Page 1 of 4
AN18.1-7 | Knee joint, Anterior compartment of leg & dorsum of foot — SDL Guide
Learning Objectives
- Describe the muscles of the anterior compartment of the leg with their attachments, nerve supply, and actions (AN18.1)
- Trace the deep peroneal nerve and anterior tibial/dorsalis pedis arteries through the anterior compartment (AN18.2)
- Explain the anatomical basis of foot drop — which nerve, which muscles, what movements are lost (AN18.3)
- Describe the knee joint — type, articular surfaces, capsule, ligaments, movements, nerve supply, and anastomosis around the knee (AN18.4)
- Explain the locking and unlocking mechanism of the knee joint with the role of popliteus (AN18.5)
- Describe knee joint injuries — unhappy triad, anterior drawer test, medial collateral ligament tears, and their anatomical basis (AN18.6)
- Explain the anatomical basis of osteoarthritis of the knee with its radiological and clinical correlates (AN18.7)
INSTRUCTIONS
This module covers three linked regions: the anterior leg, the dorsum of the foot, and the knee joint. The knee joint section is the most detailed — it is a high-yield topic for both examinations and clinical practice. Complete each self-check before proceeding.
References
- Gray's Anatomy for Students (Drake et al.) — Lower Limb (Textbook)
- BD Chaurasia's Human Anatomy Vol. 2 — Leg and Foot (Textbook)
- Clinically Oriented Anatomy (Moore et al.) — Knee, Leg, Foot (Textbook)
- OpenStax Anatomy and Physiology 2e — Joints (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 22-year-old football player from a village near Vellore is brought to casualty after a tackle during a match. His right knee is swollen, he cannot bear weight, and he says he heard a "pop" when he fell. On examination, there is a haemarthrosis, the Lachman test is positive, and the medial side of the knee is tender.
Which structures were injured? What is the classic triad that your professor will ask about? How will you stabilise this knee before referring him?
By the end of this module, the anatomy behind every clinical test at the knee will make complete sense.
WHY THIS MATTERS
The knee is the most commonly injured major joint in India — from road traffic accidents to sports injuries to the epidemic of osteoarthritis in the elderly population. As a doctor you will:
- Perform the anterior drawer test and Lachman test in the Emergency Department
- Recognise foot drop — the most common peroneal nerve palsy, seen after fibular neck fractures and knee surgeries
- Counsel patients with osteoarthritis — now a leading cause of disability in Indians over 50
- Identify anterior compartment syndrome — a surgical emergency requiring fasciotomy within hours
- Understand why the knee locks and how a physiotherapist unlocks it
This is anatomy you will use every single working day.
RECALL
From your earlier sessions:
- The femur articulates with the tibia (weight-bearing) and the patella (anteriorly)
- The fibula does NOT carry weight; its head is at the neck of the fibula where the common peroneal nerve winds around
- The quadriceps (L3, L4) extend the knee; hamstrings (L5, S1) flex it
- The popliteal artery (deepest structure in the popliteal fossa) continues as the anterior tibial artery (through the interosseous membrane) and posterior tibial artery
These facts will anchor everything in this module.
Anterior Compartment of the Leg
The anterior compartment of the leg lies between the tibia (medially), fibula (laterally), interosseous membrane (posteriorly), and the deep fascia of the leg (anteriorly).

Figure: Neurovascular bundle

Figure: Anterior Compartment of the Leg
Four muscles (from medial to lateral):
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Tibialis anterior | Upper 2/3 of lateral tibia + interosseous membrane | Medial cuneiform + base of 1st metatarsal | Dorsiflexion + inversion | Deep peroneal (L4, L5) |
| Extensor hallucis longus | Middle 1/2 of fibula + interosseous membrane | Base of distal phalanx of big toe | Extend big toe; dorsiflexion | Deep peroneal (L4, L5) |
| Extensor digitorum longus | Upper 3/4 of fibula + interosseous membrane | Middle and distal phalanges of toes 2–5 | Extend toes 2–5; dorsiflexion | Deep peroneal (L4, L5) |
| Peroneus (fibularis) tertius | Lower 1/3 of fibula | Base of 5th metatarsal | Dorsiflexion + eversion | Deep peroneal (L4, L5) |
Key fact: All four muscles are supplied by the deep peroneal (fibular) nerve (L4, L5). All dorsifllex the foot. If this nerve is injured → foot drop.
Neurovascular bundle:
- Deep peroneal nerve: Enters the anterior compartment by winding around the neck of fibula (with the common peroneal nerve), then passes with the anterior tibial artery between extensor hallucis longus and tibialis anterior
- Anterior tibial artery: Branch of the popliteal artery; passes through the interosseous membrane; becomes the dorsalis pedis at the ankle (felt between extensor hallucis longus and extensor digitorum tendons — a clinical pulse point)
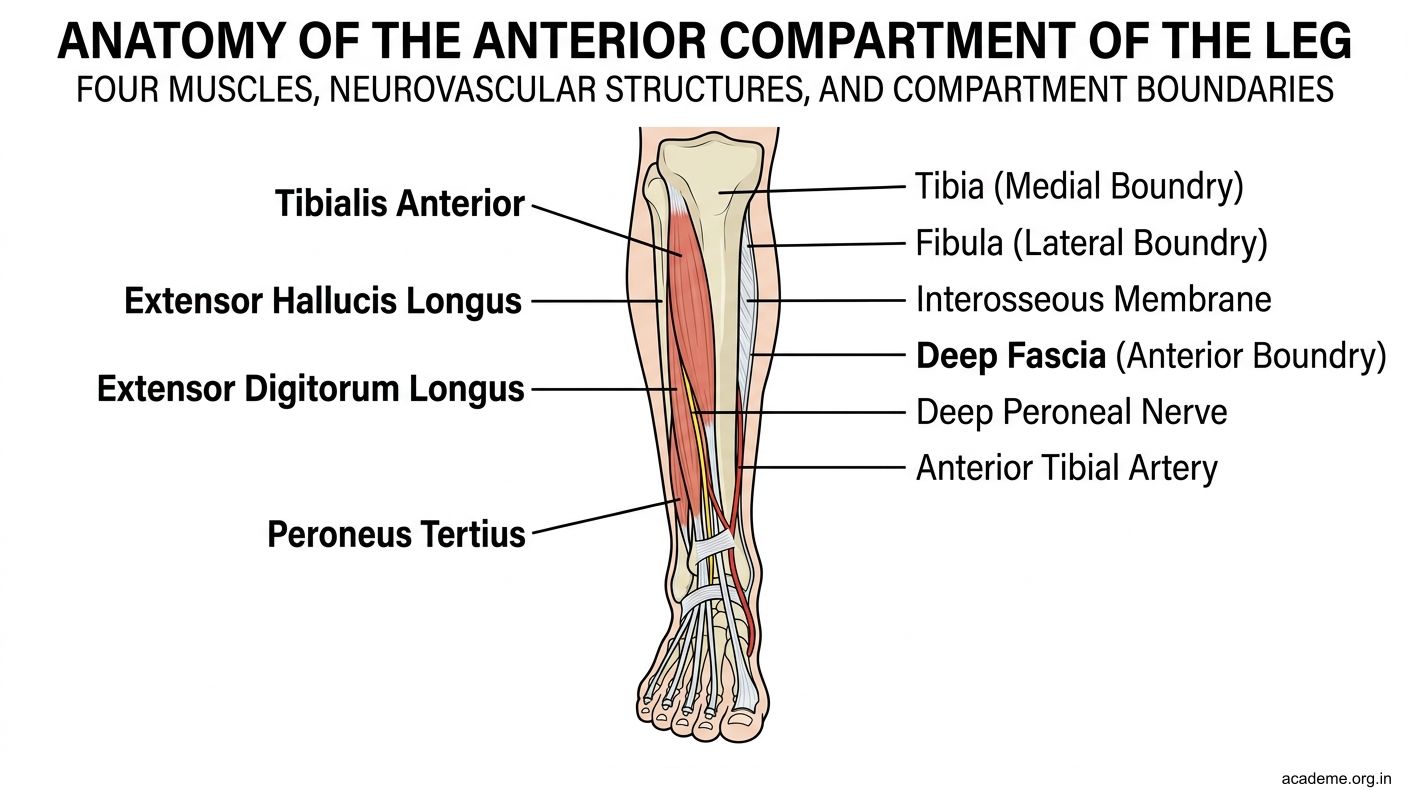
Figure: Anterior Compartment of the Leg
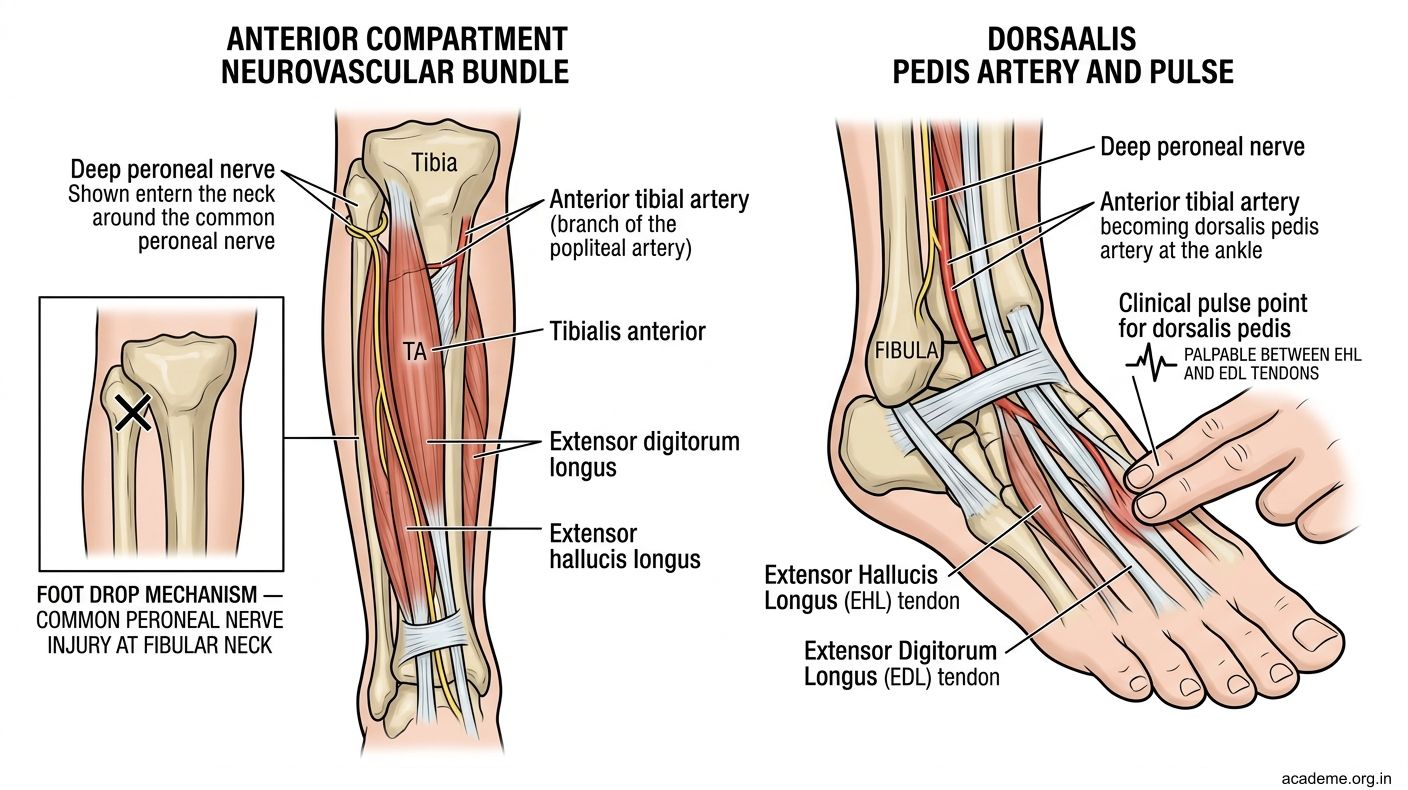
Figure: Neurovascular bundle

Figure: Anterior Compartment Syndrome
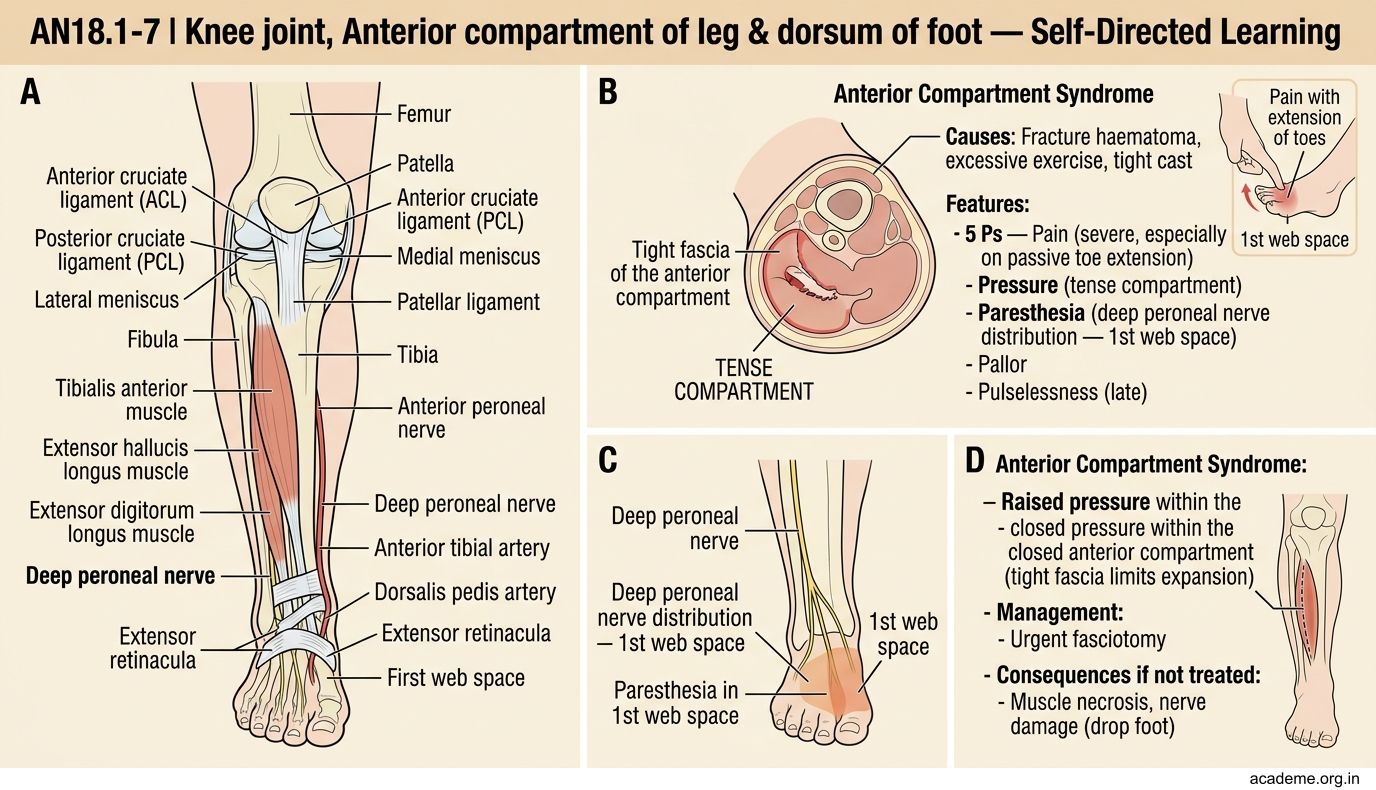
Figure: Anterior Compartment Syndrome
CLINICAL PEARL
Foot Drop (AN18.3):
- The patient cannot dorsiflex the foot — the foot hangs in plantar flexion and the toes drag on the ground during walking
- The steppage gait: the patient lifts the knee high to clear the dragging toes
- Caused by deep peroneal nerve (or common peroneal nerve) injury
- Most common site: neck of fibula (fibular head fracture, tight below-knee cast, prolonged crossed-leg sitting, knee surgery)
- All four anterior compartment muscles are paralysed; sensation lost in the first web space
Anterior Compartment Syndrome:
- Raised pressure within the closed anterior compartment (tight fascia limits expansion)
- Causes: fracture haematoma, excessive exercise, tight cast
- Features: 5 Ps — Pain (severe, especially on passive toe extension), Pressure (tense compartment), Paresthesia (deep peroneal nerve distribution — 1st web space), Pallor, Pulselessness (late)
- Treatment: Emergency fasciotomy — delay beyond 6 hours risks permanent muscle necrosis and foot drop
- In India: seen after road traffic accidents, snake bites (venom-induced swelling), and crush injuries
The Knee Joint — Structure and Stabilisers
The knee joint is the largest and most complex joint in the body. It is a modified hinge joint (condylar type), allowing flexion/extension with some axial rotation.

Figure: Capsule and Synovial Membrane

Figure: The Knee Joint — Structure and Stabilisers
Articular surfaces:
- Medial and lateral condyles of femur + medial and lateral condyles of tibia + patella (femoropatellar joint)
- Articular cartilage covers all surfaces; fibrocartilaginous menisci deepen the joint and act as shock absorbers
Menisci:
- Medial meniscus: C-shaped, attached to medial collateral ligament (less mobile → more commonly torn)
- Lateral meniscus: O-shaped (more complete ring), NOT attached to lateral collateral ligament (more mobile → less commonly torn)
Capsule and Synovial Membrane:
- The synovial membrane is the most extensive in the body — it forms a suprapatellar pouch under quadriceps
- The capsule is deficient anteriorly (replaced by quadriceps tendon + patella + patellar ligament)
Ligaments:
Extracapsular:
- Medial (tibial) collateral ligament (MCL): Resists valgus stress; attached to medial meniscus
- Lateral (fibular) collateral ligament (LCL): Resists varus stress; NOT attached to lateral meniscus
- Patellar ligament: Quadriceps tendon continuation; attaches to tibial tuberosity
Intracapsular (but extrasynovial):
- Anterior cruciate ligament (ACL): From anterior intercondylar area of tibia → medial surface of lateral femoral condyle; prevents anterior tibial displacement + hyperextension
- Posterior cruciate ligament (PCL): From posterior intercondylar area of tibia → lateral surface of medial femoral condyle; prevents posterior tibial displacement; stronger than ACL
Nerve supply: Branches of femoral, common peroneal, obturator, and tibial nerves (Hilton's law — nerve to the joint = nerve to the muscles acting on the joint)
Anastomosis around the knee: Formed by genicular branches of popliteal artery + descending genicular branch of femoral + recurrent branches of anterior tibial. Allows collateral circulation when popliteal artery is ligated above the genicular branches.

Figure: The Knee Joint — Structure and Stabilisers
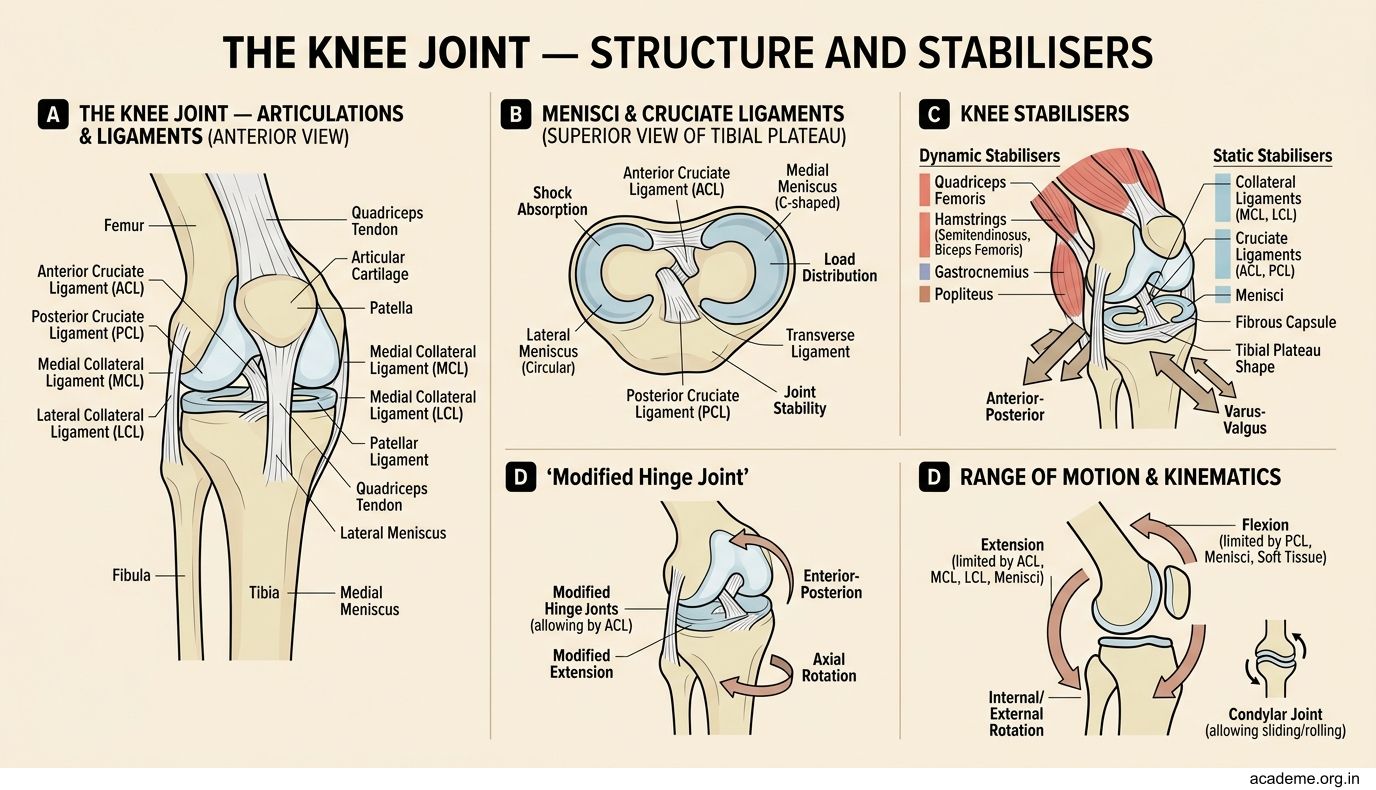
Figure: Articular surfaces
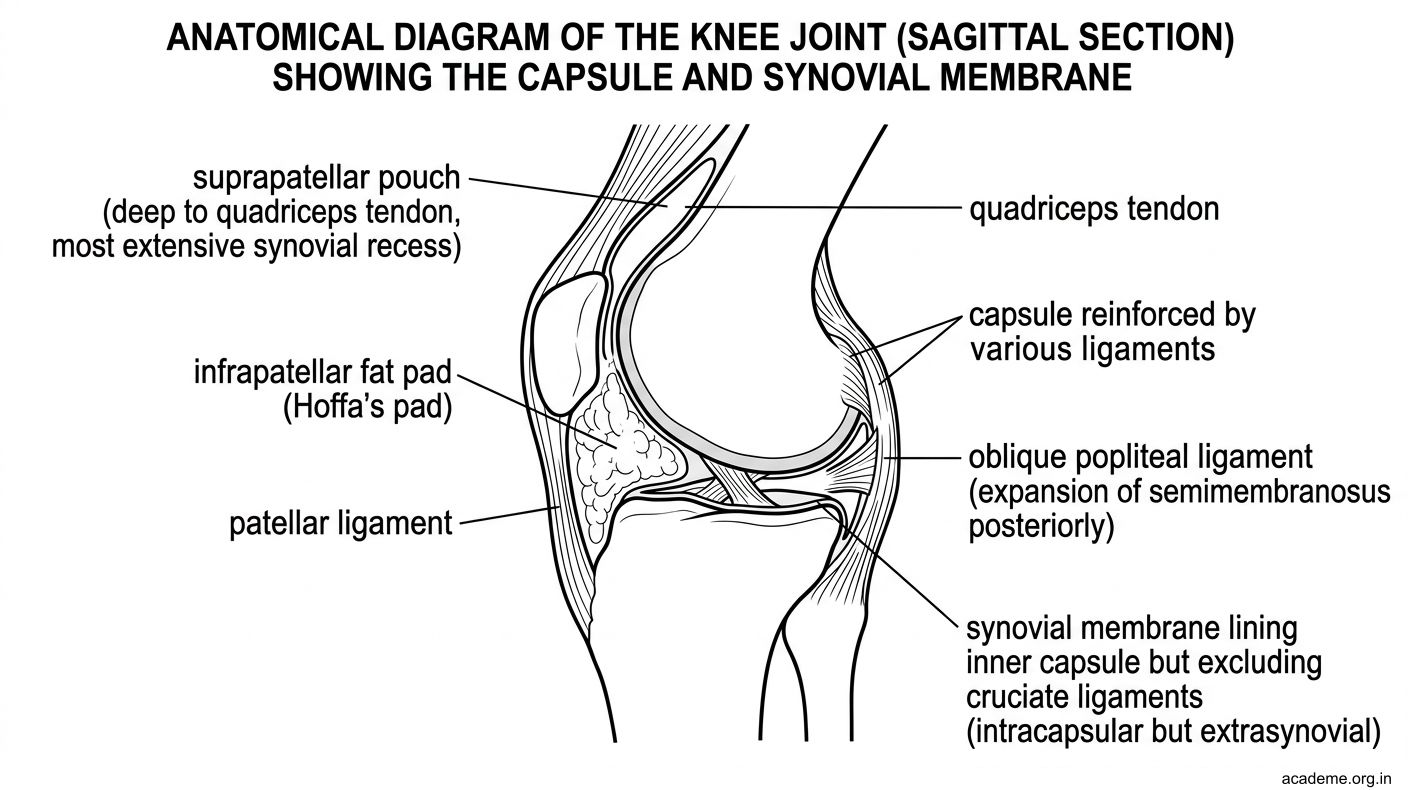
Figure: Capsule and Synovial Membrane
Locking and Unlocking of the Knee
Locking of the knee (AN18.5) — NOT pathological locking; this is the physiological "screw-home" mechanism.

Figure: Clinical relevance

Figure: Locking and Unlocking of the Knee
Why it happens:
- The medial femoral condyle is longer than the lateral condyle
- As the knee approaches full extension, the lateral condyle finishes its movement before the medial one does
- The tibia is forced to rotate laterally on the femur (or femur rotates medially on tibia) in the last 5–10° of extension
- This brings the articular surfaces into maximal congruence — the knee is "locked" (fully extended, most stable)
- In this position, the knee requires minimal muscular effort to stay extended (saves energy during standing)
Unlocking the knee (to begin flexion):
- Popliteus is the "key" that unlocks the knee
- Popliteus rotates the tibia medially (or femur laterally) to "unscrew" the joint → flexion can begin
- Popliteus is supplied by the tibial nerve (L4, L5, S1)
Clinical relevance: In a locked knee (pathological), the joint is stuck in slight flexion due to a torn meniscus fragment acting as a block. This is different from the physiological locked position (full extension).
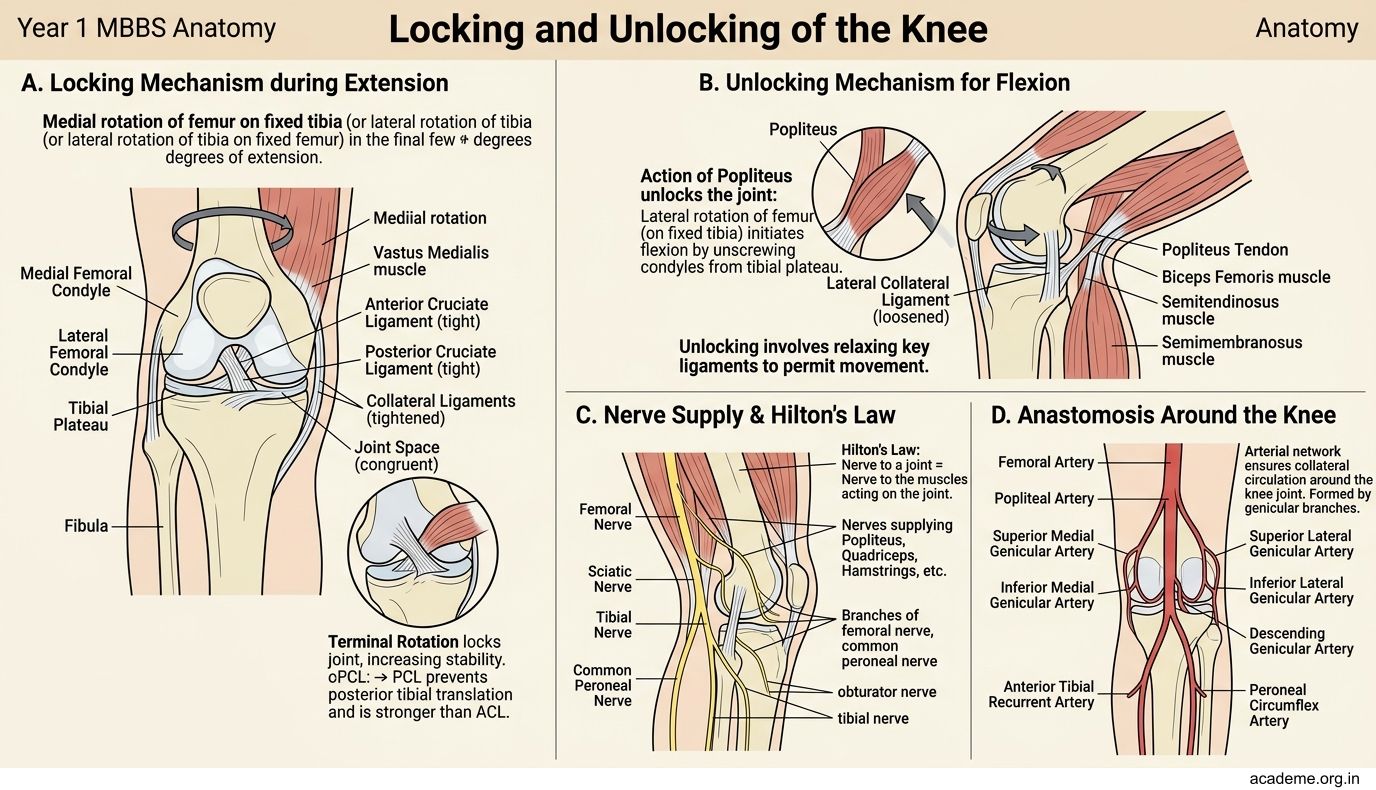
Figure: Locking and Unlocking of the Knee
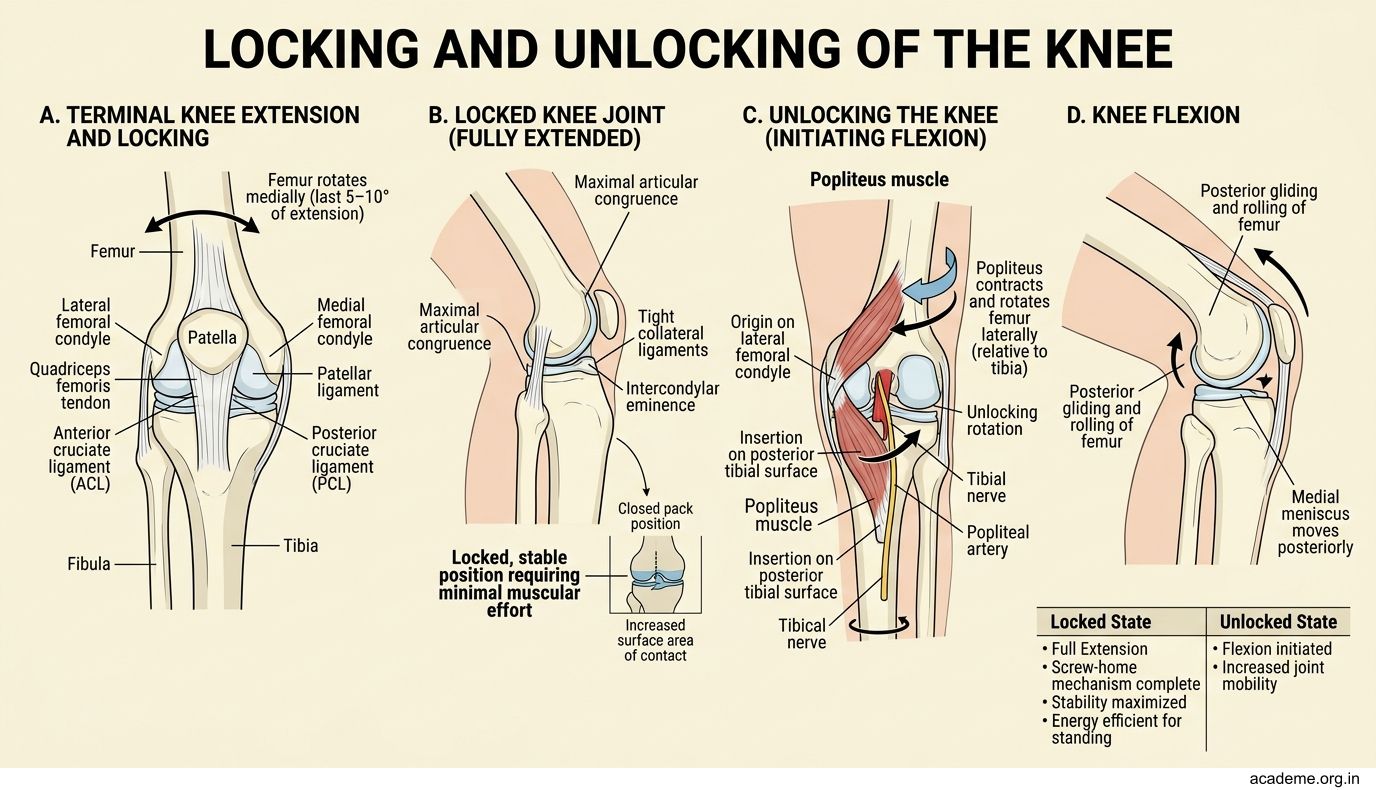
Figure: Clinical relevance
SELF-CHECK — 2
During the last degrees of knee extension, which movement of the tibia occurs to lock the knee?
A. Medial rotation of tibia
B. Lateral rotation of tibia
C. Anterior sliding of tibia
D. Posterior sliding of tibia
Reveal Answer
Answer: B. Lateral rotation of tibia
Which ligament prevents anterior displacement of the tibia on the femur?
A. Posterior cruciate ligament
B. Medial collateral ligament
C. Anterior cruciate ligament
D. Patellar ligament
Reveal Answer
Answer: C. Anterior cruciate ligament
Knee Joint Injuries & Clinical Tests
The Unhappy Triad (O'Donoghue's Triad) (AN18.6):
- ACL + MCL + Medial Meniscus — the classic sports injury
- Mechanism: Valgus force with the knee slightly flexed and tibia externally rotated (e.g., a lateral tackle in football that pushes the knee inward while the foot is planted)
- The MCL tears first; because the medial meniscus is attached to the MCL, it tears with it; the ACL then gives way
- Features: Haemarthrosis (blood in joint — immediate swelling), pain, instability, positive anterior drawer test

Figure: Genu varum vs genu valgum

Figure: Why medial compartment is affected first

Figure: Anatomical basis

Figure: Medial vs Lateral Meniscus tears

Figure: Clinical Tests for Knee Ligaments
Clinical Tests for Knee Ligaments:
| Test | What it tests | Positive finding |
|---|---|---|
| Anterior drawer test | ACL integrity | Tibia slides > 5 mm anteriorly on femur (knee at 90°) |
| Lachman test | ACL (more sensitive) | Anterior tibial translation at 20–30° flexion |
| Posterior drawer test | PCL integrity | Tibia slides posteriorly |
| Valgus stress test | MCL | Pain/gap on medial side with valgus force |
| Varus stress test | LCL | Pain/gap on lateral side with varus force |
| McMurray's test | Meniscus tear | Click/pain on medial rotation + extension (lateral meniscus) or lateral rotation + extension (medial meniscus) |
Medial vs Lateral Meniscus tears:
- Medial is more commonly torn (less mobile; attached to MCL)
- A torn fragment can flip into the joint → "locked knee" (cannot extend fully; painful block)
Haemarthrosis (blood in the joint, immediate swelling) = ligament/cruciate injury or fracture
Effusion (fluid, swells over hours) = meniscus tear or mild sprain
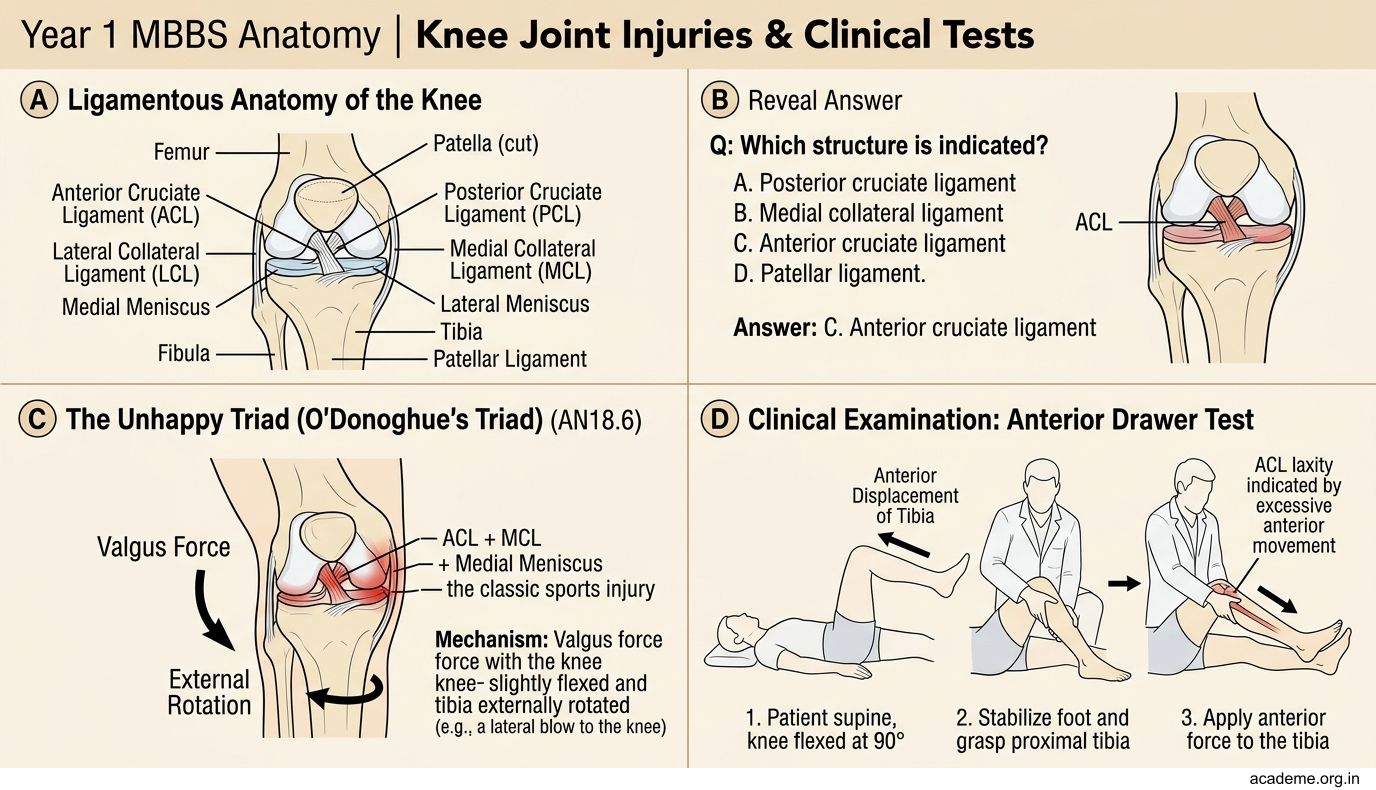
Figure: Clinical Tests for Knee Ligaments
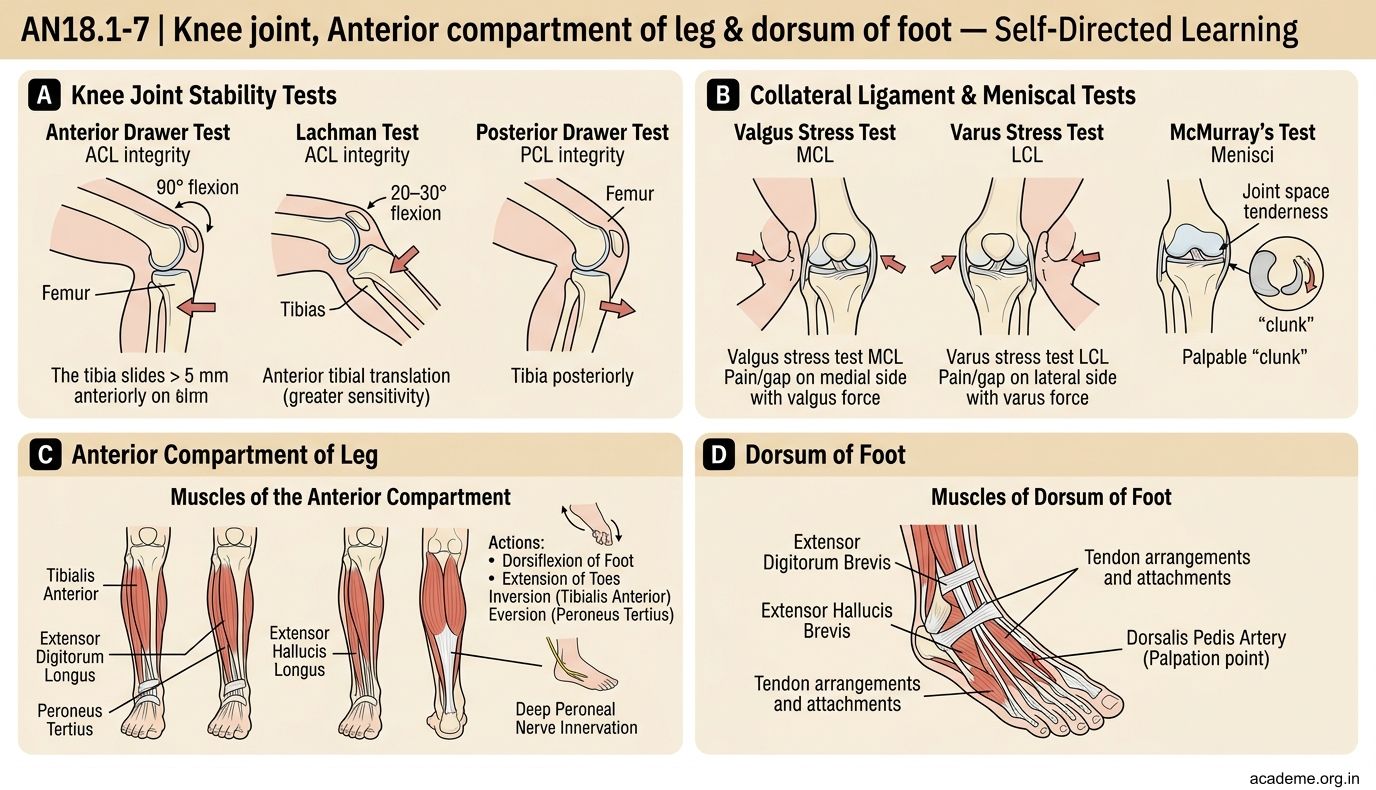
Figure: Medial vs Lateral Meniscus tears
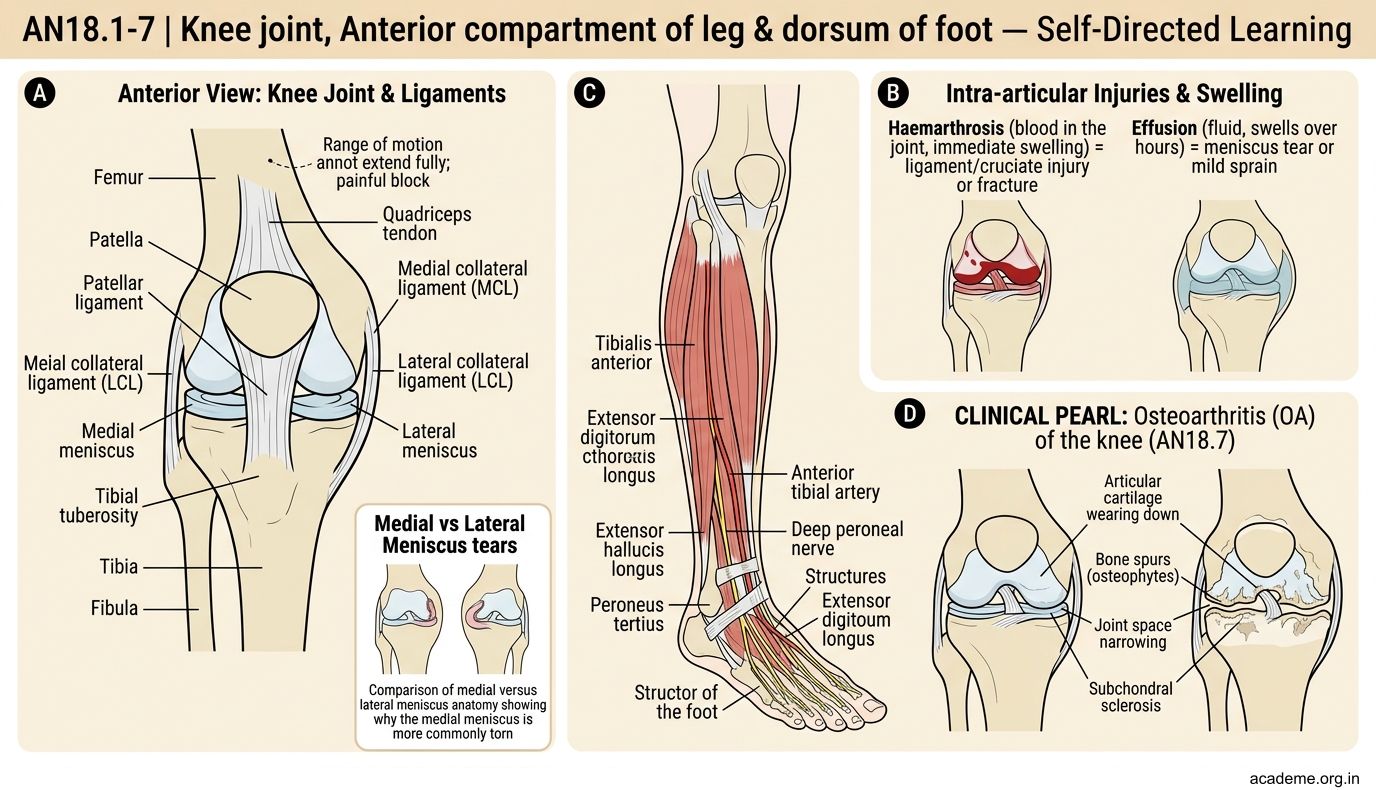
Figure: Anatomical basis
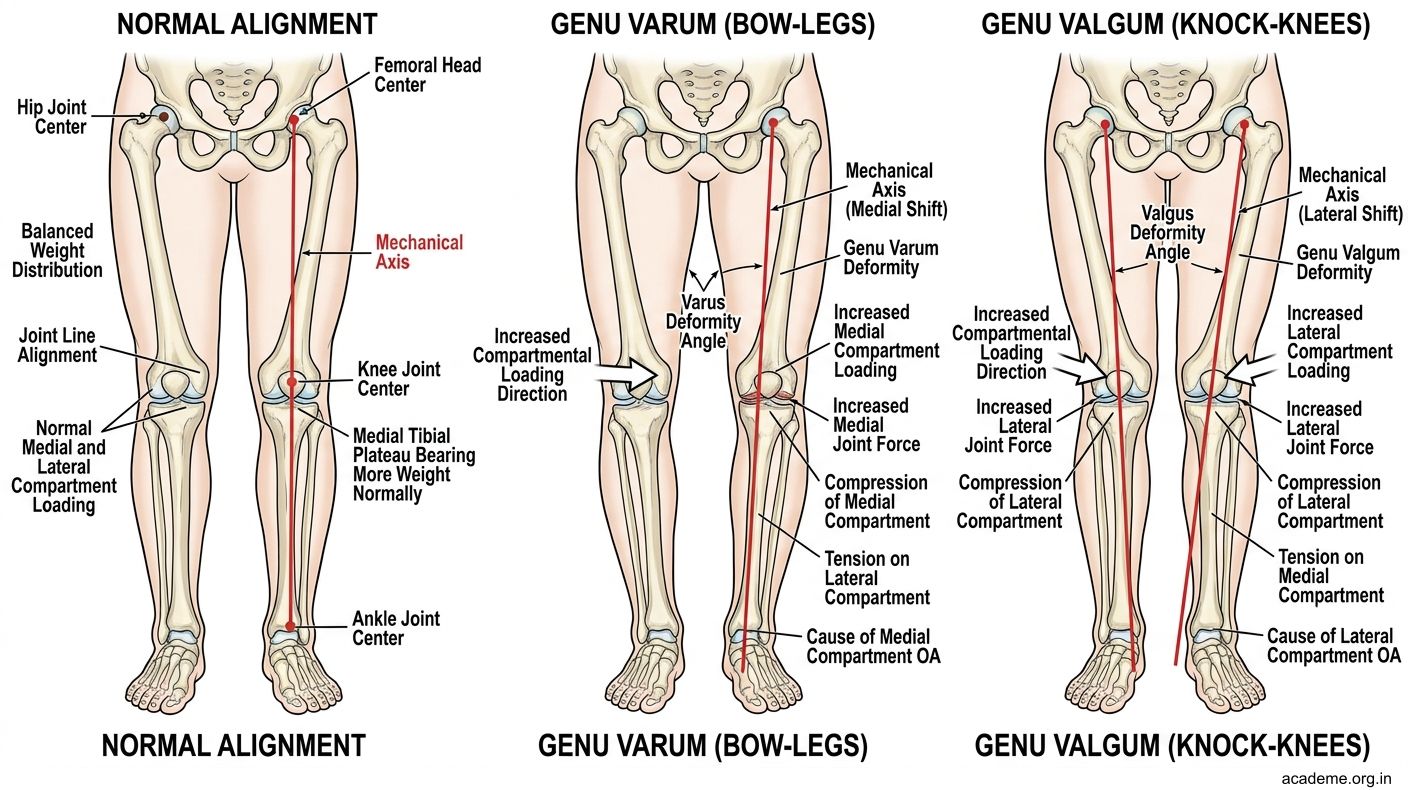
Figure: Why medial compartment is affected first
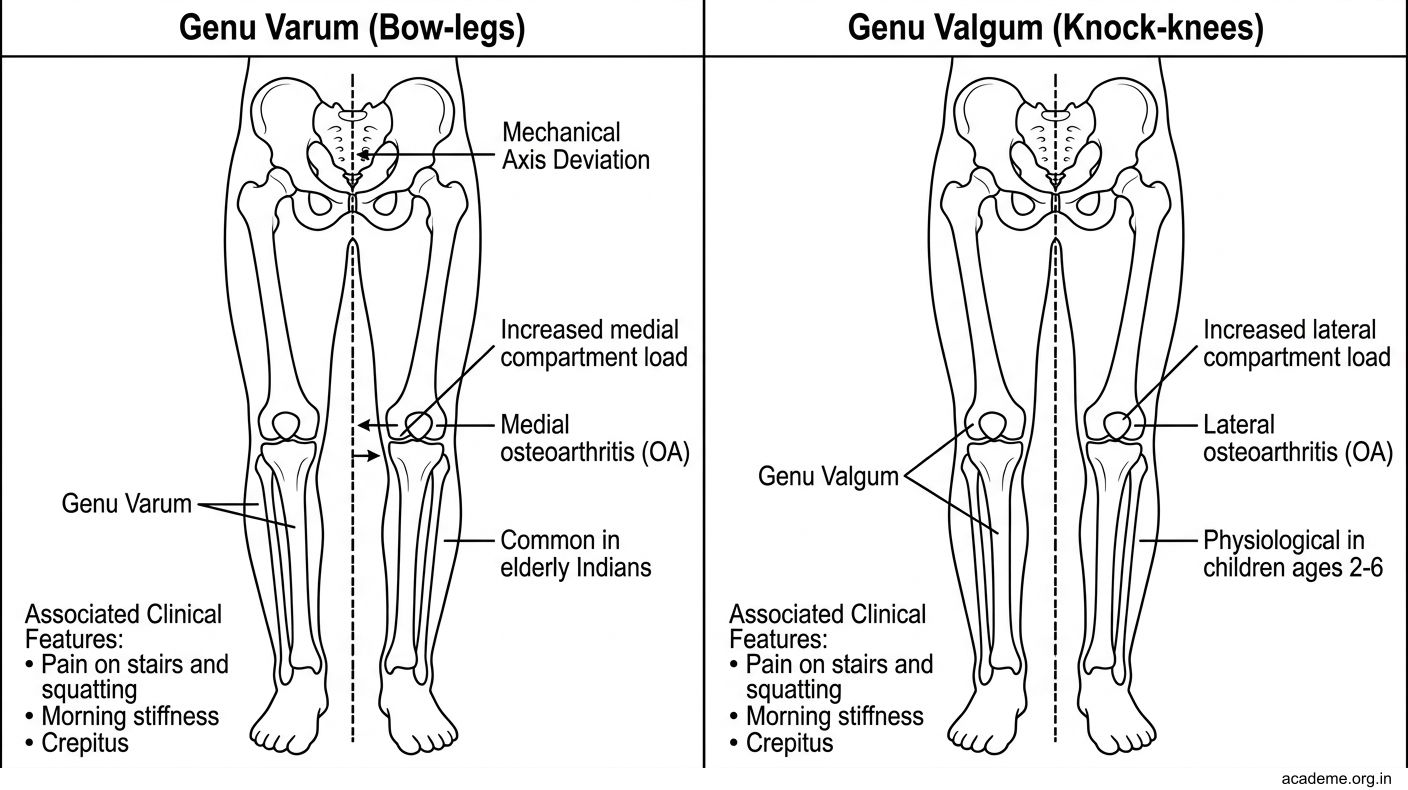
Figure: Genu varum vs genu valgum
CLINICAL PEARL
Osteoarthritis (OA) of the knee (AN18.7) is the most common joint disease in India, affecting nearly 25% of adults over 65.
Anatomical basis:
- Progressive destruction of articular cartilage (avascular, cannot regenerate)
- Subchondral bone becomes exposed and eburnated (ivory-hard)
- Osteophytes (bony spurs) form at joint margins
- Synovial inflammation → joint effusion → pain
Radiological features (LOSS):
- Loss of joint space (cartilage destruction)
- Osteophytes (bony spurs at margins)
- Subchondral sclerosis (bone hardening under cartilage)
- Subchondral cysts
Why medial compartment is affected first: Most body weight passes through the medial tibial plateau. In varus deformity (bow-legs), medial loading is even greater — a vicious cycle.
Genu varum vs genu valgum:
- Varus (bow-legs): increased medial compartment loading → medial OA
- Valgum (knock-knees): increased lateral compartment loading → lateral OA
Clinical: Pain worse on stairs and squatting (Indians who squat for toileting or religious observance are at particular risk), morning stiffness < 30 minutes, crepitus, bony enlargement.
SELF-CHECK — 3
The "unhappy triad" of knee injury classically involves injury to which three structures?
A. ACL, PCL, and lateral meniscus
B. ACL, MCL, and medial meniscus
C. PCL, LCL, and lateral meniscus
D. ACL, LCL, and medial meniscus
Reveal Answer
Answer: B. ACL, MCL, and medial meniscus
A 60-year-old woman with knee pain undergoes X-ray. You see joint space narrowing predominantly on the medial side, subchondral sclerosis, and osteophytes at the medial tibial plateau. The most likely diagnosis is:
A. Rheumatoid arthritis
B. Septic arthritis
C. Osteoarthritis (medial compartment)
D. Anterior cruciate ligament tear
Reveal Answer
Answer: C. Osteoarthritis (medial compartment)
REFLECT
A 30-year-old kabaddi player sustains a valgus knee injury. He has immediate swelling, medial pain, and a positive anterior drawer test. Describe: (a) the structures injured and why, (b) what you look for on examination to assess each structure, and (c) what you would explain to the patient about his recovery.
KEY TAKEAWAYS
Anterior Compartment of Leg
- Four muscles: tibialis anterior, EHL, EDL, peroneus tertius — all deep peroneal nerve (L4, L5)
- All dorsiflex the foot; injury → foot drop + steppage gait
- Anterior compartment syndrome: emergency fasciotomy needed
Dorsalis Pedis Artery
- Continuation of anterior tibial artery; palpated between EHL and EDL tendons on dorsum of foot
Knee Joint
- Modified hinge (condylar); largest joint; most complex
- Medial meniscus = C-shaped, attached to MCL (less mobile, more torn)
- Lateral meniscus = O-shaped, not attached to LCL (more mobile, less torn)
- ACL: prevents anterior tibial displacement; PCL: prevents posterior displacement
Locking/Unlocking
- Lock: lateral tibial rotation in last 5–10° extension (screw-home)
- Unlock: popliteus medially rotates tibia (tibial nerve L4, L5, S1)
Unhappy Triad: ACL + MCL + Medial Meniscus (valgus force with external rotation)
Osteoarthritis: LOSS (Loss of space, Osteophytes, Subchondral Sclerosis, Subchondral cysts); medial compartment most affected