Page 3 of 9
AN21.1-11 | Thoracic cage — SDL Guide (Part 3)
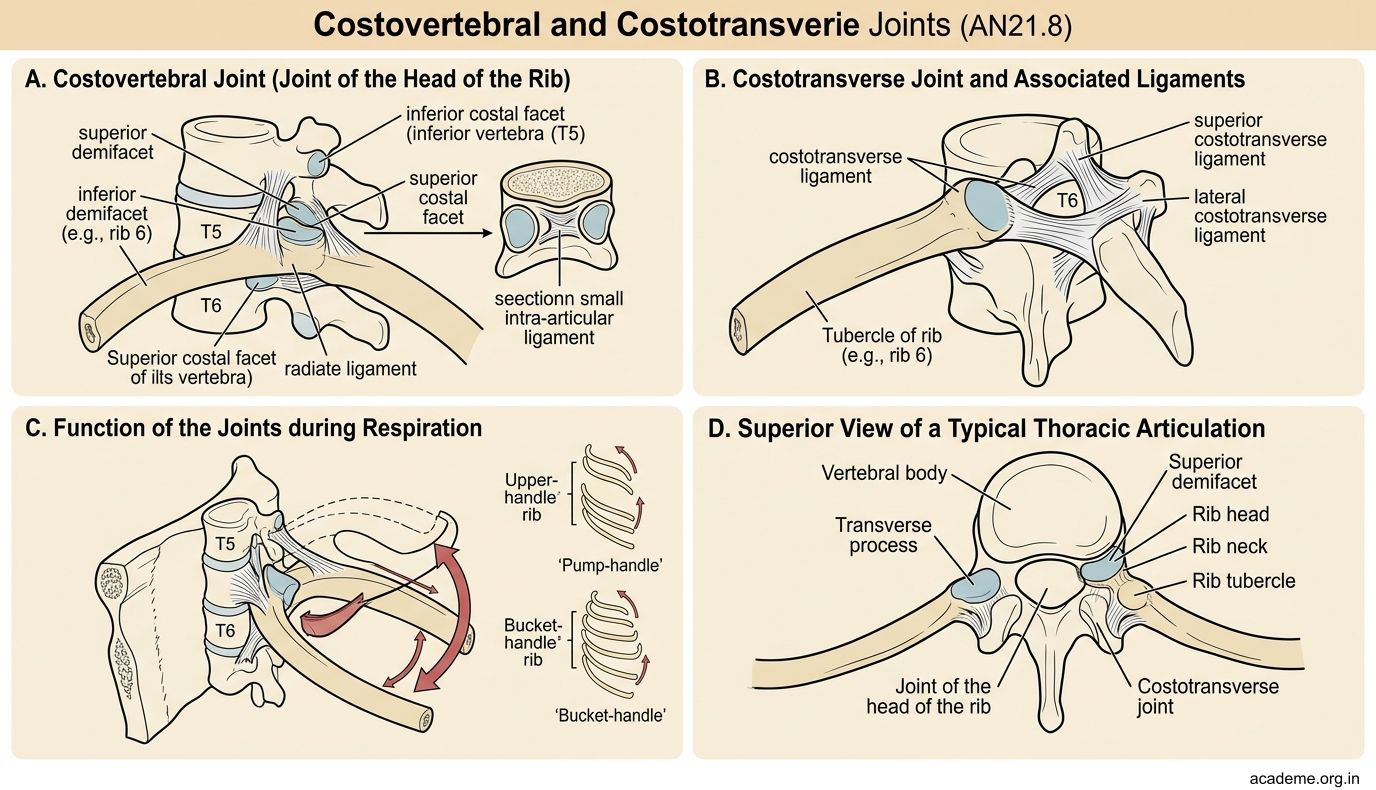
Costovertebral and Costotransverse Joints (AN21.8)
Each typical rib articulates with the vertebral column at two joints. These joints are crucial because they determine how the ribs move during breathing.

Figure: Costovertebral and Costotransverse Joints (AN21.8)
1. Joint of the head of the rib (costovertebral joint)
The head of a typical rib has two facets that articulate with:
• The superior demifacet of its own vertebra
• The inferior demifacet of the vertebra above
• The intervertebral disc between them
A small ligament — the intra-articular ligament — divides this joint into two compartments. It's a synovial joint, but its movement is limited to a small gliding motion.
2. Joint of the tubercle of the rib (costotransverse joint)
The articular facet on the rib's tubercle articulates with the costal facet on the transverse process of the corresponding vertebra. This is also a synovial joint.
The axis of rib movement depends on both joints working together. The rib rotates around an axis passing through these two joints — and the orientation of this axis determines whether the rib swings forward (pump-handle) or outward (bucket-handle). We'll see how in the next section.
Special cases:
• The 1st rib has a single facet (only articulates with T1)
• Ribs 11 and 12 have no costotransverse joint (no tubercle, so no articulation with the transverse process) — they're more mobile but also less stable
Mechanics of Respiration — Pump-Handle and Bucket-Handle (AN21.9)
Here's where the thoracic cage comes alive. Breathing is not just the lungs expanding — it's the entire cage changing shape. Two movements increase thoracic volume during inspiration:

Figure: Mechanics of Respiration — Pump-Handle and Bucket-Handle (AN21.9)
1. Pump-handle movement (increases anteroposterior diameter)
Imagine a pump handle — it goes up, and the far end moves forward. This is what the upper ribs (2–6) do. The axis of rotation passes almost transversely (side-to-side) through the costovertebral and costotransverse joints. When the rib elevates, its anterior end and the sternum move forward and upward, increasing the front-to-back dimension of the chest.
Try it: Place one hand on your sternum and breathe in deeply. You'll feel your sternum move forward — that's the pump-handle movement.
2. Bucket-handle movement (increases transverse diameter)
Imagine a bucket handle — it goes up, and the middle moves outward. This is what the lower ribs (7–10) do. The axis of rotation passes anteroposteriorly (front-to-back) through the joints. When the rib elevates, its middle portion (the most lateral point of the rib curve) moves outward, increasing the side-to-side dimension of the chest.
Try it: Place your hands on your lower ribs and breathe in. You'll feel them flare outward — that's the bucket-handle movement.
Both movements happen simultaneously with every breath. The upper ribs primarily pump-handle (more AP expansion), the lower ribs primarily bucket-handle (more transverse expansion), and the middle ribs do a bit of both.
The diaphragm adds the third dimension — it contracts and descends, increasing the vertical dimension of the thorax. Together, the three movements expand the thorax in all three dimensions, creating negative pressure that draws air into the lungs.
Spiral forward: In Respiratory Physiology (PY6), you'll learn how these mechanical changes translate into pressure changes (Boyle's law) and airflow. The anatomy you learn here is the structural basis for everything in respiratory physiology.
Costochondral and Interchondral Joints (AN21.10)
The anterior ends of the ribs don't reach the sternum directly. Instead, they connect via costal cartilages — bars of hyaline cartilage that provide flexibility to the thoracic cage.
Costochondral joints — where the bony rib meets its costal cartilage:
• Type: primary cartilaginous joint (synchondrosis)
• Movement: none (the bone and cartilage are directly continuous)
• No joint cavity, no synovial membrane — the periosteum of the rib blends with the perichondrium of the cartilage
• These joints can separate in trauma (costochondral separation) — painful but often missed on X-ray because cartilage is radiolucent
Sternocostal joints — where the costal cartilage meets the sternum:
• 1st sternocostal joint: primary cartilaginous (synchondrosis) — no movement, very firm
• 2nd–7th sternocostal joints: synovial — allow gliding movement during breathing
• The 2nd sternocostal joint is at the sternal angle — this is why the sternal angle is your rib-counting landmark
Interchondral joints — between adjacent costal cartilages of ribs 6-7, 7-8, 8-9 (and sometimes 9-10):
• Type: synovial — small, plane joints
• They link the costal cartilages together, contributing to the rigid costal margin
• They allow slight gliding during breathing
Clinical note — Tietze syndrome: Painful swelling of the costochondral or sternocostal joints (especially 2nd and 3rd), often mistaken for cardiac chest pain. It's benign but alarming. Palpation reproduces the pain — a key distinguishing feature from cardiac causes.
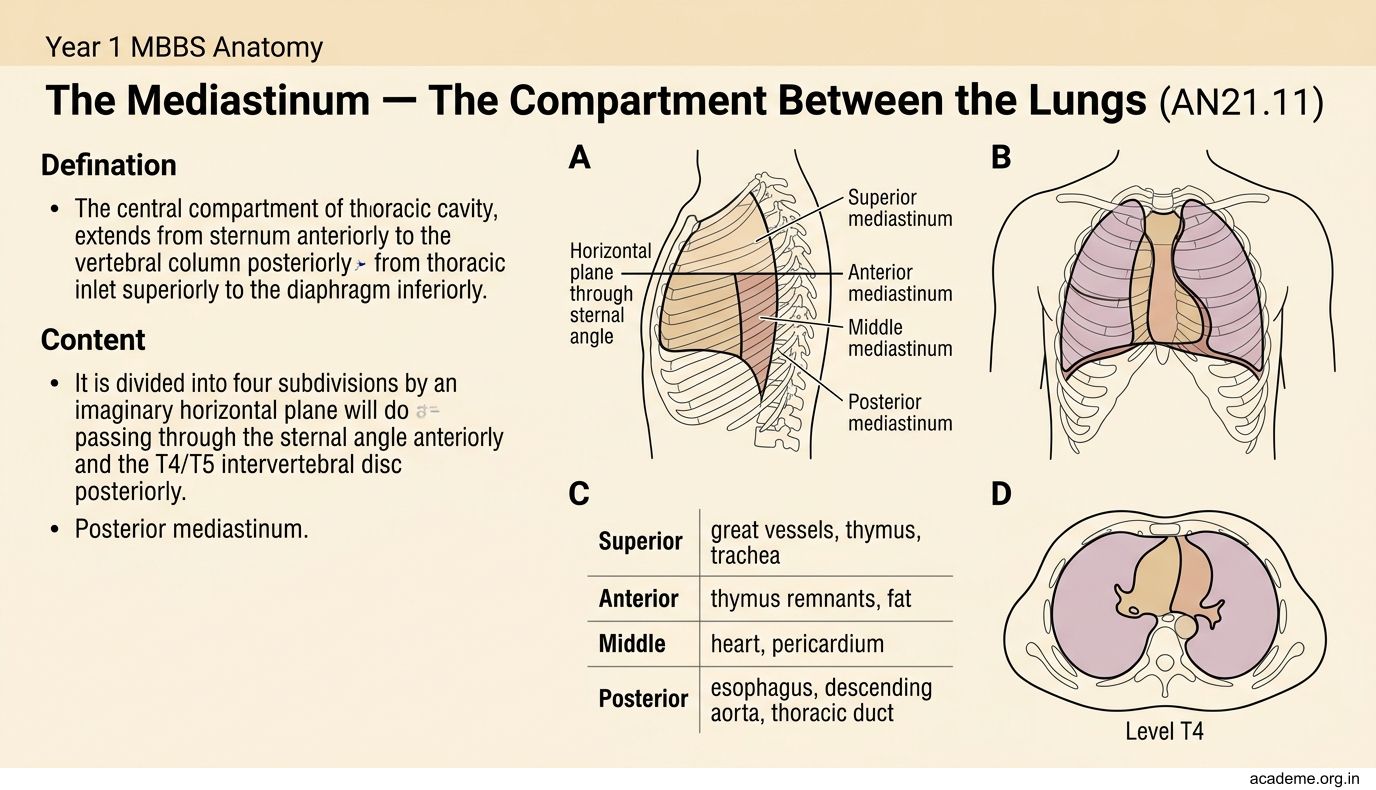
The Mediastinum — The Compartment Between the Lungs (AN21.11)
The mediastinum is the central compartment of the thoracic cavity — everything between the two lungs. It extends from the sternum (anteriorly) to the vertebral column (posteriorly), and from the thoracic inlet (superiorly) to the diaphragm (inferiorly).
It is divided into four subdivisions by an imaginary horizontal plane passing through the sternal angle anteriorly and the T4/T5 intervertebral disc posteriorly:
1. Superior mediastinum — above the plane
Contents: arch of aorta and its three branches (brachiocephalic trunk, left common carotid, left subclavian), SVC (and brachiocephalic veins), trachea and its bifurcation, oesophagus, thoracic duct, vagus nerves, phrenic nerves, left recurrent laryngeal nerve (loops under the aortic arch), and the thymus (prominent in children, involutes in adults).
2. Anterior mediastinum — below the plane, in front of the pericardium
Contents: fat, lymph nodes, remnants of the thymus, sternopericardial ligaments. This is a small space.
3. Middle mediastinum — contains the pericardium and its contents
Contents: the heart, pericardium, ascending aorta, pulmonary trunk, SVC (lower part), main bronchi, phrenic nerves (on the pericardium).
4. Posterior mediastinum — below the plane, behind the pericardium
Contents: descending thoracic aorta, oesophagus (lower part), azygos and hemiazygos veins, thoracic duct, vagus nerve (oesophageal plexus), sympathetic trunks and splanchnic nerves.
Mnemonic for the sternal angle as the dividing line: "All Thoracic Structures Meet at the Sternal Angle" — it divides superior from inferior mediastinum.
You'll revisit the mediastinum in detail when you study the heart (next module), the great vessels, and the respiratory system. For now, focus on the four subdivisions and the sternal angle as the landmark that divides them.
SELF-CHECK
During normal quiet inspiration, the transverse diameter of the lower thorax increases primarily due to which rib movement?
A. Pump-handle movement of upper ribs
B. Bucket-handle movement of lower ribs
C. Caliper movement of floating ribs
D. Descent of the xiphoid process
Reveal Answer
Answer: B. Bucket-handle movement of lower ribs
The bucket-handle movement of the lower ribs (7–10) increases the transverse diameter. The rib elevates and its middle swings outward — like lifting a bucket handle. In contrast, the pump-handle movement of the upper ribs increases the anteroposterior diameter (sternum moves forward). Both happen simultaneously during breathing.