Page 1 of 7
AN31.1-5 | Orbit — SDL Guide
Learning Objectives
- Describe and identify the extraocular muscles — their attachments, nerve supply, and actions (AN31.1)
- Describe the nerves and vessels within the orbit — origin, course, and branches (AN31.2)
- Explain the anatomical basis of Horner's syndrome — the sympathetic pathway and clinical signs (AN31.3)
- Describe the components of the lacrimal apparatus and the pathway of tear drainage (AN31.4)
- Explain the anatomical basis of oculomotor, trochlear, and abducent nerve palsies and strabismus (AN31.5)
INSTRUCTIONS
Work through the blocks in order. Complete the micro-quiz after the main content before checking answers. Use your atlas (Gray's or BD Chaurasia) to visualise the orbit as you read.
References
- Gray's Anatomy for Students (Drake et al.) — Head and Neck: Orbit (Textbook)
- BD Chaurasia's Human Anatomy Vol. 3 — Head, Neck & Brain (Textbook)
- Snell's Clinical Neuroanatomy — Cranial Nerves III, IV, VI (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 58-year-old woman from Vellore presents to a government hospital with a drooping of her right eyelid that she noticed three days ago. On closer examination, her right pupil is constricted, not dilated, and the eye appears to be slightly sunken. She also mentions her face feels dry on the right side.
Which part of the nervous system has been affected? Which anatomical pathway has been interrupted? What is the likely diagnosis?
By the end of this module, you will be able to answer these questions — and diagnose Horner's syndrome — with anatomical precision.
WHY THIS MATTERS
The orbit is a densely packed anatomical space housing the eyeball and all its motor, sensory, and autonomic connections. In Indian clinical practice, you will encounter:
- Oculomotor (CN III) palsy — a classic sign of posterior communicating artery aneurysm; the dilated pupil is the warning sign
- Horner's syndrome — seen in Pancoast tumours (common in bidi/cigarette smokers), cervical sympathetic chain injury, or carotid dissection
- Strabismus (squint) — one of the most common paediatric ophthalmic conditions in India; understanding muscle actions is essential for surgical planning
- Epiphora (watering eyes) — blocked nasolacrimal duct; commonly seen in infants and post-traumatic facial injuries
- Retrobulbar haematoma — a surgical emergency after orbital wall fractures (road traffic accidents, assault)
Orbital anatomy is directly examined in USMLE, PG entrance exams (NEET-PG, AIIMS), and is foundational to both ophthalmology and neurology postings.
RECALL
Before we begin, recall what you have already covered:
- The orbit is a bony pyramid with its apex pointing posteriorly toward the optic canal
- The optic canal transmits the optic nerve (CN II) and ophthalmic artery
- The superior orbital fissure transmits CN III, IV, V1 (ophthalmic), VI, and superior ophthalmic vein
- The inferior orbital fissure transmits the maxillary nerve (V2) and infraorbital vessels
- The tendinous ring (annulus of Zinn) is the common origin for four recti muscles
Extraocular Muscles — Attachments, Nerve Supply, and Actions (AN31.1)
There are seven extraocular muscles controlling eye movement (six move the eyeball; one elevates the eyelid).
The Six Muscles that Move the Eyeball
| Muscle | Origin | Insertion | Nerve | Primary Action |
|---|---|---|---|---|
| Superior rectus | Annulus of Zinn (upper part) | Superior sclera | CN III (superior division) | Elevation |
| Inferior rectus | Annulus of Zinn (lower part) | Inferior sclera | CN III (inferior division) | Depression |
| Medial rectus | Annulus of Zinn (medial part) | Medial sclera | CN III (inferior division) | Adduction |
| Lateral rectus | Annulus of Zinn (lateral part) | Lateral sclera | CN VI (Abducent) | Abduction |
| Superior oblique | Body of sphenoid (superomedial to optic canal) | Superior sclera (posterior to equator, via trochlea) | CN IV (Trochlear) | Depression in adduction; intorsion |
| Inferior oblique | Orbital floor (maxilla) | Inferior sclera (posterior to equator) | CN III (inferior division) | Elevation in adduction; extorsion |
The Trochlea — a fibrocartilaginous pulley attached to the frontal bone at the superomedial angle of the orbit. The superior oblique tendon turns 45° through this pulley, which is why it depresses the adducted eye. Damage to the trochlea (e.g., in orbital roof fractures) causes characteristic head tilt.
Levator Palpebrae Superioris (LPS) — the seventh muscle; elevates the upper eyelid. Supplied by CN III (superior division). Also contains smooth muscle fibres (Müller's muscle) supplied by the sympathetic nervous system — their paralysis causes partial ptosis in Horner's syndrome.
Clinical Memory Aid — "LR6 SO4 rest 3":
- Lateral Rectus → CN 6 (abducent)
- Superior Oblique → CN 4 (trochlear)
- All the rest → CN 3 (oculomotor)
Paralysis Patterns:
• CN III palsy: Eye deviated "down and out" (unopposed lateral rectus and superior oblique); complete ptosis; dilated pupil (loss of parasympathetic constriction) — surgical emergency if new onset (aneurysm until proved otherwise)
• CN IV palsy: Patient cannot depress the adducted eye; compensatory head tilt away from the affected side; diplopia on looking down (especially descending stairs)
• CN VI palsy: Medial deviation of eye (esotropia); patient cannot abduct; diplopia on lateral gaze to the affected side

Figure: Extraocular Muscles — Attachments, Nerve Supply, and Actions (AN31.1)

Figure: The Six Muscles that Move the Eyeball
Nerves and Vessels of the Orbit (AN31.2)
Nerves of the Orbit

Figure: Nerves and Vessels of the Orbit (AN31.2)
Motor nerves enter via the superior orbital fissure:
• Oculomotor (CN III) — superior division: superior rectus + LPS; inferior division: medial rectus, inferior rectus, inferior oblique + parasympathetic fibres to ciliary ganglion (pupil constriction, lens accommodation)
• Trochlear (CN IV) — enters orbit outside the common tendinous ring; crosses over the LPS to reach the superior oblique
• Abducent (CN VI) — enters the ring; passes directly into the lateral rectus
Sensory nerve — Ophthalmic nerve (V1), branch of trigeminal (CN V):
Enters via superior orbital fissure and divides into three branches:
1. Lacrimal nerve — lateral orbit; sensation to lacrimal gland, upper eyelid, conjunctiva
2. Frontal nerve — large branch; divides into supraorbital (forehead, scalp) and supratrochlear (medial forehead) nerves
3. Nasociliary nerve — deepest branch; gives long ciliary nerves (corneal sensation; carries sympathetic fibres to dilator pupillae), short ciliary nerves (via ciliary ganglion), and ends as the infratrochlear and anterior/posterior ethmoidal nerves
Autonomic nerves:
• Ciliary ganglion — parasympathetic relay station, located lateral to the optic nerve; preganglionic fibres from CN III → synapse → postganglionic fibres travel in short ciliary nerves → pupil constriction + ciliary muscle (accommodation)
• Sympathetic fibres — travel with nasociliary nerve (long ciliary nerves); supply dilator pupillae and Müller's muscle
Vessels of the Orbit
Ophthalmic artery — first branch of the internal carotid artery (after it exits the cavernous sinus); enters orbit through the optic canal below the optic nerve.
Key branches:
• Central artery of retina — enters optic nerve sheath ~12 mm behind the eyeball; sole blood supply to inner retina — occlusion causes sudden painless monocular blindness (a medical emergency)
• Posterior ciliary arteries (long + short) — supply choroid and outer retina
• Anterior ciliary arteries — from muscular branches; supply iris and ciliary body
• Lacrimal artery — supplies lacrimal gland and sends a branch back to the cavernous sinus (anastomosis with middle meningeal artery — this explains orbital pain in meningeal pathology)
• Supraorbital, supratrochlear — scalp and forehead
Venous drainage:
• Superior ophthalmic vein — drains into the cavernous sinus posteriorly (no valves — explains cavernous sinus thrombosis from facial infections — "danger triangle of the face")
• Inferior ophthalmic vein — also drains to cavernous sinus; communicates with pterygoid plexus
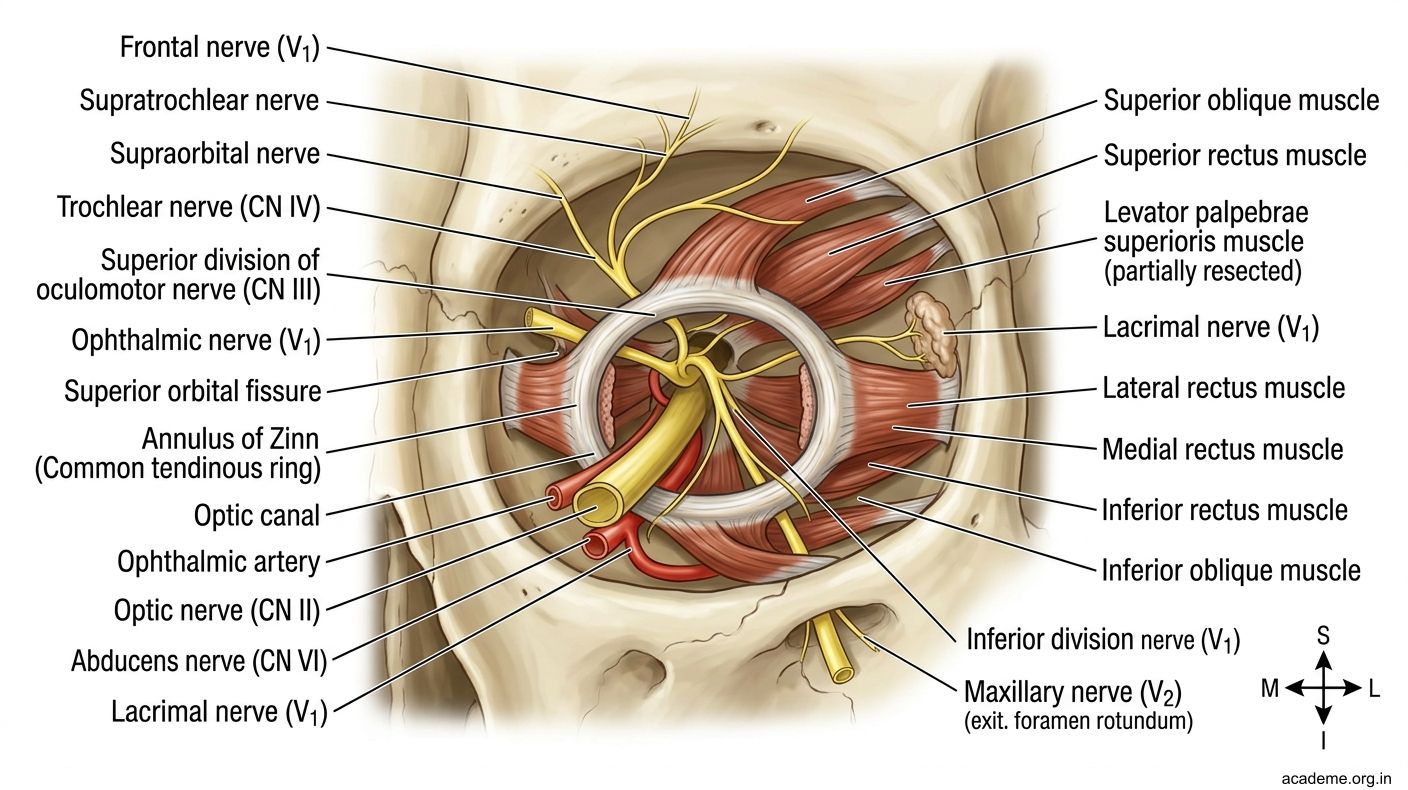
Figure: Nerves and Vessels of the Orbit (AN31.2)

Figure: Vessels of the Orbit
Horner's Syndrome — Anatomical Basis (AN31.3)
Horner's Syndrome is caused by interruption of the oculosympathetic pathway at any point along its three-neuron arc.
The Three-Neuron Sympathetic Pathway to the Eye:
1st order neuron (Central):
Hypothalamus → descends ipsilaterally through brainstem and lateral spinal cord → synapses at ciliospinal centre of Budge (C8–T2)
Lesions: brainstem stroke, syringomyelia, demyelination
2nd order neuron (Preganglionic):
Ciliospinal centre → exits T1 root → loops over the apex of the lung and subclavian artery → ascends along the common carotid artery → synapses in the superior cervical ganglion (at C2–C3 level)
Lesions: Pancoast tumour (apex of lung — common in smokers), cervical rib, thyroid surgery, neck dissection, brachial plexus birth injury
3rd order neuron (Postganglionic):
Superior cervical ganglion → fibres travel with the internal carotid artery into the cavernous sinus → join the nasociliary nerve (V1) → reach the orbit via long ciliary nerves
Lesions: carotid dissection, cavernous sinus pathology, cluster headache
Classic Triad of Horner's Syndrome:
1. Ptosis — partial drooping (Müller's muscle paralysed; LPS intact — hence "partial" not complete)
2. Miosis — constricted pupil (dilator pupillae paralysed; sphincter unchecked)
3. Anhidrosis — absent sweating on the ipsilateral face (sudomotor fibres interrupted — present only in 1st and 2nd order neuron lesions)
4. (Sometimes listed): Enophthalmos — apparent sunken eye (inferior tarsal muscle and orbitalis paralysed)
Pharmacological confirmation: Cocaine eye drops fail to dilate the affected pupil (as cocaine acts by blocking reuptake of noradrenaline, which is not being released). Hydroxyamphetamine differentiates 2nd from 3rd order neuron lesions.

Figure: The Three-Neuron Sympathetic Pathway to the Eye: