Page 1 of 7
AN25.1-9 | Thorax — SDL Guide
Learning Objectives
- Describe the thoracic vertebrae and their features (AN25.1)
- Classify and describe the ribs with their articulations (AN25.2)
- Describe the intercostal space — contents and their arrangement (AN25.3)
- Describe the diaphragm — attachments, openings, and nerve supply (AN25.4)
- Define and describe the thoracic inlet and outlet (AN25.5)
- Identify and interpret thoracic cage structures on X-ray and CT (AN25.6)
- Describe common thoracic cage anomalies (AN25.7)
- Describe surface markings of thoracic viscera (AN25.8)
- Apply thoracic anatomy to common clinical scenarios (AN25.9)
INSTRUCTIONS
Work through systematically. Use reference CXRs alongside the imaging section. Complete micro-quizzes before proceeding.
References
- Gray's Anatomy for Students — Chapter 3: Thorax (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 1 — Thorax (Textbook)
- OpenStax Anatomy and Physiology 2e — The Thoracic Cage (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 22-year-old motorcyclist is brought to a trauma centre in Puducherry after a collision. He is breathless with paradoxical chest wall movement — the left side moves inward on inspiration. CXR shows multiple rib fractures (ribs 4–8) on the left, with a fluid level.
What is the diagnosis? What does "paradoxical movement" mean anatomically? Why are multiple adjacent fractures dangerous?
This is a flail chest — and your thoracic anatomy knowledge is what makes you the doctor who understands it.
WHY THIS MATTERS
The thoracic cage is the most commonly injured structure in road traffic accidents — India's leading cause of trauma. Understanding thoracic anatomy directly saves lives in casualty:
- Rib fractures — diagnosis, complications (pneumothorax, haemothorax, flail chest)
- Intercostal nerve blocks — pain management for rib fractures
- Diaphragmatic hernia — both congenital (neonatal emergency) and traumatic
- Thoracic outlet syndrome — compression of subclavian vessels + brachial plexus by cervical rib or tight scalenes
- Surface markings — essential for clinical examination (auscultation, percussion, cardiac impulse)
Cross-reference PY: The mechanics of breathing (Boyle's law, chest wall compliance) depend entirely on the anatomy of the thoracic cage and diaphragm.
RECALL
Before we begin, recall:
- The thoracic cage has 12 vertebrae, 12 pairs of ribs, and the sternum
- The sternum has 3 parts: manubrium, body, xiphoid process
- The sternal angle (manubriosternal joint) is at T4/T5 — a critical landmark
- Ribs articulate posteriorly with vertebrae and anteriorly with costal cartilages → sternum (true ribs) or remain free (floating ribs)
Thoracic Vertebrae and Ribs (AN25.1, AN25.2)
Thoracic Vertebrae (T1–T12) — Distinguishing Features:
Thoracic vertebrae are identified by their costal facets for rib articulation:
- Costal demifacets on the vertebral body (superior and inferior) — for the head of the rib
- Costal facet on the transverse process — for the tubercle of the rib (T1–T10)
- Heart-shaped vertebral body (intermediate between cervical and lumbar)
- Long, oblique spinous processes (point downward — overlap the vertebra below)
T1 has a full superior facet + demifacet below; T10–T12 have full (not demi) facets. T12 has no transverse facet (12th rib has no tubercle articulation).
Classification of Ribs:
| Type | Ribs | Characteristics |
|---|---|---|
| True (vertebrosternal) | 1–7 | Costal cartilage connects directly to sternum |
| False (vertebrochondral) | 8–10 | Costal cartilage joins that of the rib above |
| Floating (vertebral) | 11–12 | Free anterior end — no anterior attachment |
Parts of a typical rib (3–9): Head → Neck → Tubercle → Angle → Body (shaft)
- Head: 2 articular facets separated by a crest (upper facet with rib above's vertebra, lower facet with own vertebra)
- Tubercle: articular part (for transverse process) + non-articular (for ligament attachment)
- Angle: where rib bends forward — most vulnerable to fracture
- Costal groove: inferior border of shaft — contains intercostal vein, artery, nerve (VAN — superior to inferior)
Atypical ribs:
- Rib 1: flat, horizontal, broad; two grooves (subclavian artery, vein) separated by scalene tubercle; no costal angle or groove — scalene muscles attach
- Rib 2: transition between 1 and typical
- Ribs 11–12: no neck, tubercle, or costal groove; one articular facet
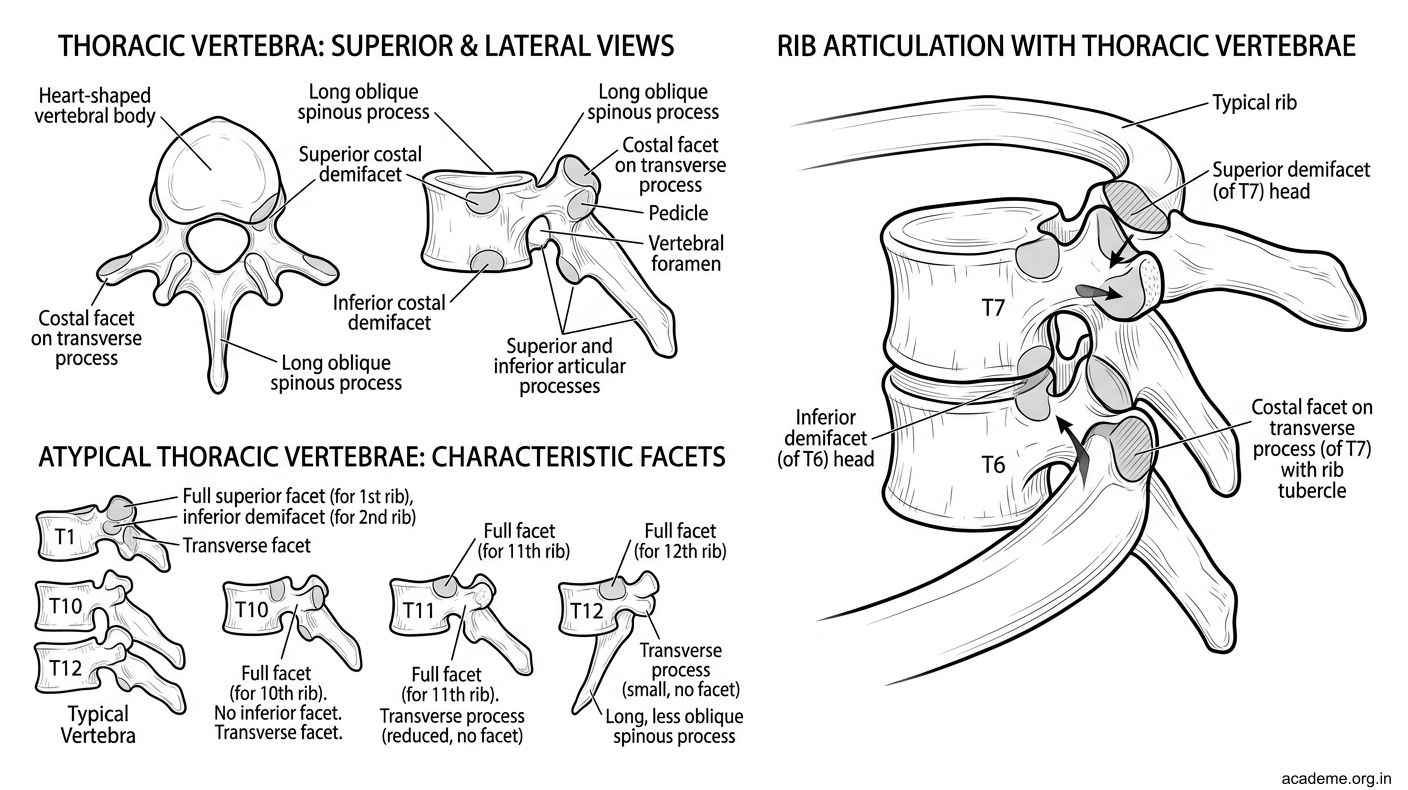
Figure: Thoracic Vertebrae and Ribs (AN25.1, AN25.2)
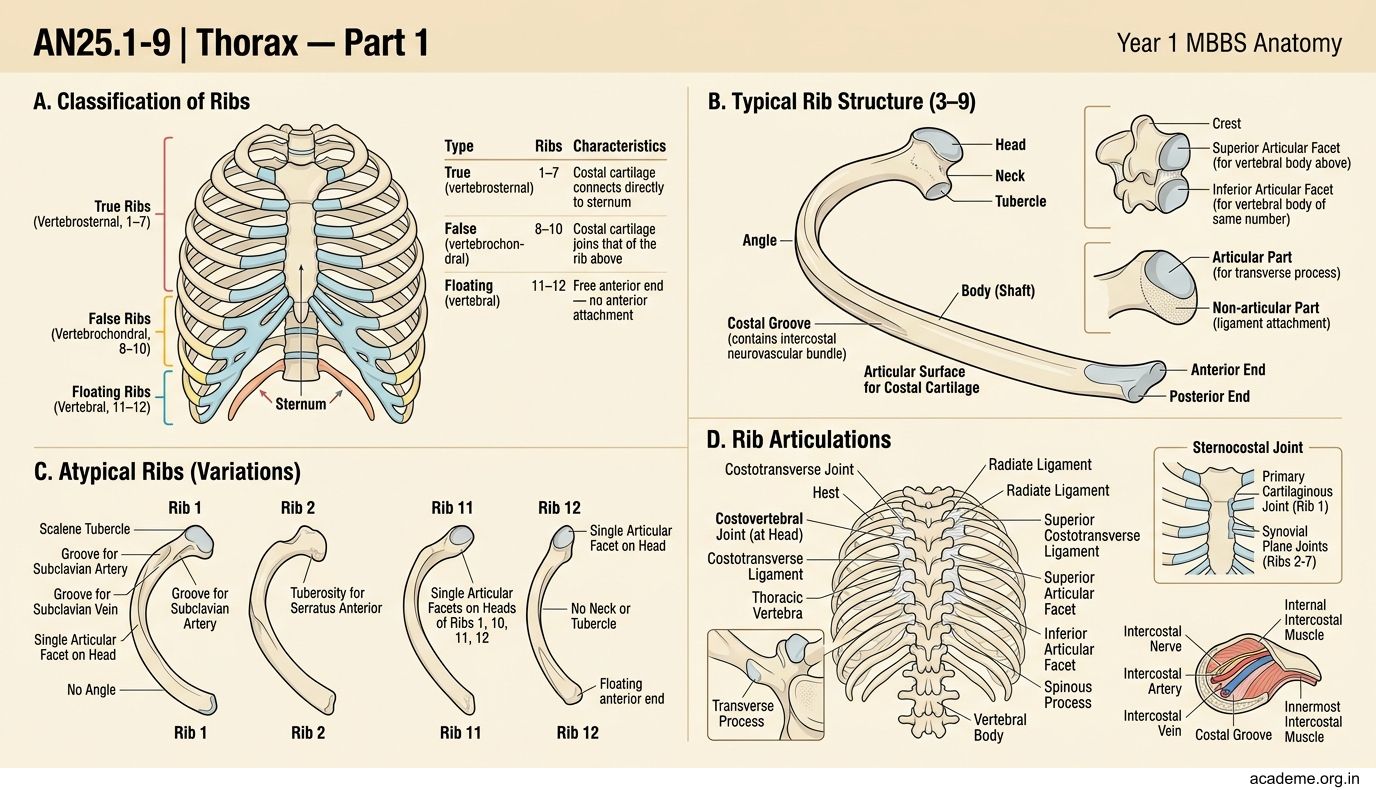
Figure: Classification of Ribs:
Intercostal Space (AN25.3)
Each intercostal space (ICS) lies between two adjacent ribs and contains the intercostal muscles, vessels, and nerve.
Three layers of intercostal muscles (external → internal):
- External intercostal — fibres run forward and downward; active in inspiration; replaced anteriorly (near costal cartilages) by the anterior intercostal membrane
- Internal intercostal — fibres run backward and downward (perpendicular to external); active in forced expiration; replaced posteriorly (near vertebral column) by the posterior intercostal membrane
- Innermost intercostal — deepest; separate from internal intercostal by the intercostal neurovascular bundle
Intercostal Neurovascular Bundle — lies between the internal and innermost intercostal muscles, in the costal groove (under the rib above):
Order (superior to inferior): Vein → Artery → Nerve (mnemonic: VAN)
Anterior intercostal arteries — from the internal thoracic (mammary) artery (spaces 1–6) and musculophrenic artery (spaces 7–9)
Posterior intercostal arteries — spaces 1–2 from superior intercostal artery (branch of costocervical trunk); spaces 3–11 from descending thoracic aorta
Clinical: Needle/drain insertion should be over the upper border of the lower rib to avoid the neurovascular bundle which runs under the rib above. Exception: ribs 1 and 2 have vessels near the upper border — be cautious.
Intercostal nerve block: Inject local anaesthetic below the rib (costal groove) for post-rib fracture pain relief.
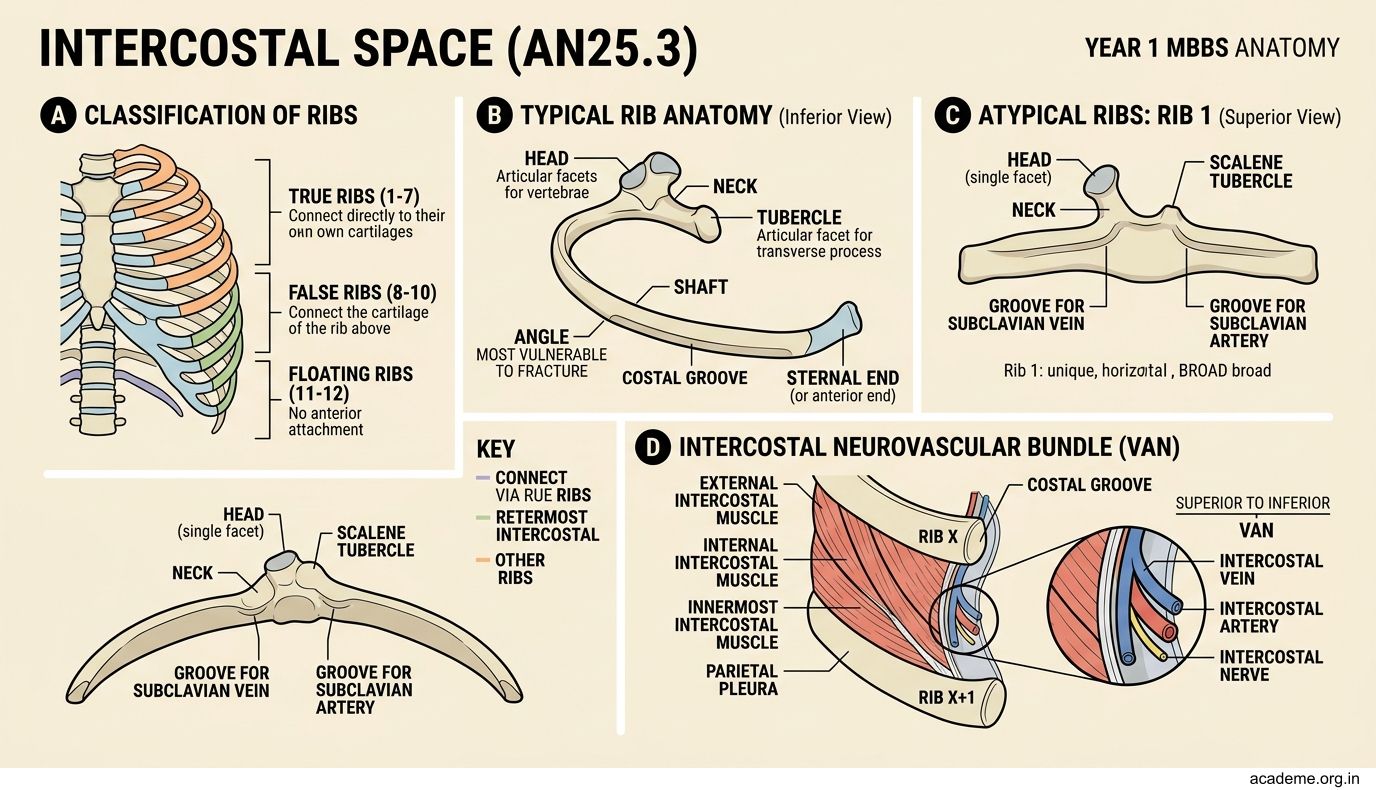
Figure: Intercostal Space (AN25.3)
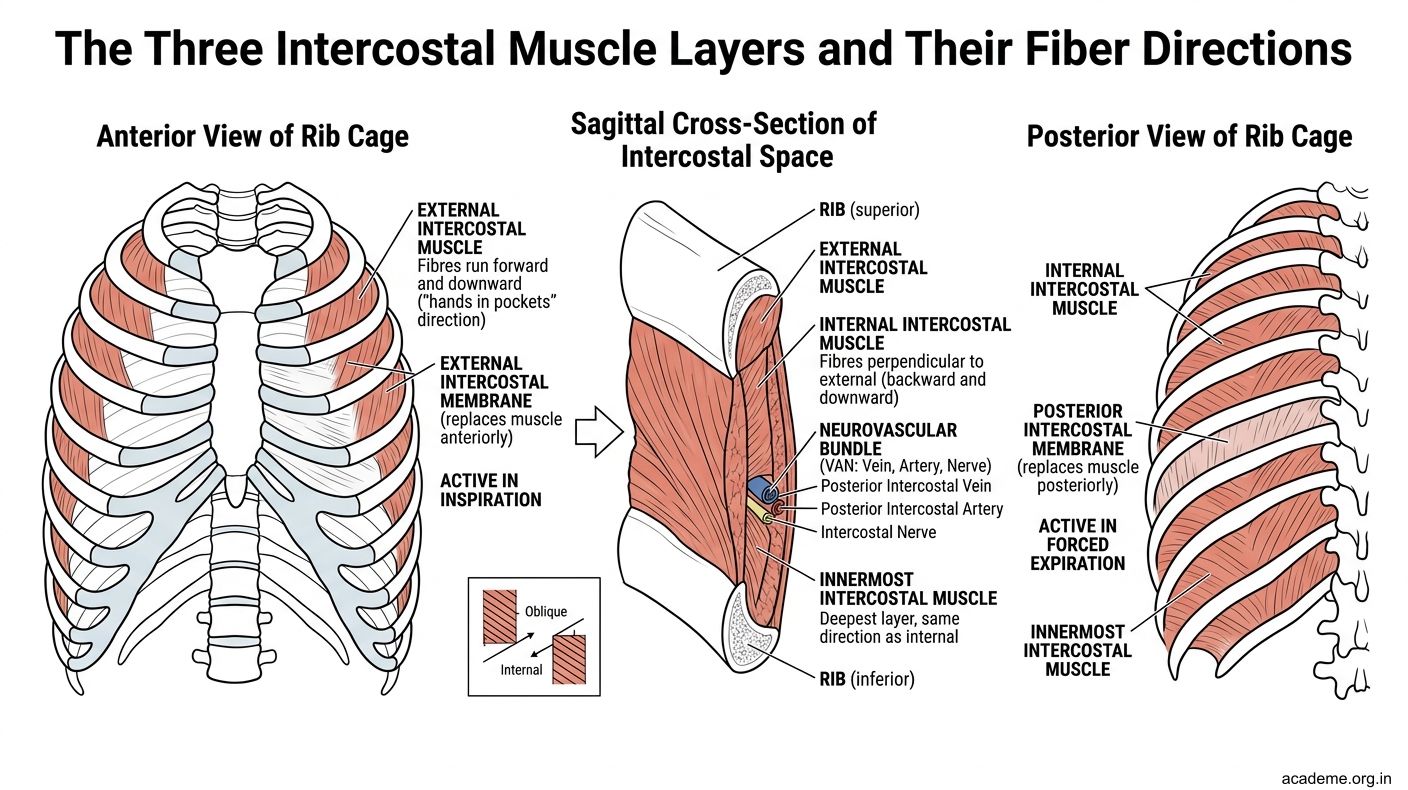
Figure: Three layers of intercostal muscles (external → internal):
SELF-CHECK
A. Over the upper border of the rib above
B. Through the middle of the intercostal space
C. Over the upper border of the rib below (lower rib)
D. At the costal angle posteriorly
Reveal Answer
Answer: see explanation below
The intercostal neurovascular bundle (VAN) runs in the costal groove under the rib above. Inserting over the upper border of the lower rib avoids this bundle.
Diaphragm (AN25.4)
The diaphragm is the primary muscle of inspiration — it is a dome-shaped musculotendinous partition separating the thorax from the abdomen.
Attachments:
- Sternal part: posterior surface of xiphoid process (2 muscular slips)
- Costal part: inner surfaces of lower 6 ribs and their costal cartilages (7–12)
- Vertebral (crural) part: right crus (from L1–L3 vertebral bodies + discs), left crus (L1–L2); also from the arcuate ligaments
Central tendon: trefoil-shaped aponeurosis; the heart rests on it (pericardium fuses with it)
Openings (and structures passing through):
| Opening | Level | Structures |
|---|---|---|
| Caval opening | T8 | IVC, right phrenic nerve |
| Oesophageal hiatus | T10 | Oesophagus, anterior + posterior vagal trunks, oesophageal branches of left gastric vessels |
| Aortic hiatus | T12 | Aorta, thoracic duct, azygos vein |
Mnemonic for levels: "I 8 10 eggs at 12" (IVC=T8, Oesophagus=T10, Aorta=T12)
Nerve supply:
- Motor: phrenic nerve (C3, C4, C5) — sole motor supply to the entire diaphragm
- Sensory: central diaphragm (central tendon + adjacent muscle) → phrenic nerve; peripheral diaphragm → lower intercostal nerves (T6–T12)
- Referred pain from diaphragm: tip of shoulder (C4 dermatome) — why subphrenic abscess presents with shoulder tip pain
Mechanism of inspiration: Diaphragm contracts → dome descends → thoracic volume increases → negative intrapleural pressure draws in air. Cross-ref PY: Boyle's law, compliance, surfactant, work of breathing.
Clinical:
- Diaphragmatic hernia (left > right): congenital Bochdalek hernia (posterolateral defect, left) → intestinal loops in thorax → neonatal respiratory distress
- Hiatus hernia: stomach herniates through oesophageal hiatus → GORD
- Phrenic nerve palsy: paradoxical diaphragmatic movement on fluoroscopy
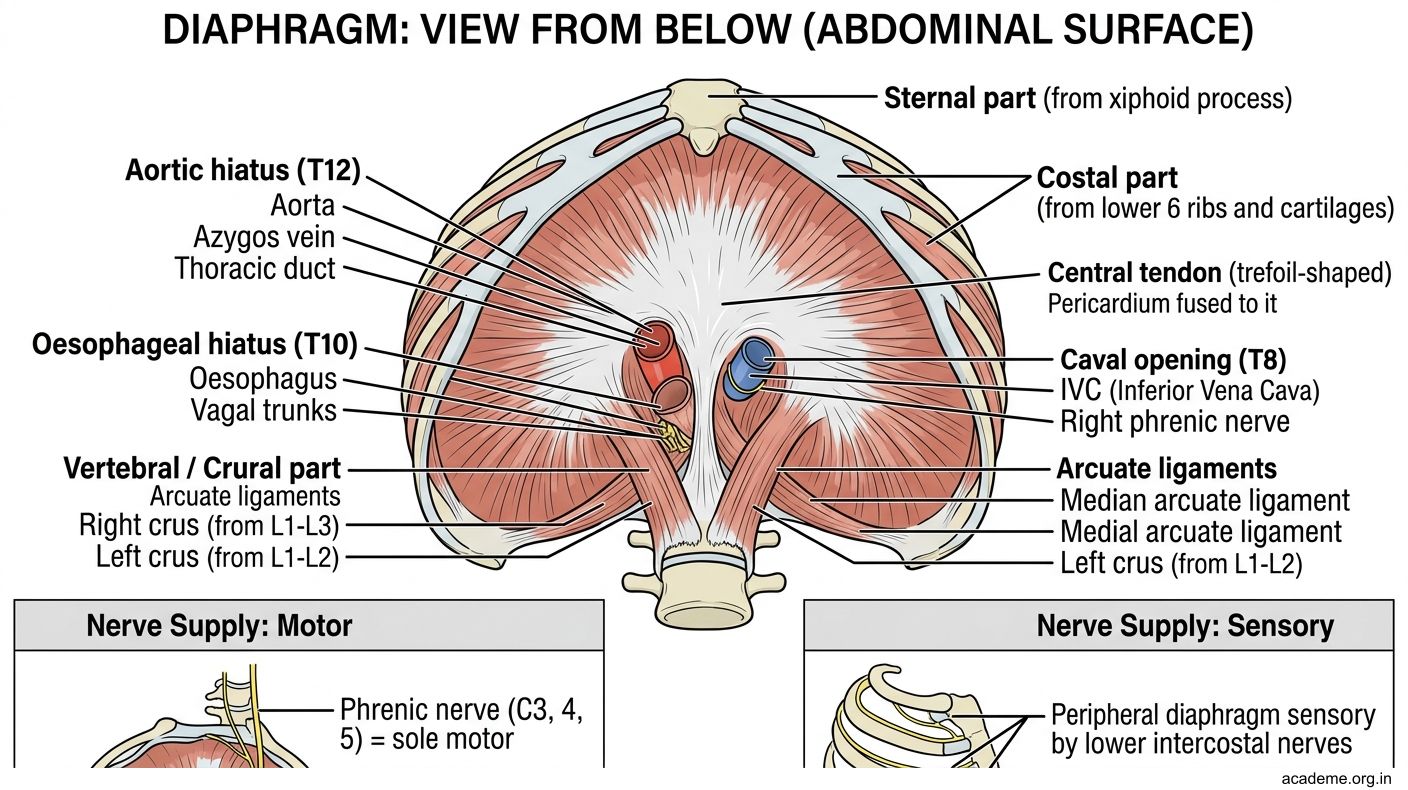
Figure: Diaphragm (AN25.4)
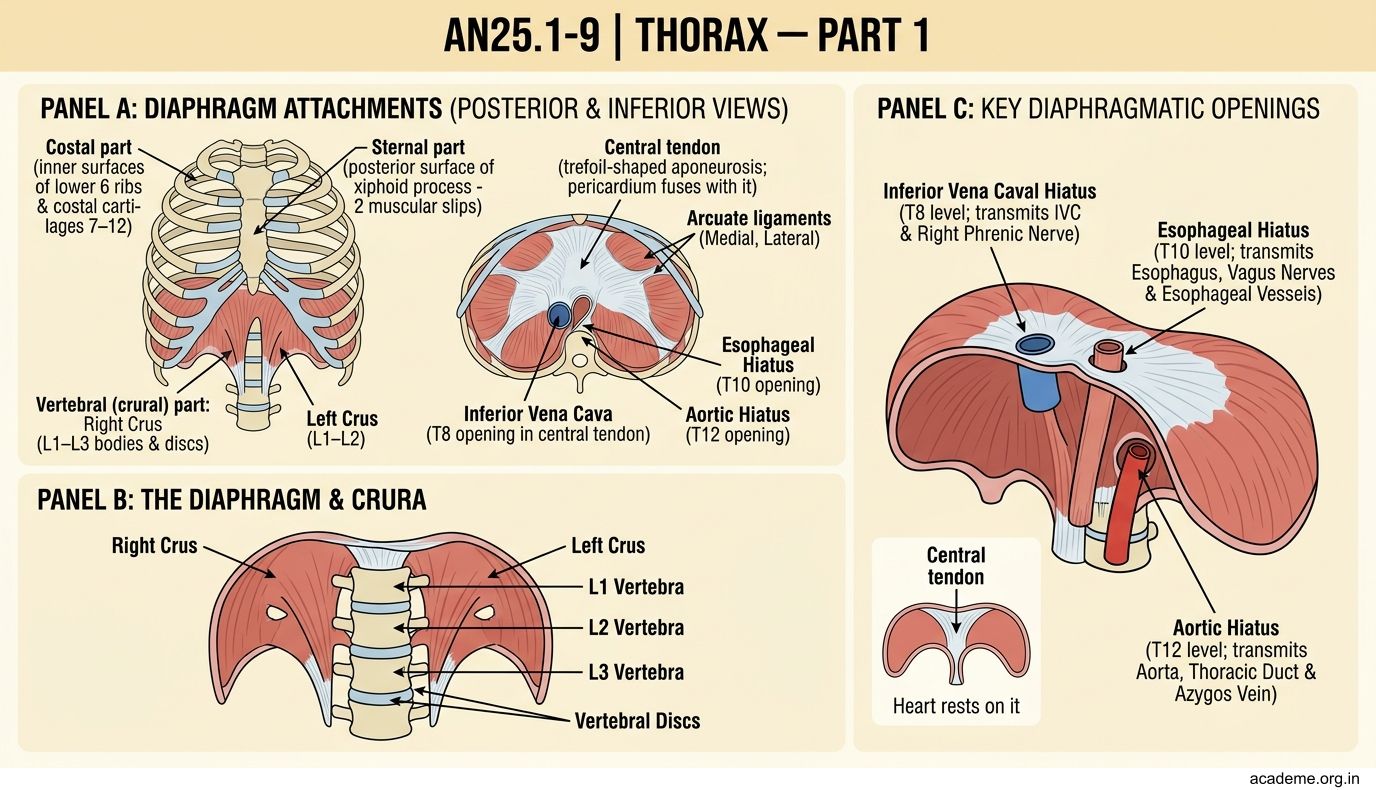
Figure: Openings (and structures passing through):