Page 1 of 9
AN21.1-11 | Thoracic cage — SDL Guide
Learning Objectives
- Describe the parts and features of the sternum and identify the sternal angle as a clinical landmark (AN21.1)
- Classify ribs into typical and atypical, and describe their distinguishing features (AN21.2)
- Describe the features of typical and atypical thoracic vertebrae (AN21.3)
- Describe the boundaries and clinical significance of the thoracic inlet and outlet (AN21.4)
- Describe the layers of the intercostal space — muscles, membranes, and their arrangement (AN21.5)
- Describe the course and distribution of a typical intercostal nerve and identify atypical intercostal nerves (AN21.6)
- Describe the intercostal vessels and their clinical significance (AN21.7)
- Describe the joints of the thorax — costovertebral and costotransverse joints (AN21.8)
- Explain the mechanics of respiration — pump-handle and bucket-handle movements (AN21.9)
- Describe the costochondral and interchondral joints (AN21.10)
- Describe the mediastinum and its subdivisions (AN21.11)
INSTRUCTIONS
This module covers the thoracic cage — the bony and muscular framework that protects your heart and lungs and makes breathing possible. We'll start with the bones you can feel on your own chest and build outward to how the whole cage moves during respiration.
Parallel connections: In Physiology, you're studying respiratory mechanics (PY6) — the lung compliance and airway resistance that complement the chest wall movements you learn here. In Biochemistry, you're learning about carbohydrate metabolism (BI3) — the energy pathways that fuel the intercostal muscles and diaphragm every single breath you take.
References
- OpenStax Anatomy and Physiology 2e, Chapter 7: Axial Skeleton (textbook (CC BY 4.0))
- B.D. Chaurasia's Human Anatomy, Vol. 1, Ch 13-14: Thoracic Wall (textbook)
- Netter's Atlas of Human Anatomy, 8th ed., Plates 185–199 (Thorax) (atlas)
- Gray's Anatomy for Students, 4th ed., Chapter 3: Thorax (textbook)
Version 2.0 | NMC CBUC 2024, Adapted from OpenStax A&P 2e (CC BY 4.0)
CLINICAL SCENARIO
Take a deep breath. Your chest just expanded in two directions simultaneously — forwards AND sideways. How? The answer is in how your ribs are shaped and hinged. Place your fingertips on the centre of your chest. That hard, flat bone is the sternum — the keystone of your thoracic cage. Now slide your fingers sideways. You're counting ribs — each one curved like a handle on a bucket. By the end of this section, you'll understand why a surgeon counts ribs from the sternal angle and why a fracture of the 1st rib is an emergency while a fracture of the 7th rib might just need painkillers.
WHY THIS MATTERS
As a doctor, the thoracic cage matters to you every single day. In the emergency department, you'll count intercostal spaces to insert a chest drain. In the ward, you'll auscultate the lungs and heart by placing your stethoscope in specific intercostal spaces. In surgery, the sternum is split open (median sternotomy) for cardiac bypass. And in radiology, you'll read chest X-rays — the most common imaging investigation in medicine — where knowing normal rib anatomy helps you spot fractures, tumours, and cervical ribs.
RECALL
From your study of the body wall and upper limb, you know that bones have processes (projections), fossae (hollows), and foramina (holes). You also know that joints can be synovial (movable, with a cavity) or cartilaginous (connected by cartilage, limited movement). Both types are found in the thoracic cage. We'll build on your understanding of how the axial skeleton provides attachments for muscles and protects vital organs.
The Sternum — Your Chest's Keystone (AN21.1)
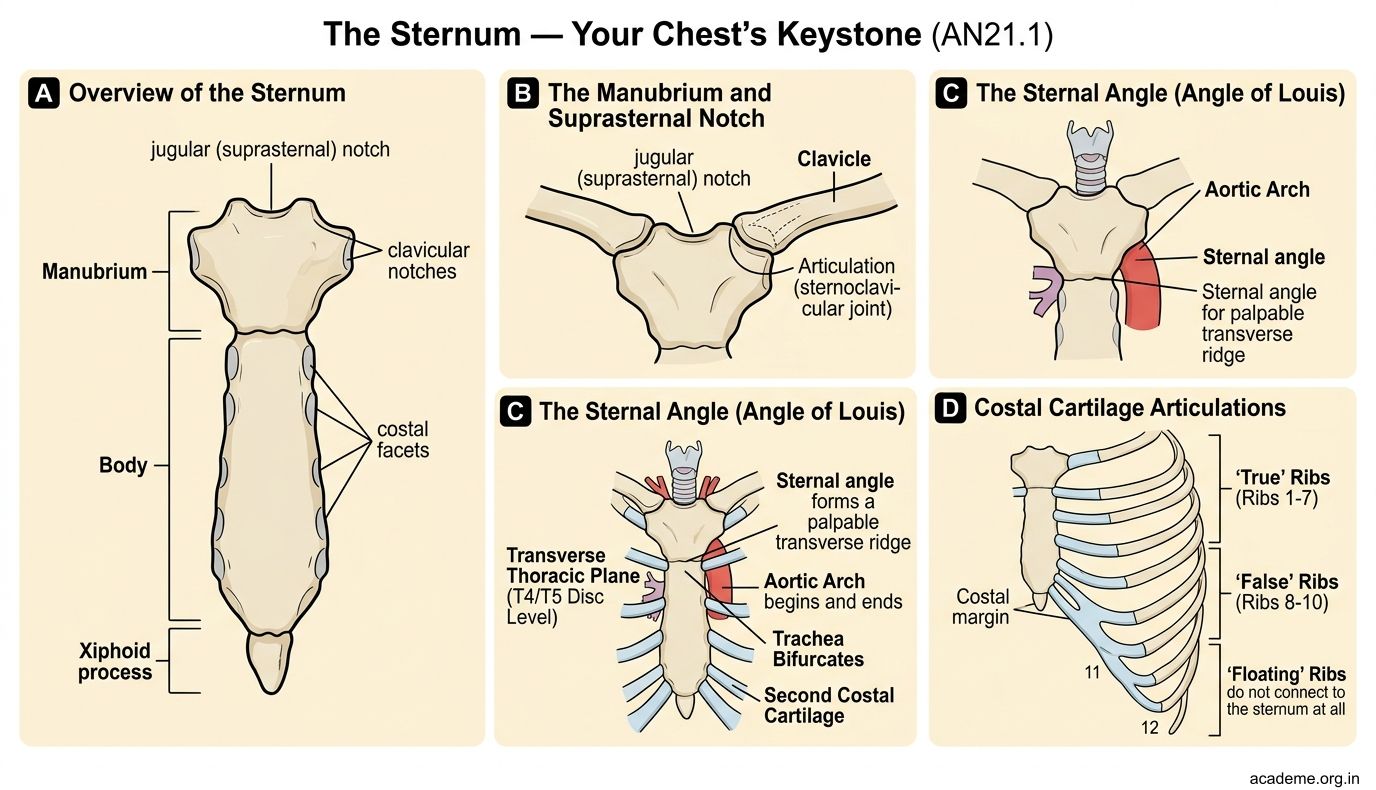
The sternum is a flat bone in the centre of the anterior chest wall. It has three parts, from top to bottom:
- Manubrium — the broad upper part. It has a notch at its top called the jugular (suprasternal) notch — you can feel this as the dip at the base of your neck between the two collarbones. On each side, the manubrium articulates with the clavicle (sternoclavicular joint) and the 1st costal cartilage (1st rib attachment). It also receives the upper half of the 2nd costal cartilage.
- Body — the longest part, articulates with costal cartilages of ribs 2–7. The body has transverse ridges on its anterior surface — remnants of the four sternebrae (segments) that fuse during development.
- Xiphoid process — a small, pointed projection at the lower end. It's cartilaginous in young adults and ossifies by age 40. The xiphoid process is a danger zone during CPR — pressing on it can fracture it and lacerate the liver.
The sternal angle (Angle of Louis) — the most important clinical landmark on the sternum. It's the palpable ridge where the manubrium meets the body. You can feel it as a horizontal ridge about 5 cm below the jugular notch.
Why is the sternal angle so important? Because it marks:
1. The level of the 2nd costal cartilage — your starting point for counting ribs
2. The level where the trachea bifurcates into right and left main bronchi
3. The level where the aortic arch begins and ends
4. The level of the T4/T5 intervertebral disc posteriorly
5. The boundary between the superior and inferior mediastinum
Ribs — Typical and Atypical (AN21.2)
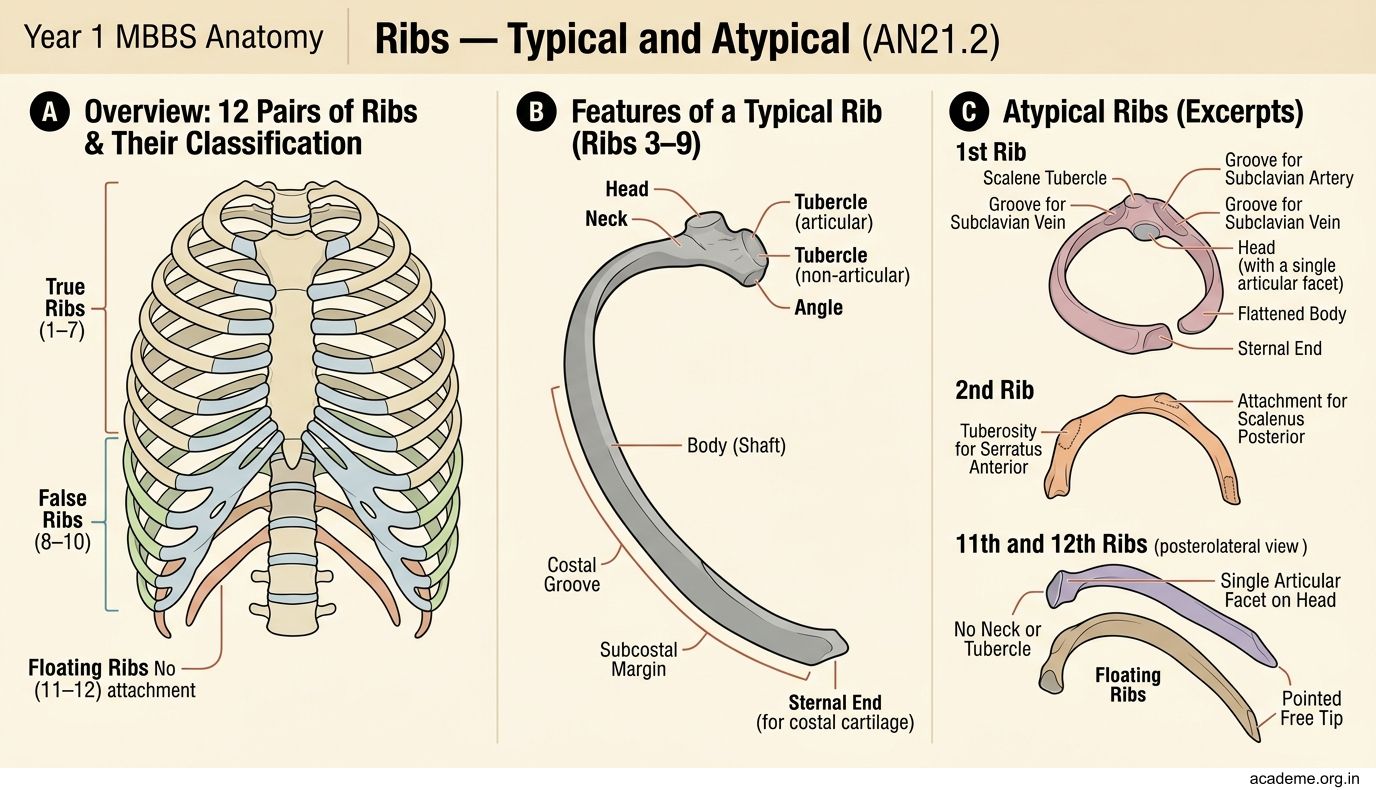
You have 12 pairs of ribs. They are classified by their anterior attachment:

Figure: Atypical ribs — what makes them special:

Figure: Ribs — Typical and Atypical (AN21.2)
- True ribs (1–7) — attach directly to the sternum via their own costal cartilage
- False ribs (8–10) — attach indirectly, their costal cartilages joining the cartilage of the rib above
- Floating ribs (11–12) — have no anterior attachment at all; their tips are free
The typical rib (ribs 3–9) has these features:
• A head with two articular facets (for two adjacent vertebral bodies) separated by a crest of the head
• A neck — the narrowed portion between the head and the tubercle
• A tubercle — a projection where the rib articulates with the transverse process of the corresponding vertebra
• A shaft (body) — curved, with a sharp bend called the angle where the rib turns forward
• A costal groove on the inferior inner surface — this groove shelters the intercostal vessels and nerve (VAN order — we'll learn this in Part 2)
Atypical ribs — what makes them special:
- 1st rib — the most atypical. It's short, broad, and flat (horizontally oriented, not vertically). It has a single facet on the head (only articulates with T1). Its upper surface has two grooves — for the subclavian vein (anterior) and subclavian artery (posterior) — separated by the scalene tubercle (attachment of scalenus anterior). A fracture of the 1st rib suggests severe trauma because it's well-protected; check for vascular injury.
- 2nd rib — has a rough area on its outer surface called the tuberosity for serratus anterior. Its head has two facets (like a typical rib).
- 10th rib — has a single facet on its head (only articulates with T10).
- 11th and 12th ribs — are short, have single facets, and have no neck, no tubercle, and no angle. They are the floating ribs with free anterior ends.
Thoracic Vertebrae — Designed for Rib Articulation (AN21.3)
There are 12 thoracic vertebrae (T1–T12), and they are unique because they articulate with ribs. A typical thoracic vertebra (T2–T8) has:

Figure: Thoracic Vertebrae — Designed for Rib Articulation (AN21.3)
- Costal facets on the body — a superior demifacet (half-facet) and an inferior demifacet on each side. A typical rib head spans two vertebral bodies, so the rib articulates with the inferior demifacet of the vertebra above and the superior demifacet of its own vertebra.
- Costal facet on the transverse process — for the tubercle of the corresponding rib
- Heart-shaped body — wider in the transverse axis
- Long, sloping spinous process — points downward like a roof tile (palpation: the spinous process of T7 is at the level of the inferior angle of the scapula)
- Circular vertebral foramen — smaller than cervical, larger than lumbar
Atypical thoracic vertebrae:
• T1 — has a complete superior costal facet (only for rib 1) and a demifacet inferiorly (for rib 2)
• T9 — may have only a superior demifacet (no inferior demifacet if rib 10 has a single facet)
• T10 — has a single complete costal facet on the body (for rib 10 only), no facet on transverse process
• T11 and T12 — each has a single complete costal facet, no facet on transverse process, short and stumpy spinous processes. T12 looks like a lumbar vertebra from below.
Memory pattern: The atypical vertebrae mirror the atypical ribs — wherever a rib has a single facet (1st, 10th, 11th, 12th), the corresponding vertebra is atypical too.
Thoracic Inlet and Outlet — Two Openings, Two Functions (AN21.4)
The thoracic cage has an opening at the top and one at the bottom:
Thoracic inlet (= superior thoracic aperture) — the gateway between the neck and the thorax. Shaped like a kidney bean, it's tilted forward (slopes downward from back to front).
Boundaries:
• Posterior: body of T1 vertebra
• Lateral: 1st rib and its costal cartilage on each side
• Anterior: superior border of the manubrium (jugular notch)
What passes through: trachea, oesophagus, major vessels (subclavian arteries, brachiocephalic veins), vagus and phrenic nerves, sympathetic trunks, thoracic duct (left side), lymphatic duct (right side). A cervical rib (an extra rib from C7) or a tight fibrous band can compress the subclavian artery and lower trunk of the brachial plexus here — causing thoracic outlet syndrome (despite the name, the compression is at the inlet).
Thoracic outlet (= inferior thoracic aperture) — the larger opening at the bottom, closed by the diaphragm.
Boundaries:
• Posterior: body of T12 vertebra
• Posterolateral: 11th and 12th ribs
• Anterolateral: costal margins (cartilages of ribs 7–10)
• Anterior: xiphoid process
The diaphragm seals this opening, with three major apertures: the aortic hiatus (T12), the oesophageal hiatus (T10), and the vena caval foramen (T8). Mnemonic for levels: "I 8 10 Eggs At 12" — IVC at T8, oEsophagus at T10, Aorta at T12.
SELF-CHECK
A clinician needs to count ribs on a patient's chest. The starting point is a palpable horizontal ridge on the sternum that marks the 2nd costal cartilage. What is this landmark called, and what vertebral level does it correspond to posteriorly?
A. Jugular notch; T2 vertebra
B. Sternal angle (Angle of Louis); T4/T5 intervertebral disc
C. Xiphoid process; T10 vertebra
D. Sternal angle (Angle of Louis); T2 vertebra
Reveal Answer
Answer: B. Sternal angle (Angle of Louis); T4/T5 intervertebral disc
The sternal angle (Angle of Louis) is the ridge at the manubriosternal joint. It marks the 2nd costal cartilage anteriorly and the T4/T5 intervertebral disc posteriorly. It's also where the trachea bifurcates and the aortic arch begins/ends. The jugular notch is higher (T2 level), and the xiphoid is lower (T9/T10 level).