Page 4 of 11
AS9.3-4 | Perioperative Fluid Therapy and Blood Product Use — SDL Guide
CLINICAL SCENARIO
A 58-year-old woman undergoing a Whipple's procedure for pancreatic cancer has been nil-by-mouth for 12 hours. Intraoperatively, she develops haemorrhage from the portal vein — estimated blood loss reaches 2 litres over 30 minutes. Her haemoglobin drops to 5.8 g/dL, INR is 2.1, and platelets are 48,000/µL. The anaesthesiologist must now make rapid, consequential decisions: how much crystalloid? Which blood components? In what ratio? Give too little fluid and the patient dies of circulatory failure; give too much and she develops dilutional coagulopathy and pulmonary oedema. Perioperative fluid therapy and blood product administration are arguably the most complex pharmacological decisions in anaesthetic practice — and they are made repeatedly, under pressure, in every major surgical case.
WHY THIS MATTERS
Fluid management errors are among the most common and consequential intraoperative mistakes. Both under-resuscitation (hypovolaemia, end-organ ischaemia) and over-resuscitation (pulmonary oedema, dilutional coagulopathy, anastomotic oedema) worsen surgical outcomes. The shift from the traditional 'liberal' infusion of saline-based crystalloids toward goal-directed fluid therapy and balanced crystalloids reflects decades of clinical trials demonstrating that the choice of fluid type, volume, and timing matters enormously. Blood component therapy adds another layer of complexity: each component — packed red blood cells (PRBCs), fresh frozen plasma (FFP), platelets, and cryoprecipitate — has specific indications, storage constraints, administration requirements, and adverse effects. The NMC 2024 curriculum requires anaesthesiology trainees to describe both the principles of perioperative fluid therapy (AS9.3) and the indications and use of blood products in the perioperative period (AS9.4). Mastery of this content underpins safe anaesthetic practice in virtually every surgical subspecialty.
RECALL
Before proceeding, revisit the following foundational concepts:
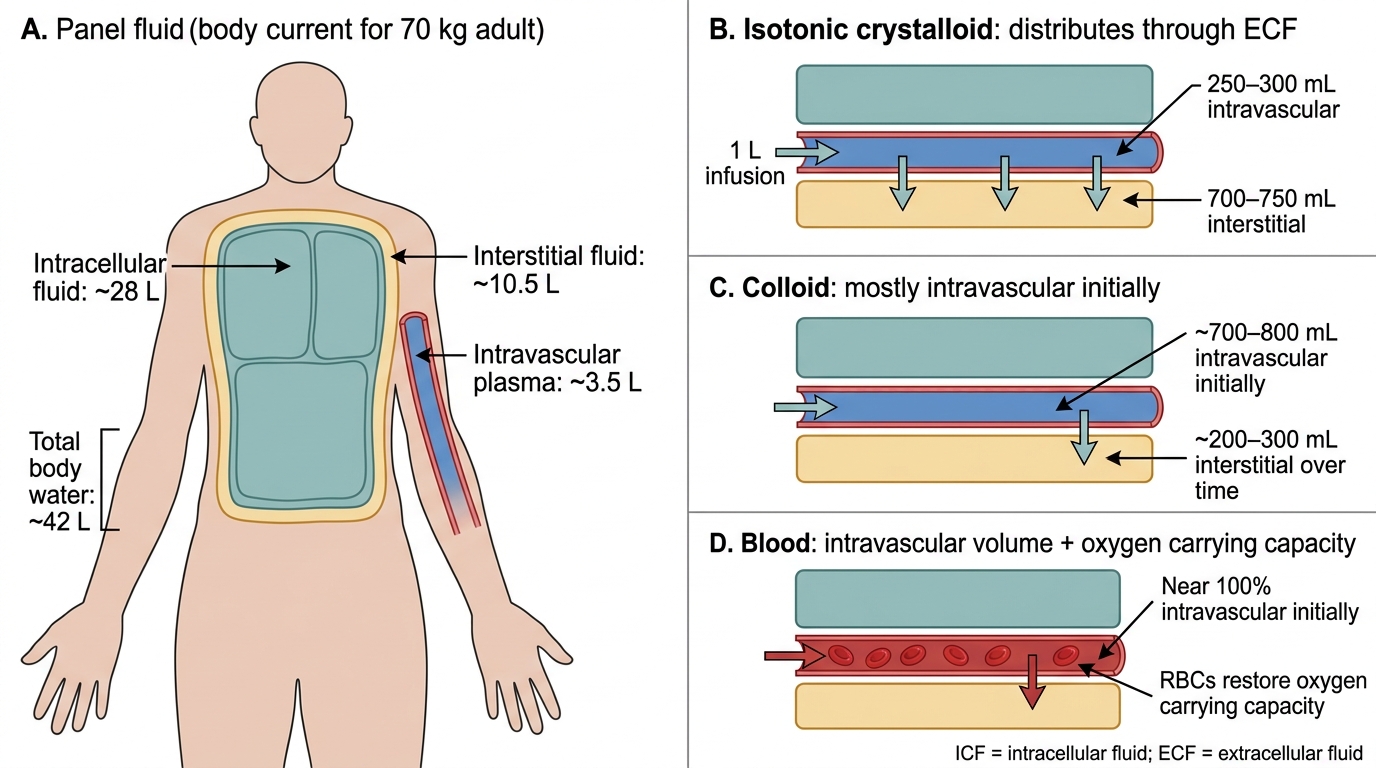
- Body fluid compartments: total body water (~60% body weight), divided into intracellular fluid (ICF, ~40%) and extracellular fluid (ECF, ~20%); ECF further divided into interstitial (~15%) and intravascular/plasma (~5%)
- Starling's law of the capillary: net fluid movement across capillary walls determined by the balance of hydrostatic and oncotic pressures (Starling forces)
- Normal blood composition: haemoglobin 12–16 g/dL; haematocrit 36–48%; platelets 150,000–400,000/µL; PT/INR 0.8–1.2; fibrinogen 2–4 g/L
- Coagulation cascade: intrinsic and extrinsic pathways converging on Factor X activation, thrombin generation, and fibrin clot formation
- Preoperative fasting: traditional 6-hour solid food / 2-hour clear fluid fast; creates a modest fluid deficit that may require intraoperative correction
Orientation and Clinical Relevance of Perioperative Fluid Therapy
Perioperative fluid therapy encompasses all decisions about intravenous fluid administration from the preoperative period through recovery from anaesthesia. It is one of the most universally applied interventions in surgery — essentially every patient undergoing general or regional anaesthesia receives intravenous fluids — yet it remains one of the most contested areas of anaesthetic pharmacology, with ongoing debate about which fluid, how much, and how fast.
The clinical imperative for perioperative fluids arises from several converging physiological stresses. Preoperative deficits accumulate from fasting, bowel preparation, fever, and pre-existing dehydration; enhanced recovery after surgery (ERAS) protocols have reduced these deficits substantially by permitting carbohydrate drinks until 2 hours before induction. Intraoperative losses include evaporation from exposed viscera (particularly in open abdominal surgery, where insensible losses may reach 5–10 mL/kg/hour), blood loss, and fluid redistribution into a 'third space' of oedematous tissue — though the clinical reality of a physiologically distinct third space is now disputed, with most authorities attributing apparent third-space losses to capillary leak driven by surgical inflammation. Vasodilation from anaesthetic agents — particularly volatile anaesthetics, propofol, and neuraxial blockade — reduces systemic vascular resistance and increases the effective vascular capacitance, demanding additional fluid to maintain adequate venous return and cardiac output.
The clinical consequences of mismanaged fluid balance range from subtle (postoperative nausea, delayed return of gut function) to life-threatening (acute kidney injury from hypovolaemia, respiratory failure from pulmonary oedema, anastomotic leak from gut oedema). A structured, physiologically-informed approach — rather than empirical 'running in' of arbitrary volumes — is therefore a core anaesthetic competency.
Body Fluid Compartments and IV Fluid Distribution
Classification and Properties of IV Fluids
A sound understanding of fluid physiology begins with the classification of intravenous fluids and their distribution characteristics. Intravenous fluids are broadly categorised as crystalloids or colloids, with blood and blood products forming a distinct third category that also replaces oxygen-carrying capacity. The choice between these categories is not merely a matter of preference but of physiology: each fluid type distributes across body compartments in a predictable pattern that depends on the molecular size of its solute, and that distribution pattern determines both the clinical effect and the complications of administration. An anaesthesiologist who understands why isotonic crystalloid expands the interstitium far more than the intravascular space — and why this matters in a post-abdominal-surgery patient — will prescribe fluids more rationally than one who simply follows a protocol.
Crystalloids are solutions of small molecules (ions, glucose) that distribute freely across capillary membranes. When 1 litre of isotonic crystalloid is infused, approximately 250–300 mL remains in the intravascular space at 30 minutes (the remainder distributes into the interstitium); the actual proportion depends on the plasma oncotic pressure and capillary integrity. Key crystalloid preparations are:
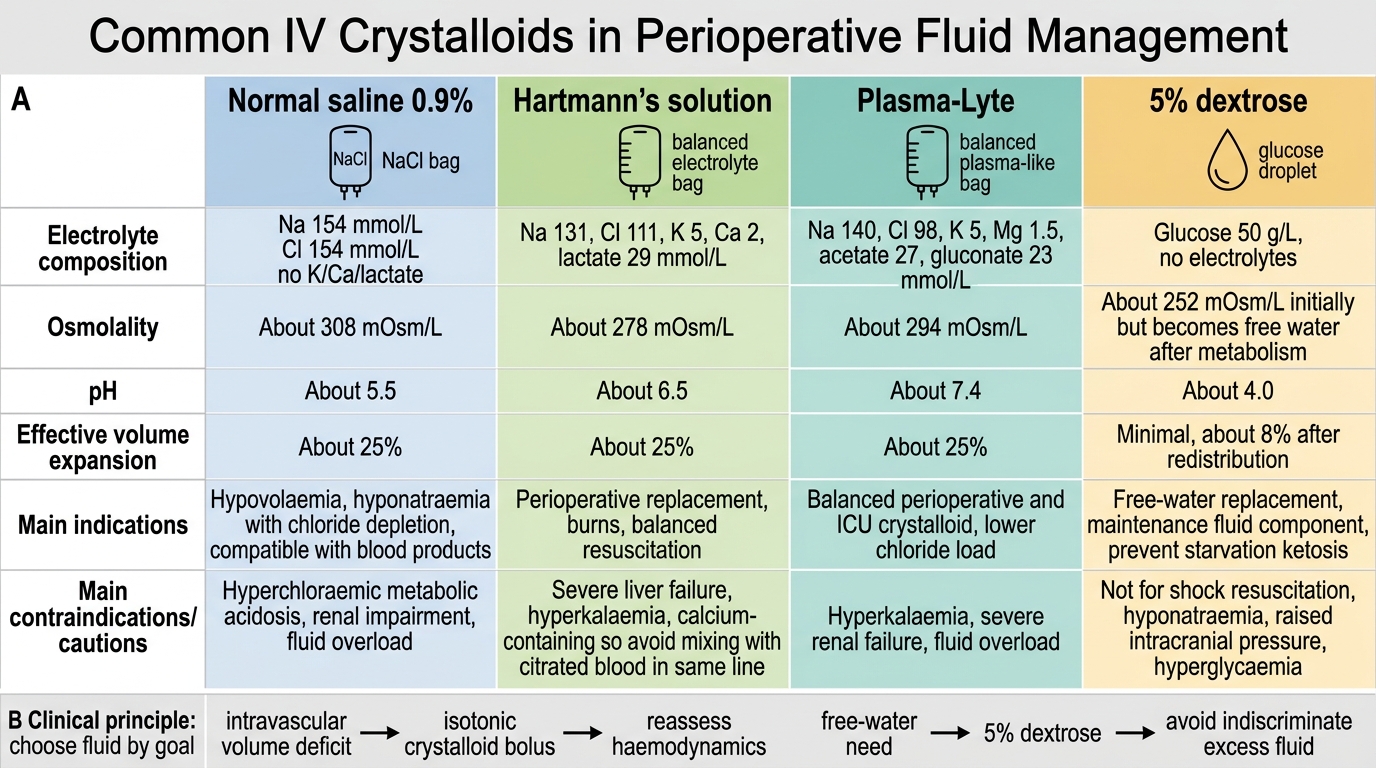
- Normal saline (0.9% NaCl): osmolality 308 mOsm/L; Na⁺ 154 mmol/L, Cl⁻ 154 mmol/L. Large volumes cause hyperchloraemic metabolic acidosis because the excess chloride suppresses renal bicarbonate reabsorption and reduces renal blood flow. Associated with increased acute kidney injury risk in critical illness.
- Hartmann's solution (compound sodium lactate / Ringer's lactate): balanced crystalloid; Na⁺ 130, Cl⁻ 109, K⁺ 4, Ca²⁺ 2, lactate 28 mmol/L; osmolality ~275 mOsm/L. Lactate is metabolised by the liver to bicarbonate, making this solution physiologically neutral. Preferred for most perioperative fluid resuscitation.
- Plasmalyte 148: balanced crystalloid with acetate and gluconate as buffers instead of lactate; osmolality 294 mOsm/L. Avoids the slight hypotonicity of Hartmann's. Preferred when lactate metabolism may be impaired (severe liver disease).
- 5% Dextrose: essentially free water; distributes across all compartments (ICF 67%, ECF 33%); no role in circulatory resuscitation but used for hypoglycaemia correction and hypernatraemia management.
Colloids are solutions of large molecules (proteins, starches) that are too large to cross the intact capillary membrane freely, so they exert an oncotic pressure that retains fluid intravascularly. Colloids provide greater intravascular volume expansion per litre than crystalloids but carry distinct risks:
- Human albumin solution (HAS) 4–5%: physiological colloid; the reference oncotic agent. Safe in hepatic failure (replaces depleted endogenous albumin). Expensive. Used in specific indications: spontaneous bacterial peritonitis, hepatorenal syndrome, post-large-volume paracentesis.
- Hydroxyethyl starch (HES): semi-synthetic starch; provides effective intravascular expansion but is associated with acute kidney injury and coagulopathy in septic patients. Contraindicated in sepsis, ICU patients, and patients with renal impairment (European regulatory restriction). Limited perioperative use.
- Gelatin solutions (Gelofusine, Haemaccel): bovine gelatin; moderate volume expansion; risk of anaphylaxis; not approved in all countries.
The crystalloid vs colloid debate has produced extensive trial data. The CRISTAL and ALBIOS trials found no mortality benefit for colloids over crystalloids in critical care. Current guidance favours balanced crystalloids (Hartmann's or Plasmalyte) as the default resuscitation fluid for most perioperative patients.
Common IV Crystalloids Compared
Principles of Perioperative Fluid Management
The evolution of perioperative fluid management has moved through three historical paradigms: the permissive liberal infusion era of the 1960s–1990s (driven by Moore's 'third-space' theory), the restrictive fluid era of the early 2000s (driven by concerns about oedema), and the current goal-directed fluid therapy (GDFT) era, in which fluid is administered in response to haemodynamic targets rather than arbitrary volume prescriptions. Each paradigm shift was driven by clinical trial evidence, and understanding the reasoning behind GDFT is as important as knowing its operational steps.
Goal-directed fluid therapy (GDFT) uses dynamic haemodynamic parameters — particularly stroke volume variation (SVV), pulse pressure variation (PPV), and oesophageal Doppler-measured stroke volume — to identify patients who are 'fluid responsive' (i.e., will increase their cardiac output by ≥10–15% with a 250 mL crystalloid bolus). Fluid is administered only to fluid-responsive patients. This avoids the indiscriminate infusion of large volumes in patients whose cardiac performance is already on the flat portion of the Frank-Starling curve (where more fluid increases preload but not stroke volume). Clinical trials of GDFT in major elective surgery consistently show reductions in postoperative complications (particularly gut-related), hospital length of stay, and occasionally mortality.
Maintenance vs resuscitation fluids serve different physiological roles and must be prescribed separately:
- Maintenance fluids replace ongoing obligatory losses (urine, insensible losses): approximately 25–30 mL/kg/day in adults. Balanced crystalloids are the default.
- Resuscitation boluses correct acute haemodynamic instability: 250–500 mL balanced crystalloid over 10–15 minutes, reassessed with dynamic parameters before repeating.
Calculation of fluid requirements involves:
1. Preoperative deficit = fasting hours × hourly maintenance rate (simplified: 4 mL/kg for first 10 kg + 2 mL/kg for next 10 kg + 1 mL/kg for each remaining kg)
2. Intraoperative losses = estimated blood loss (replaced mL for mL up to the Maximum Allowable Blood Loss [MABL]) + insensible losses (3–5 mL/kg/hr for laparotomy, 1–2 mL/kg/hr for closed procedures)
3. MABL = estimated blood volume × (starting haematocrit − acceptable minimum haematocrit) ÷ average haematocrit; below MABL, blood transfusion is indicated.
Perioperative fluid monitoring tools include urine output (target ≥0.5 mL/kg/hr), mean arterial pressure (target ≥65 mmHg), lactate trend (normalisation suggests adequate tissue perfusion), SVV/PPV (best in mechanically ventilated patients with regular rhythm and tidal volume >8 mL/kg), and oesophageal Doppler or pulmonary artery catheter in high-risk patients.
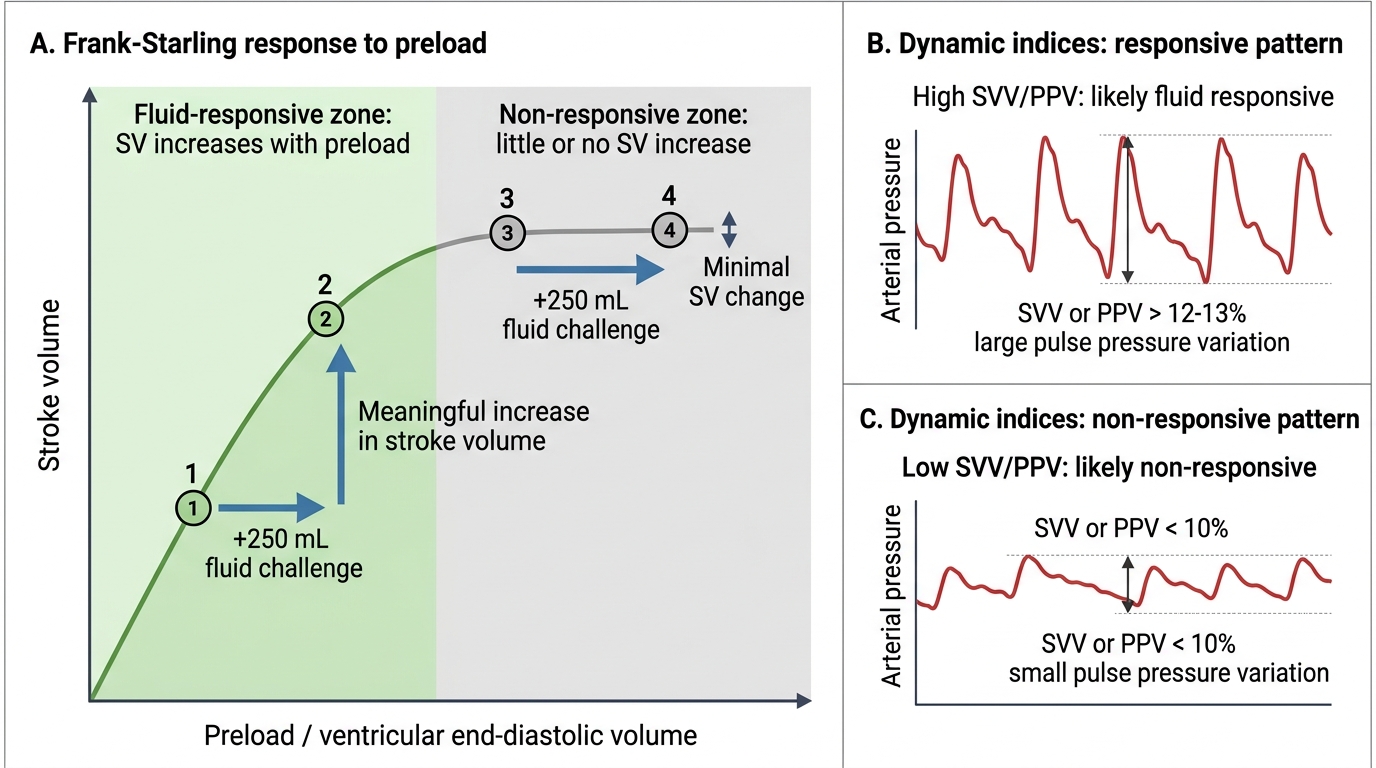
Fluid Responsiveness on the Frank-Starling Curve