Page 1 of 8
AN22.1-7 | Heart & Pericardium — SDL Guide
Learning Objectives
- Describe the pericardium — its layers, sinuses, and clinical significance including pericardial effusion and cardiac tamponade (AN22.1)
- Describe the external and internal features of all four chambers of the heart, including the interatrial and interventricular septa (AN22.2)
- Trace the origin, course, and distribution of the coronary arteries (LAD, LCx, RCA) and identify the territories they supply (AN22.3)
- Explain the anatomical basis of ischaemic heart disease (IHD) — how coronary artery blockage leads to myocardial infarction (AN22.4)
- Describe the coronary sinus and the venous drainage of the heart (AN22.5)
- Describe the fibrous skeleton of the heart and its functions (AN22.6)
- Describe the conducting system of the heart — SA node, AV node, Bundle of His, and Purkinje fibres (AN22.7)
INSTRUCTIONS
This module covers the heart and pericardium — the engine of your circulatory system. We'll start from what you can feel on your own body (your heartbeat, your pulse) and build from the outside in: pericardium wrapping → chambers inside → coronary arteries feeding → conducting system coordinating.
Parallel connections: In Physiology (PY5), you're studying the cardiac cycle — systole, diastole, heart sounds, and blood pressure. The anatomy you learn here is the structural foundation for everything you'll learn about cardiac function. In Biochemistry (BI4), you're studying lipid metabolism — understanding how cholesterol deposits in coronary arteries (atherosclerosis) leads directly to the ischaemic heart disease we discuss in AN22.4.
References
- OpenStax Anatomy and Physiology 2e, Chapter 19: The Cardiovascular System — The Heart (textbook (CC BY 4.0))
- B.D. Chaurasia's Human Anatomy, Vol. 1, Ch 18-19: The Heart (textbook)
- Netter's Atlas of Human Anatomy, 8th ed., Plates 212–226 (Heart) (atlas)
- Gray's Anatomy for Students, 4th ed., Chapter 3: Thorax — Heart (textbook)
Version 2.0 | NMC CBUC 2024, Adapted from OpenStax A&P 2e (CC BY 4.0)
CLINICAL SCENARIO
Put your hand on your chest — slightly to the left of centre, between the 2nd and 5th ribs. Feel that? Your heart beats about 100,000 times a day, 36 million times a year, and roughly 2.5 billion times in a lifetime. It starts beating around day 22 of embryonic development and never stops until you die. No other muscle in your body works this hard — and it does it without you ever consciously commanding it. How? The answer lies in the anatomy we're about to explore: a self-contained organ with its own wrapping, its own blood supply, and its own pacemaker.
WHY THIS MATTERS
Heart disease is the number one cause of death worldwide — and India is in the middle of a cardiovascular epidemic. As a doctor, you will encounter heart disease every single day of your practice, regardless of your speciality. Whether you're an emergency physician diagnosing a myocardial infarction, an obstetrician managing a pregnant woman with valvular disease, or a general practitioner counselling patients about risk factors — you need to understand the heart's anatomy cold. This module gives you the structural foundation that everything else builds upon.
RECALL
From your study of the thoracic wall, you know that the thorax contains the two pleural cavities (housing the lungs) and the mediastinum (the central compartment). The heart sits in the middle mediastinum, enclosed in its own sac called the pericardium. You also know the concept of serous membranes from the pleura — a double-layered membrane with a thin film of fluid between the layers. The pericardium follows exactly the same principle.
The Pericardium — A Double-Walled Protective Bag (AN22.1)
The heart doesn't just float freely in the chest — it sits inside a tough, multi-layered sac called the pericardium. Think of pushing your fist into a balloon: your fist is the heart, and the balloon wrapping around it has two layers — one touching your fist (visceral layer) and one on the outside (parietal layer). The space between them contains a small amount of lubricating fluid.

Figure: The Pericardium — A Double-Walled Protective Bag (AN22.1)
The pericardium has two main layers:
- Fibrous pericardium — the tough outer bag. Made of dense connective tissue. It anchors the heart to the diaphragm below, the sternum in front, and the great vessels above. It cannot stretch — and this is critically important in disease (we'll see why shortly).
- Serous pericardium — the slippery inner lining, which itself has two layers:
- Parietal layer — lines the inside of the fibrous pericardium
- Visceral layer (also called the epicardium) — covers the heart surface directly
- Between them lies the pericardial cavity — normally containing 15–50 mL of serous fluid that allows the heart to beat with minimal friction
The pericardial sinuses — two recesses within the pericardial cavity that surgeons must know:
- Transverse sinus — a passage behind the aorta and pulmonary trunk, in front of the superior vena cava. A surgeon can pass a finger through this sinus to place a clamp on the aorta and pulmonary trunk during cardiac bypass surgery. Think of it as a tunnel behind the outflow pipes.
- Oblique sinus — a cul-de-sac behind the left atrium, bounded by the reflections of the serous pericardium around the pulmonary veins and IVC. You can slide your hand in from below but you cannot pass a finger all the way through — it's a dead-end, not a tunnel.
Clinical connection — cardiac tamponade:
If fluid rapidly accumulates in the pericardial cavity (from bleeding after a stab wound, or from pericarditis), the inelastic fibrous pericardium cannot expand. The fluid compresses the heart, preventing it from filling during diastole. This is cardiac tamponade — a life-threatening emergency. Beck's triad identifies it: (1) low blood pressure, (2) distended neck veins, (3) muffled heart sounds. Emergency treatment is pericardiocentesis — inserting a needle below the xiphoid process to drain the fluid.
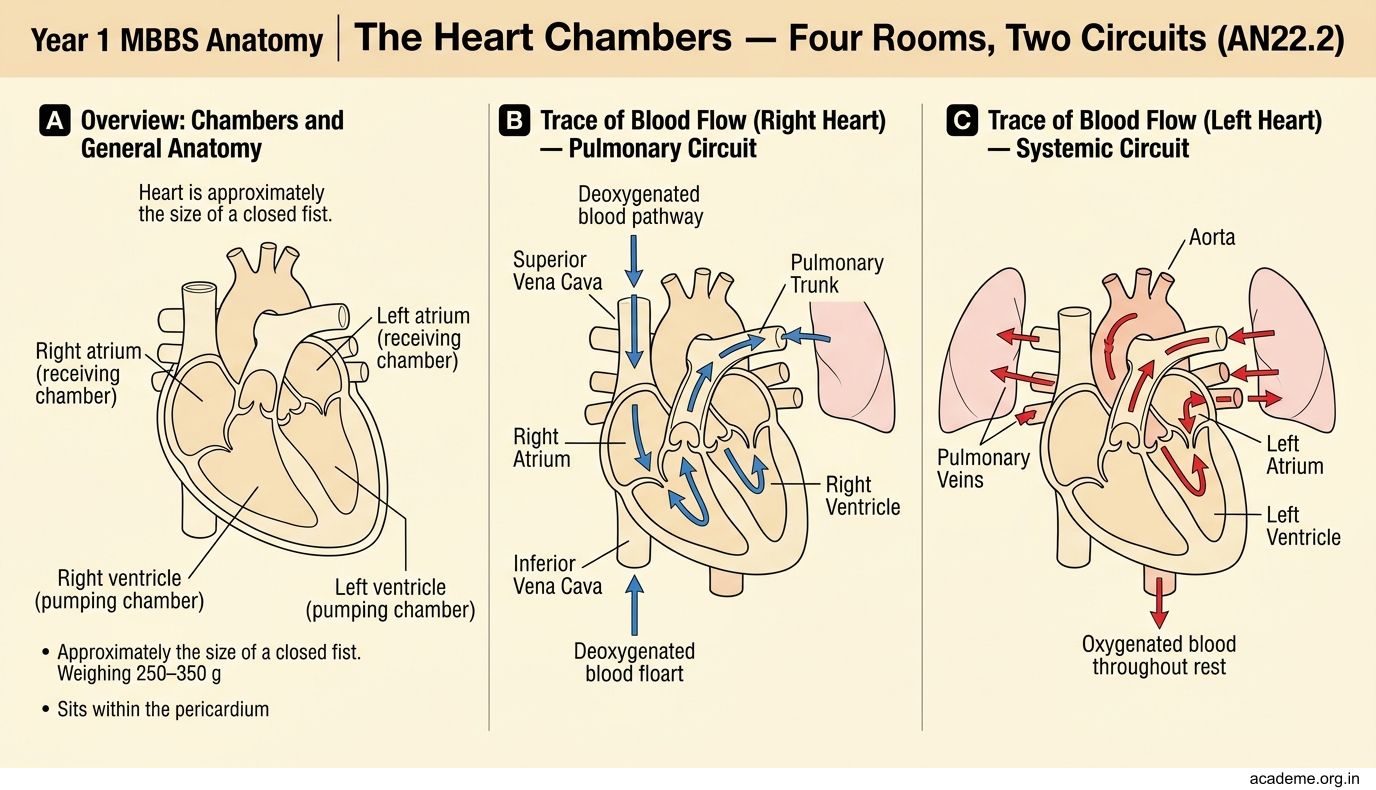
The Heart Chambers — Four Rooms, Two Circuits (AN22.2)
Open the pericardium and you see the heart — a muscular pump about the size of your closed fist, weighing 250–350 g. It has four chambers: two atria (receiving rooms) on top and two ventricles (pumping rooms) below.

Figure: The Heart Chambers — Four Rooms, Two Circuits (AN22.2)
Let's trace the blood flow — starting from the body, through the heart, to the lungs, and back:
1. Right atrium — receives deoxygenated blood from:
- Superior vena cava (SVC) — from the head, neck, and upper limbs
- Inferior vena cava (IVC) — from the trunk and lower limbs
- Coronary sinus — from the heart wall itself
- Internal features: crista terminalis (a smooth muscular ridge), musculi pectinati (comb-like muscle ridges in the anterior wall), fossa ovalis (a shallow depression marking the site of the foramen ovale — the opening that allowed blood to bypass the lungs before birth)
2. Right ventricle — pumps blood to the lungs through the pulmonary trunk
- Internal features: trabeculae carneae (irregular muscular ridges), septomarginal trabecula (also called the moderator band — carries the right bundle branch of the conducting system to the anterior papillary muscle), three papillary muscles attached to the tricuspid valve by chordae tendineae ('heart strings')
- The infundibulum (conus arteriosus) — the smooth outflow tract leading to the pulmonary valve
3. Left atrium — receives oxygenated blood from the lungs via four pulmonary veins (two from each lung)
- Mostly smooth-walled (the musculi pectinati are confined to the left auricle — the small ear-shaped appendage)
4. Left ventricle — the powerhouse. Pumps oxygenated blood to the entire body through the aorta
- Wall is 3× thicker than the right ventricle (it pumps against systemic resistance, not just pulmonary)
- Internal features: thicker trabeculae carneae, two papillary muscles (anterior and posterior) attached to the mitral (bicuspid) valve
- The aortic vestibule — smooth outflow tract leading to the aortic valve
The septa:
• Interatrial septum — thin wall between the atria. Contains the fossa ovalis (remnant of foramen ovale). An atrial septal defect (ASD) is a hole that persists after birth — blood shunts from left atrium to right (left-to-right shunt because left-side pressures are higher).
• Interventricular septum — thick, muscular wall between the ventricles. Has a thin membranous part (superior) and a thick muscular part (inferior). Ventricular septal defects (VSDs) are the most common congenital heart defect — usually in the membranous part.
The Fibrous Skeleton — The Heart's Internal Scaffold (AN22.6)
Between the atria and ventricles lies a dense connective tissue framework called the fibrous skeleton of the heart. It's made of four fibrous rings (annuli fibrosi) around the four valves, fused together into a single structural unit.
The fibrous skeleton has three critical functions:
- Structural support — it forms the 'frame' to which the valve leaflets and heart muscle attach. Without it, the valves would have nothing to anchor to.
- Electrical insulation — it separates the atrial muscle mass from the ventricular muscle mass. Electrical impulses cannot cross the fibrous skeleton directly. The only pathway from atria to ventricles is through the AV node and Bundle of His — this ensures the atria contract before the ventricles (we'll explore this in Part 2).
- Attachment for myocardium — the atrial muscle fibres insert onto the top of the skeleton, and the ventricular muscle fibres originate from the bottom. This allows the two muscle masses to contract independently.
Spiral forward: In Physiology (PY5), you'll learn about the cardiac cycle — the precise timing of atrial and ventricular contraction. The fibrous skeleton is what makes this timing possible by electrically isolating the two chambers.
SELF-CHECK
A patient with a stab wound to the chest develops low blood pressure, distended neck veins, and muffled heart sounds (Beck's triad). What is the diagnosis, and why can't the pericardium simply stretch to accommodate the blood?
A. Pneumothorax; the pericardium is elastic but the lung collapses
B. Cardiac tamponade; the fibrous pericardium is inelastic and cannot expand
C. Cardiac tamponade; the serous pericardium actively contracts
D. Haemothorax; the pericardial cavity communicates with the pleural cavity
Reveal Answer
Answer: B. Cardiac tamponade; the fibrous pericardium is inelastic and cannot expand
This is cardiac tamponade — blood accumulates in the pericardial cavity faster than it can be absorbed. The fibrous pericardium is made of tough, inelastic connective tissue that cannot stretch. The trapped blood compresses the heart, preventing diastolic filling. Emergency treatment: pericardiocentesis (needle drainage via the subxiphoid approach).