Page 3 of 9
AN10.1-13 | Axilla, Shoulder and Scapular region — SDL Guide (Part 3)
The Big Movers — Trapezius and Latissimus Dorsi (AN10.8)
Two large, flat muscles dominate the back and contribute to shoulder movements. You can feel both on your own body right now.

Figure: The Big Movers — Trapezius and Latissimus Dorsi (AN10.8)
Trapezius — the diamond-shaped muscle covering the upper back. Place your hand on your opposite shoulder and shrug — you're feeling trapezius contract.
- Origin: skull (superior nuchal line), ligamentum nuchae, spinous processes of C7–T12
- Insertion: clavicle (lateral third), acromion, spine of scapula
- Action: Upper fibres = elevate scapula (shrugging), middle fibres = retract scapula (squeezing shoulder blades together), lower fibres = depress scapula
- Nerve supply: Spinal accessory nerve (CN XI) + C3, C4 (proprioception)
Latissimus dorsi — the broadest muscle of the back ('latissimus' = widest). It wraps from the lower back to the arm.
- Origin: spinous processes of T6–T12, thoracolumbar fascia, iliac crest, lower 3–4 ribs
- Insertion: floor of intertubercular sulcus (bicipital groove) of humerus
- Action: extension, adduction, and medial rotation of the arm. The climbing muscle — pull your body up with your arms and latissimus dorsi does most of the work
- Nerve supply: Thoracodorsal nerve (C6, 7, 8 — from the posterior cord)
Both muscles are superficial — you can see them clearly on a muscular person. They move the scapula and arm respectively in powerful, gross movements.
The Rotator Cuff — SITS Muscles (AN10.9, AN10.10)
The shoulder joint is the most mobile joint in the body — but this mobility comes at a cost: stability. Unlike the hip (where the ball sits deep in a socket), the shoulder's humeral head sits on a shallow glenoid cavity, like a golf ball on a tee.

Figure: The Rotator Cuff — SITS Muscles (AN10.9, AN10.10)
What keeps the ball on the tee? The answer is the rotator cuff — four muscles whose tendons blend with the shoulder joint capsule, forming a 'cuff' that holds the humeral head firmly against the glenoid.
Remember them with the mnemonic SITS (from top to bottom around the scapula):
- Supraspinatus — sits above the spine of the scapula
- Action: initiates abduction (first 0–15°), then deltoid takes over
- Nerve: suprascapular nerve (C5, C6)
- This is the most commonly torn rotator cuff muscle
- Infraspinatus — sits below the spine of the scapula
- Action: lateral (external) rotation of the arm
- Nerve: suprascapular nerve (C5, C6)
- Teres minor — small muscle below infraspinatus
- Action: lateral rotation (assists infraspinatus)
- Nerve: axillary nerve (C5, C6)
- Subscapularis — fills the subscapular fossa (front of the scapula)
- Action: medial (internal) rotation of the arm
- Nerve: upper and lower subscapular nerves (C5, C6)
Key concept: three of the four SITS muscles rotate the arm laterally (supraspinatus helps, infraspinatus and teres minor are the main lateral rotators), while only subscapularis rotates medially. This imbalance matters: when the rotator cuff is torn (usually supraspinatus), the arm can't initiate abduction properly — the painful arc of a rotator cuff tear.
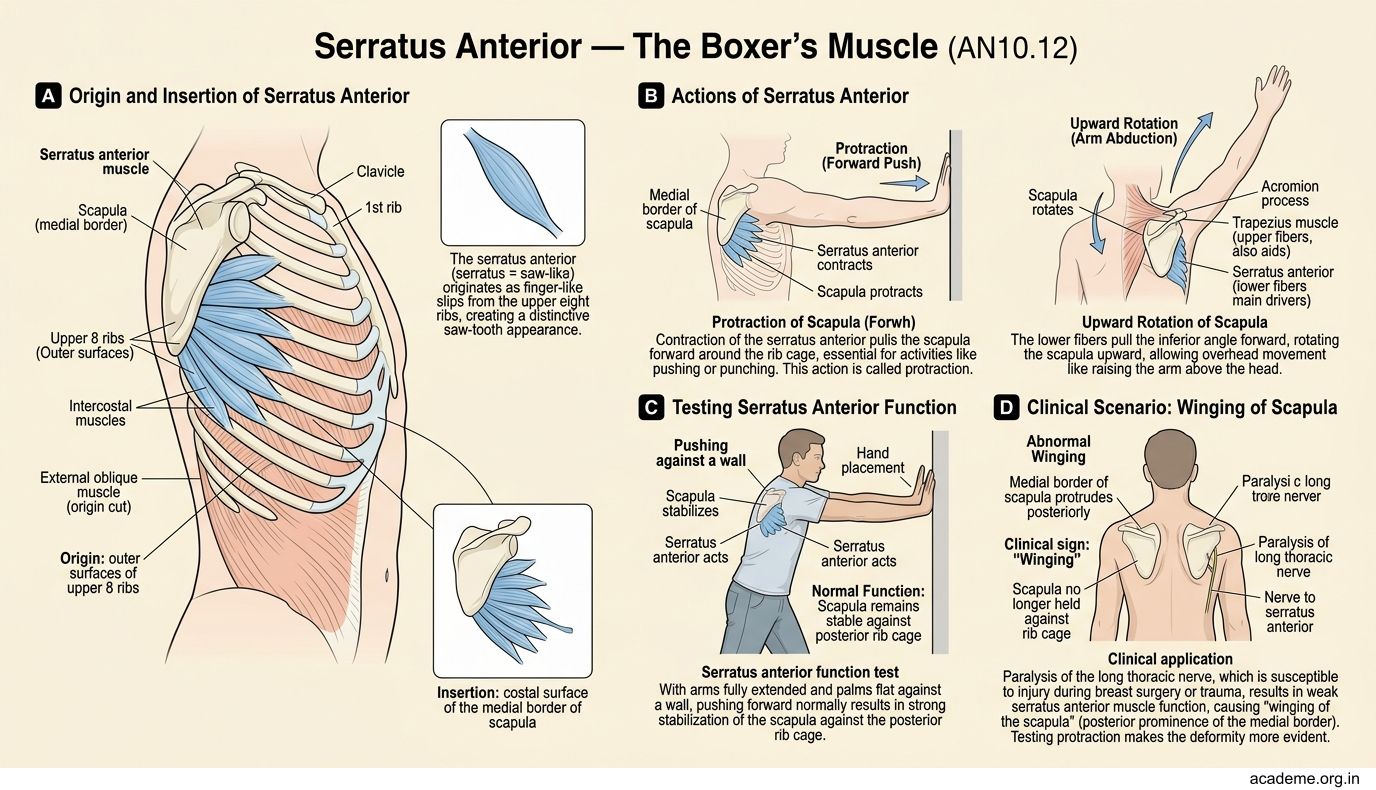
Serratus Anterior — The Boxer's Muscle (AN10.12)
Place your hand flat against the side of your chest, just below the armpit. Now push forward against a wall. The muscle you feel is the serratus anterior — a saw-toothed muscle (serratus = saw-like) that attaches from the ribs to the medial border of the scapula.
- Origin: outer surfaces of upper 8 ribs (the saw-tooth pattern)
- Insertion: costal surface of the medial border of scapula
- Action: protracts the scapula (pulls it forward around the chest wall) and rotates the scapula upward (essential for raising the arm above the head)
- Nerve supply: Long thoracic nerve (C5, C6, C7) — also called the nerve of Bell
Clinical connection — winged scapula:
The long thoracic nerve is vulnerable during surgery (mastectomy, axillary lymph node clearance) because it runs along the chest wall superficially. If it's damaged, serratus anterior is paralysed, and the scapula 'wings' — the medial border sticks out like a wing when the patient pushes against a wall.
This is called a winged scapula, and it's a classic clinical sign that examiners love to test. The patient can't raise their arm above the head because the scapula can't rotate upward.
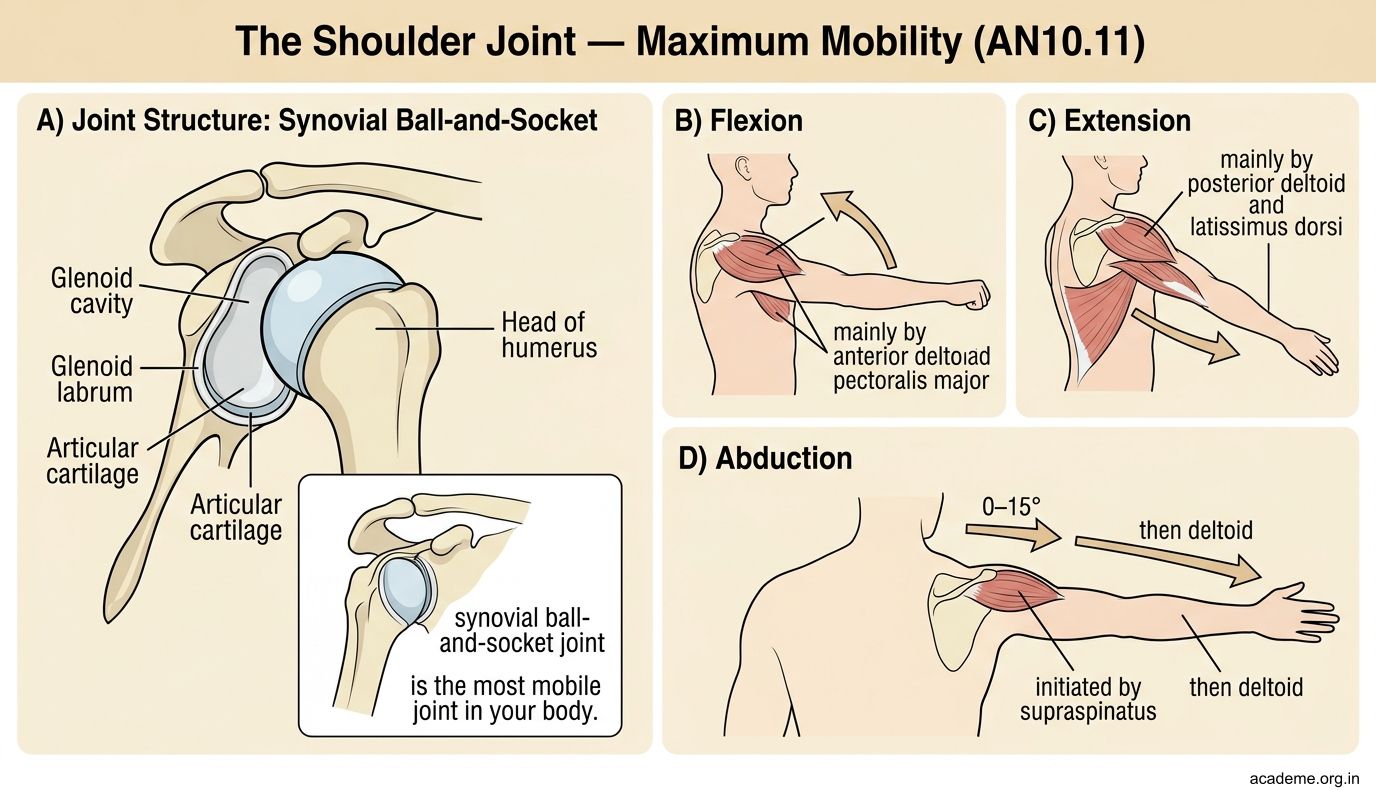
The Shoulder Joint — Maximum Mobility (AN10.11)
The glenohumeral (shoulder) joint is a synovial ball-and-socket joint — the most mobile joint in your body. It allows movements in all planes:
- Flexion (arm forward) — mainly by anterior deltoid and pectoralis major
- Extension (arm backward) — mainly by posterior deltoid and latissimus dorsi
- Abduction (arm out to the side) — initiated by supraspinatus (0–15°), then deltoid (15–90°), then trapezius rotates the scapula (90–180°)
- Adduction (arm to the body) — pectoralis major and latissimus dorsi
- Medial rotation — subscapularis, pectoralis major, latissimus dorsi
- Lateral rotation — infraspinatus and teres minor
- Circumduction — a combination of all movements
Why is the shoulder so mobile yet vulnerable?
- The glenoid cavity is small and shallow (covers only 1/3 of the humeral head) — like a golf ball on a tee
- The glenoid labrum (fibrocartilage ring) deepens the socket slightly but doesn't prevent dislocation
- The joint capsule is loose and redundant (has folds to allow movement)
- Stability depends almost entirely on the rotator cuff muscles — not on bony architecture
The shoulder dislocates more than any other joint. The most common direction is anteroinferior (the humeral head slips forward and downward) — because the rotator cuff is weakest inferiorly and the capsule is thinnest anteroinferiorly.
Scapular Anastomosis — The Backup Blood Supply (AN10.13)
What happens if the axillary artery is blocked? The shoulder region has a built-in backup: the scapular anastomosis — a network of arteries around the scapula that connects the subclavian artery system (above the block) with the third part of the axillary artery (below the block).
The key arteries in this anastomosis are:
- Suprascapular artery (from the thyrocervical trunk of the subclavian) — runs above the scapula
- Deep branch of the transverse cervical artery (also from the subclavian) — runs along the medial border of the scapula (also called the dorsal scapular artery)
- Subscapular artery and its branch, the circumflex scapular artery (from the 3rd part of the axillary artery) — runs behind the scapula
These arteries anastomose freely around the scapula, creating a detour route. If the axillary artery is slowly blocked (e.g., by atherosclerosis), the scapular anastomosis enlarges gradually and can maintain blood flow to the arm.
Spiral forward: We'll revisit arterial anastomoses as a general concept when we study the cardiovascular system (Week 20–24). The principle is the same everywhere: the body builds in backup routes near vulnerable points.
Axillary Nerve Injury — The Deltoid Danger Zone (AN10.12)
The axillary nerve (C5, C6) is a terminal branch of the posterior cord. It wraps around the surgical neck of the humerus — the narrow region just below the humeral head. This makes it vulnerable in two situations:
- Fracture of the surgical neck of the humerus — common in elderly patients who fall on an outstretched hand
- Anterior dislocation of the shoulder — the humeral head displaces forward and stretches the nerve
- Intramuscular injection in the wrong site — injecting too low in the deltoid can hit the axillary nerve
Consequences of axillary nerve injury:
• Paralysis of deltoid — can't abduct the arm beyond 15° (supraspinatus can still initiate, but deltoid can't continue)
• Paralysis of teres minor — weakness of lateral rotation
• Loss of sensation over the regimental badge area — a patch of skin over the lower deltoid (where a military regiment badge would sit)
Safe injection zone: For intramuscular injections in the deltoid, always inject in the upper third of the deltoid, approximately 2–3 finger-breadths below the acromion. This avoids the axillary nerve, which runs at the level of the surgical neck (lower portion of the deltoid).
SELF-CHECK
A medical student is about to give a deltoid intramuscular injection. To avoid damaging the axillary nerve, the injection should be placed:
A. In the lower third of the deltoid, near the deltoid tuberosity
B. In the upper third of the deltoid, 2-3 finger-breadths below the acromion
C. At the exact centre of the deltoid muscle
D. At the posterior border of the deltoid
Reveal Answer
Answer: B. In the upper third of the deltoid, 2-3 finger-breadths below the acromion
The axillary nerve wraps around the surgical neck of the humerus at the level of the lower deltoid. To avoid it, inject in the upper third of the deltoid — 2–3 finger-breadths below the acromion. This is above the path of the axillary nerve. Injecting too low risks paralysing the deltoid.
CLINICAL PEARL
Rotator cuff tears are extremely common — by age 60, up to 30% of people have a partial tear (often asymptomatic). The supraspinatus tendon is most commonly torn because it has a relatively poor blood supply in its 'critical zone' (near its insertion on the greater tubercle) and is repeatedly compressed between the humeral head and the acromion during abduction. Patients present with a painful arc — pain between 60° and 120° of abduction (the range where supraspinatus is maximally compressed). Below 60° and above 120°, the pain decreases. MRI is the investigation of choice. Treatment ranges from physiotherapy (strengthening the remaining rotator cuff muscles) to arthroscopic surgical repair.