Together: ICU Management Conduct in a Ventilated Unconscious Patient
The daily management conduct for a ventilated unconscious patient integrates airway care, ventilator optimisation, monitoring interpretation, and complication prevention into a structured routine. The ICU morning ward round follows a systematic patient assessment format: events in the past 24 hours (fever, haemodynamic instability, new culture results); 24-hour fluid balance (total in — total out, including insensible losses); current ventilator settings and ABG result; cardiovascular status (trends in MAP, HR, vasopressor requirements); neurological status (GCS trend, latest imaging if available); renal function (urine output trend, creatinine trend); nutrition (enteral feed tolerated versus prescribed); antibiotic day number and de-escalation eligibility; and procedures planned for the day. Ventilator weaning is initiated when the patient meets readiness criteria: primary cause of ventilatory failure is improving or resolved; the patient can breathe spontaneously on pressure support with adequate tidal volumes; FiO2 has been reduced to 0.40 or below; PEEP is 5 cmH2O; the patient is adequately awake (GCS motor response 5-6) and following simple commands; haemodynamics are stable on minimal vasopressor. The spontaneous breathing trial (SBT) tests these criteria: the patient is placed on T-piece or low-level PSV (5 cmH2O) for 30-120 minutes while observing for failure signs: SpO2 below 90%, RR above 35, HR above 140 or below 50, BP above 180/90 or below 90/60, respiratory distress, or GCS deterioration. If the SBT is passed, the patient is extubated. If failed, the reason is identified and the trial repeated after 24 hours of rest. Tracheostomy is considered when prolonged ventilation (more than 10-14 days) is anticipated, because it improves comfort, facilitates weaning, reduces sedation requirements, and simplifies airway nursing care.
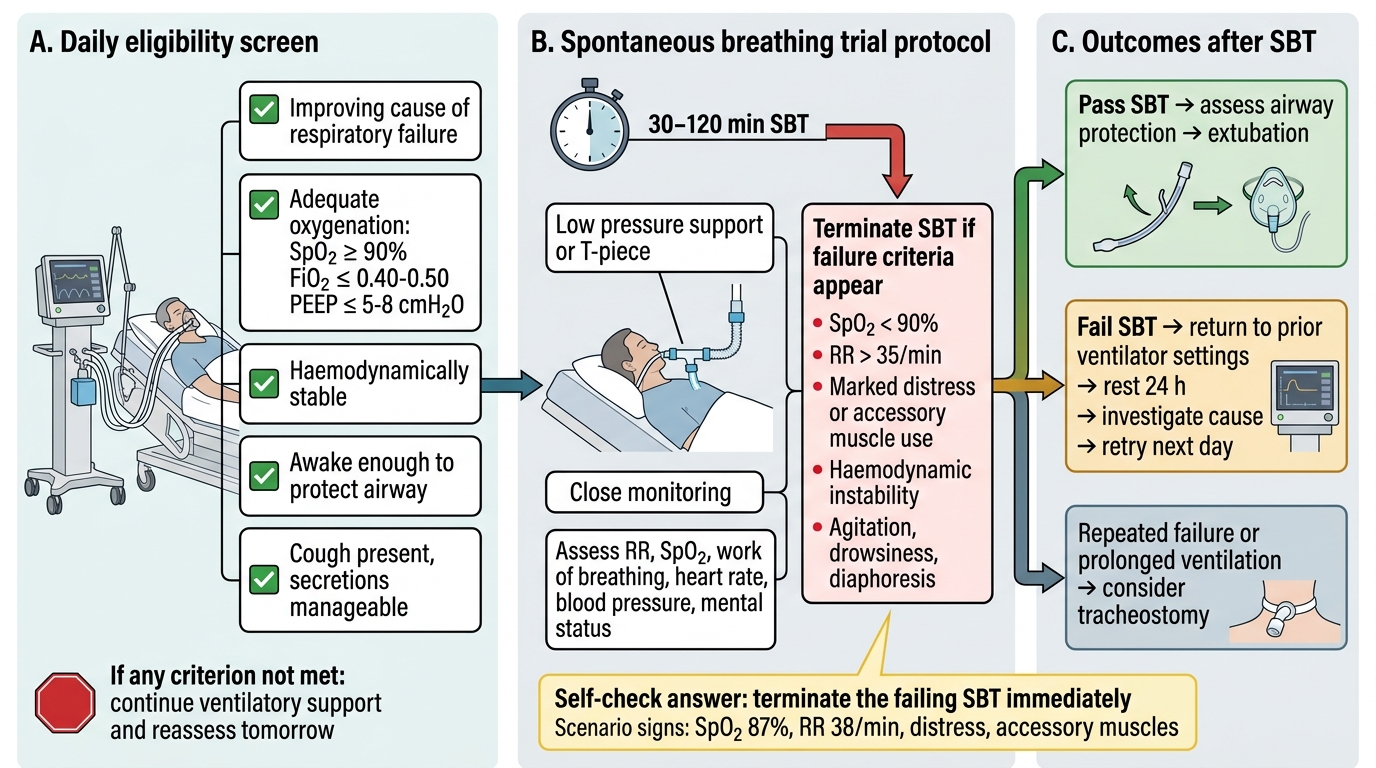
Daily Ventilator Weaning Assessment Algorithm
SELF-CHECK
During a spontaneous breathing trial (SBT) on a post-operative ventilated patient, the nurse observes: SpO2 drops to 87%, respiratory rate rises to 38 breaths/min, and the patient appears distressed and is using accessory muscles. What is the correct immediate management?
A. Continue the SBT for the full 120-minute duration — these signs are expected and will resolve
B. Terminate the SBT immediately, return the patient to prior ventilator settings, and investigate the cause of failure
C. Increase the pressure support level by 10 cmH2O and continue the trial
D. Extubate the patient immediately since SpO2 of 87% still indicates residual oxygen reserve
Reveal Answer
Answer: B. Terminate the SBT immediately, return the patient to prior ventilator settings, and investigate the cause of failure
The SBT must be terminated immediately when failure criteria are met — SpO2 below 90%, RR above 35, respiratory distress, or haemodynamic instability. Continuing the SBT in a failing patient risks respiratory muscle exhaustion, hypoxic injury, and cardiorespiratory arrest. The correct action is to return to prior ventilator settings (which the patient was tolerating), allow 24 hours of rest, identify the cause of failure (residual secretions, weak respiratory muscles, unresolved lung pathology, delirium causing dyssynchrony), and retry the SBT when the cause is addressed.
Self-Assessment: Integrating Monitoring and Ventilator Management
Test your understanding of ventilator setup, unconscious patient management, and ICU monitoring through the following self-assessment exercises. The goal is to move from knowing individual parameters to integrating them into a clinical picture.
Scenario A — Ventilator alarm response: A ventilated patient's high-pressure alarm fires. The ventilator displays peak airway pressure of 42 cmH2O (set high-pressure alarm at 40 cmH2O). SpO2 is 91% and falling. List five possible causes in order of urgency (most immediately life-threatening first) and describe one bedside action to rapidly exclude or confirm each. Hint: use the DOPE mnemonic (Displacement, Obstruction, Pneumothorax, Equipment failure).
Scenario B — Monitoring integration: An unconscious patient 48 hours post-subarachnoid haemorrhage has the following: MAP 72 mmHg, HR 58 bpm (sinus bradycardia), bilateral pupils 5 mm and sluggishly reactive (yesterday 3 mm and brisk), GCS dropped from 9 to 6 over 2 hours. The nurse reports the blood pressure rose transiently to 180/95 mmHg before the HR slowed. Identify the clinical syndrome, name the reflex involved, and state the immediate management priority.
Scenario C — Ventilator settings calculation: A 70 kg (IBW 68 kg) female patient is intubated for acute respiratory distress syndrome (ARDS). Her current ABG on FiO2 0.70 shows: PaO2 58 mmHg, PaCO2 48 mmHg, pH 7.30. Current settings: VT 510 mL, RR 14, PEEP 8 cmH2O. Identify which setting violates lung-protective strategy. Calculate the corrected VT. Comment on whether permissive hypercapnia is acceptable for this patient.
For each scenario: name the monitoring parameter that first alerted you, describe the integration across organ systems, and state one management action and one safety documentation point.