Page 1 of 6
AN11.1-6 | Arm & Cubital fossa — SDL Guide
Learning Objectives
- Describe and demonstrate the muscle groups of the upper arm, with emphasis on biceps brachii and triceps brachii (AN11.1)
- Identify and describe the origin, course, relations, branches, and termination of important nerves and vessels in the arm (AN11.2)
- Describe the anatomical basis of venipuncture of cubital veins (AN11.3)
- Describe the anatomical basis of Saturday night paralysis (AN11.4)
- Identify and describe the boundaries and contents of the cubital fossa (AN11.5)
- Describe the anastomosis around the elbow joint (AN11.6)
INSTRUCTIONS
This self-directed learning guide covers the anatomy of the arm and cubital fossa. Read each section carefully, attempt all self-check quizzes, and complete the reflection activity. Estimated time: 28 minutes.
References
- OpenStax Anatomy and Physiology 2e, Chapters 8 and 11 (textbook)
- Gray's Anatomy for Students, 4th Edition — Chapter 7: Upper Limb (textbook)
- Gray's Anatomy 1918 (Bartleby) — Public Domain Illustrations (atlas)
- Clinically Oriented Anatomy (Moore, Dalley & Agur), 8th Edition (reference)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old man falls asleep on a park bench with his arm draped over the back rest after a long night out. When he wakes up, he cannot extend his wrist or fingers — his hand hangs limply, and he panics thinking he has had a stroke. In the emergency department at a government hospital in Chennai, the duty doctor reassures him: "Your brain is fine — it is a nerve in your arm that got compressed while you slept." This is Saturday night paralysis, and understanding it requires knowing exactly where the radial nerve travels through the arm. By the end of this guide, you will be able to explain why sleeping in that position causes this dramatic but reversible condition.
WHY THIS MATTERS
The arm is the gateway between the shoulder and the hand. Every nerve impulse that moves your fingers, every drop of blood that nourishes your palm, passes through this region. As a future doctor, you will:
- Take blood pressure using the brachial artery — the main artery of the arm
- Draw blood from the cubital fossa — the front of the elbow — in almost every patient you see
- Diagnose nerve injuries like Saturday night paralysis by knowing which nerve runs where
- Understand fracture complications: a broken humerus (the arm bone) can damage the radial nerve
You are currently studying Nerve and Muscle Physiology in Physiology — the action potentials and neuromuscular junctions you learn there are the signals travelling through the very nerves we will trace in this guide.
RECALL
Before we begin, let us recall what you already know:
- From NCERT Biology, you learned that muscles contract to produce movement, and nerves carry signals from the brain to muscles
- You know that arteries carry blood away from the heart, and veins return blood to the heart
- From your recent Anatomy sessions on the shoulder and axilla, you encountered the brachial plexus — the network of nerves that supplies the upper limb
- The humerus is the single long bone of the arm — you studied its features in the osteology module
Think of the arm as a corridor with two rooms (compartments), each with its own set of muscles, and with important cables (nerves) and pipes (blood vessels) running along specific paths. Knowing the layout of this corridor is what we will master today.
The Two Compartments of the Arm
The arm — the region between the shoulder and the elbow — is divided into two distinct compartments by walls of tough connective tissue called the medial intermuscular septum and lateral intermuscular septum. Think of these septa as partition walls in an office, separating the front team from the back team.
Anterior (flexor) compartment — the front of the arm. The muscles here flex (bend) the elbow and forearm. This compartment contains three muscles:
- Biceps brachii — the most superficial muscle, the one you see when someone "flexes." It has two heads: the long head arises from the supraglenoid tubercle of the scapula, and the short head from the coracoid process. Both heads merge into a single tendon that inserts into the radial tuberosity. Biceps is a powerful supinator (turns the palm upward) and flexor of the elbow.
- Brachialis — lies deep to biceps. It arises from the lower half of the anterior surface of the humerus and inserts into the coronoid process and tuberosity of the ulna. Brachialis is actually the strongest flexor of the elbow — think of biceps as the celebrity and brachialis as the workhorse.
- Coracobrachialis — a small muscle from the coracoid process to the mid-shaft of the humerus. It flexes and adducts the arm at the shoulder.
Posterior (extensor) compartment — the back of the arm. It contains just one muscle:
- Triceps brachii — the only extensor of the elbow. It has three heads: long head (from the infraglenoid tubercle of the scapula), lateral head (from the posterior surface of the humerus above the radial groove), and medial head (from the posterior surface below the radial groove). All three converge into a single tendon inserting into the olecranon of the ulna — the bony point of your elbow.
You can feel these muscles on yourself right now: place your right hand on your left upper arm. The bulge in front when you bend your elbow is biceps; the firm mass at the back when you straighten your elbow is triceps.
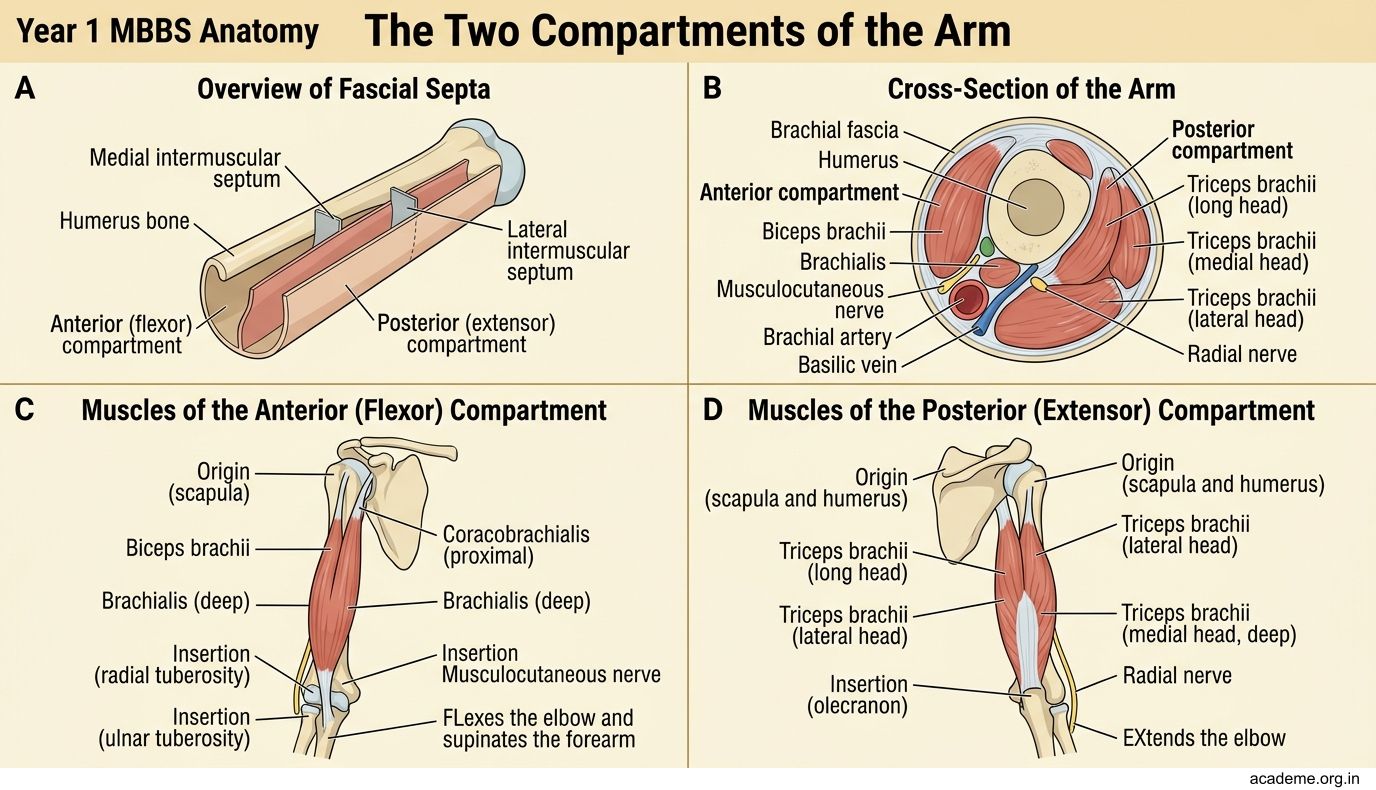
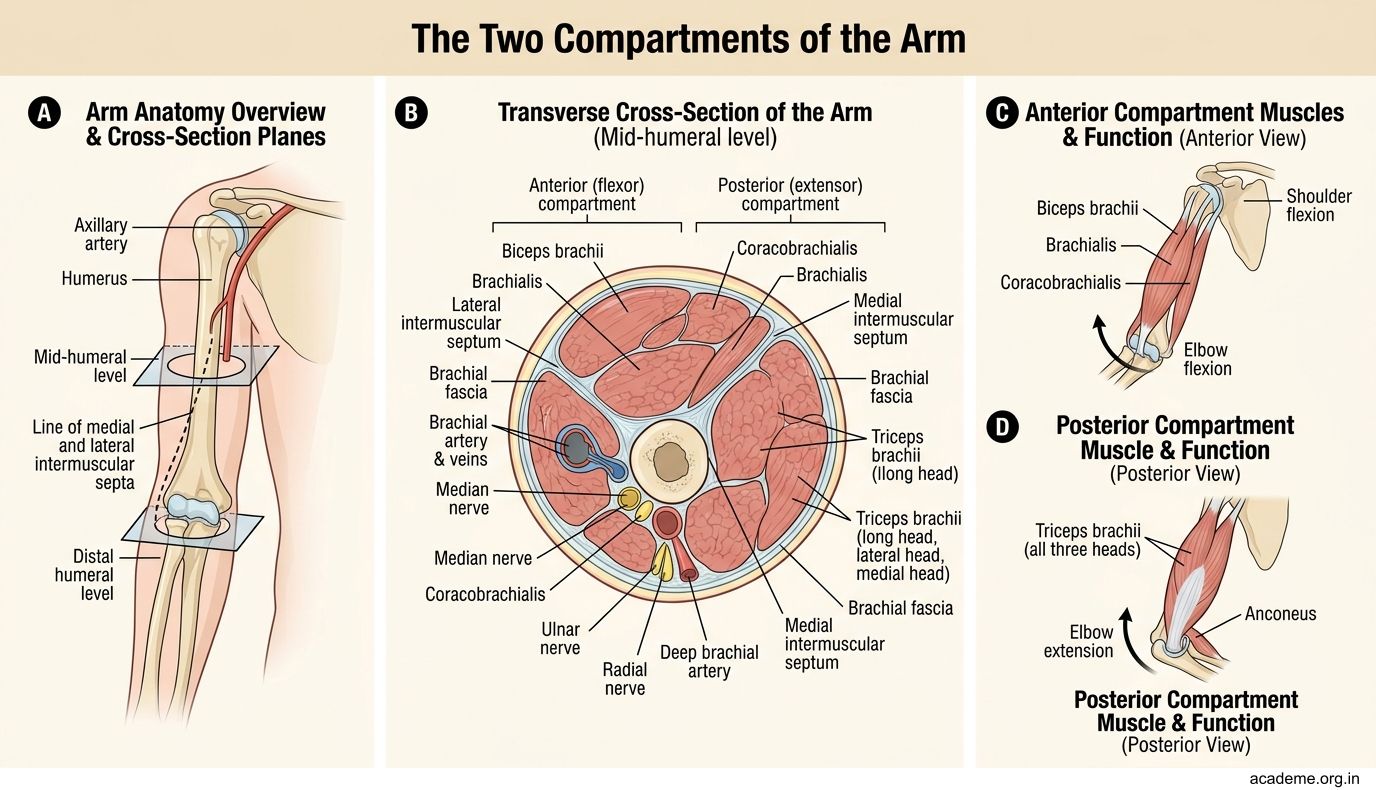

Figure: The Two Compartments of the Arm
SELF-CHECK — Arm Compartments Check
A patient cannot extend the elbow after a posterior humerus fracture. Which muscle is most likely affected?
A. Biceps brachii
B. Brachialis
C. Triceps brachii
D. Coracobrachialis
Reveal Answer
Answer: C. Triceps brachii
Which muscle is the strongest flexor of the elbow, despite being less visible than biceps?
A. Coracobrachialis
B. Brachialis
C. Pronator teres
D. Brachioradialis
Reveal Answer
Answer: B. Brachialis
Nerves and Vessels of the Arm
Three major nerves and one major artery travel through the arm. Picture them as cables and a water main running through our corridor.
Brachial artery — the continuation of the axillary artery. It begins at the lower border of teres major and runs along the medial side of the arm, closely related to the median nerve. It ends in the cubital fossa by dividing into the radial artery and ulnar artery. You feel the brachial artery pulse on the medial side of the arm, midway between the biceps tendon and the medial epicondyle — this is where you place your stethoscope when measuring blood pressure.
Key branches of the brachial artery:
• Profunda brachii (deep artery of the arm) — accompanies the radial nerve in the radial groove (also called the spiral groove) on the posterior surface of the humerus
• Superior ulnar collateral artery — accompanies the ulnar nerve behind the medial epicondyle
• Inferior ulnar collateral artery — participates in the anastomosis around the elbow
Median nerve — enters the arm lateral to the brachial artery, then crosses anterior to the artery (usually at mid-arm) to lie medial to it in the cubital fossa. Remember: median crosses the brachial artery from lateral to medial as it descends. It gives no branches in the arm — it is just passing through on its way to the forearm and hand.
Ulnar nerve — runs along the medial side of the arm in the anterior compartment initially, then pierces the medial intermuscular septum at mid-arm to enter the posterior compartment. It passes behind the medial epicondyle — this is the "funny bone" spot. Like the median nerve, the ulnar nerve gives no motor branches in the arm.
Radial nerve — the most important nerve for understanding Saturday night paralysis. It enters the posterior compartment from the axilla, spiralling around the humerus in the radial groove (spiral groove) with the profunda brachii artery. It supplies all muscles of the posterior compartment (triceps) and then pierces the lateral intermuscular septum to enter the anterior compartment in the lower arm. The radial groove is where the nerve is most vulnerable to compression or fracture injury.
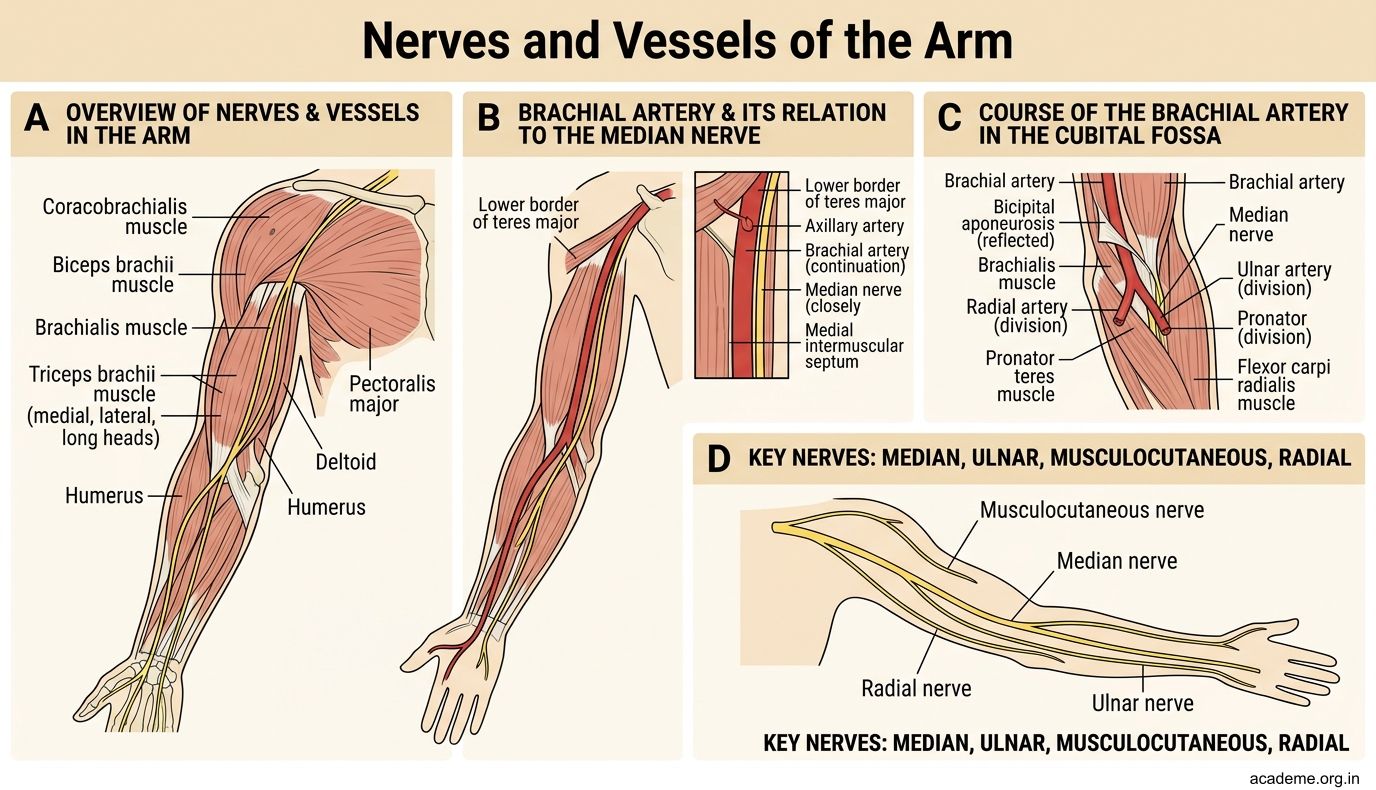

Figure: Nerves and Vessels of the Arm
CLINICAL PEARL
Mid-shaft humerus fracture and radial nerve injury: The radial nerve is directly in contact with the bone in the radial groove. A fracture of the mid-shaft of the humerus can directly damage or compress the radial nerve, causing wrist drop — the patient cannot extend the wrist or fingers. This is one of the most commonly tested clinical correlations in Anatomy examinations. Always check for wrist extension when examining a patient with a humerus fracture.
SELF-CHECK — Nerves & Vessels Check
The median nerve in the arm gives branches to:
A. Biceps brachii and brachialis
B. Pronator teres and flexor carpi radialis
C. No muscles — it passes through without branching
D. Triceps brachii (medial head)
Reveal Answer
Answer: C. No muscles — it passes through without branching
Which artery accompanies the radial nerve in the spiral groove of the humerus?
A. Brachial artery
B. Superior ulnar collateral artery
C. Profunda brachii artery
D. Inferior ulnar collateral artery
Reveal Answer
Answer: C. Profunda brachii artery
The Cubital Fossa — Boundaries and Contents
The cubital fossa is a triangular depression on the anterior surface of the elbow — the spot where blood samples are drawn. Understanding its boundaries and contents is essential for safe venipuncture.
Boundaries:
• Superior (base): An imaginary line connecting the two epicondyles of the humerus (medial and lateral)
• Lateral: Brachioradialis muscle
• Medial: Pronator teres muscle
• Floor: Brachialis muscle (superiorly) and supinator muscle (inferiorly)
• Roof: Skin, superficial fascia (containing the median cubital vein and the lateral cutaneous nerve of the forearm), deep fascia reinforced by the bicipital aponeurosis (a flat tendon spreading from the biceps tendon medially)
A helpful mnemonic for the contents from lateral to medial: Really Need Burgers Today
• Radial nerve (and its terminal branches: posterior interosseous and superficial branch)
• N — biceps teNdon
• Brachial artery (which divides here into radial and ulnar arteries)
• T — median nerve (passes between the Two heads of pronator Teres just below)
The bicipital aponeurosis (also called the lacertus fibrosus) is clinically important — it separates the superficial cubital veins from the deeper brachial artery and median nerve, providing a protective layer during venipuncture.
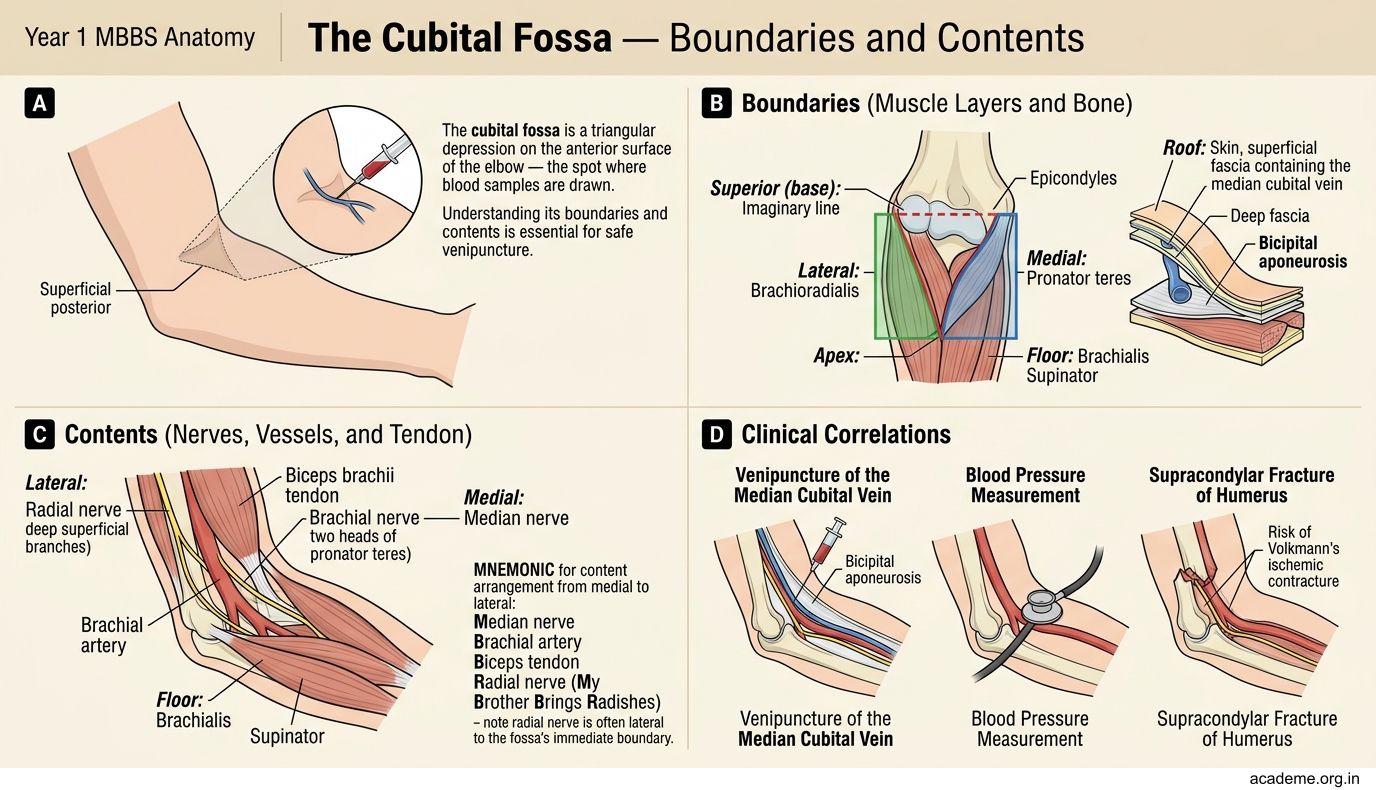

Figure: The Cubital Fossa — Boundaries and Contents