Page 1 of 4
AN33.1-5 | Temporal and Infratemporal regions — SDL Guide
Learning Objectives
- Describe and demonstrate the extent, boundaries, and contents of the temporal and infratemporal fossae (AN33.1)
- Describe and demonstrate the attachments, direction of fibres, nerve supply, and actions of the muscles of mastication (AN33.2)
- Describe and demonstrate the articulating surfaces, type, and movements of the temporomandibular joint (AN33.3)
- Explain the clinical significance of the pterygoid venous plexus (AN33.4)
- Describe the features of dislocation of the temporomandibular joint (AN33.5)
INSTRUCTIONS
The infratemporal fossa is the most complex region of the head. Work methodically: boundaries → muscles → vessels → nerves → joint. Use a skull to visualise the fossae.
References
- Gray's Anatomy for Students — Head and Neck: Temporal and Infratemporal Fossae (Textbook)
- BD Chaurasia's Human Anatomy Vol. 3 — Infratemporal Fossa (Textbook)
- Oral and Maxillofacial Surgery (Hupp et al.) — Temporomandibular Joint (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 28-year-old woman arrives at a government hospital in Pondicherry with her mouth locked wide open after yawning. She is in obvious distress, drooling, and cannot close her jaw. Relatives say this happened suddenly and she has had similar episodes before that resolved on their own.
What joint has dislocated? What anatomical structure normally prevents this? What is the emergency bedside manoeuvre to reduce this dislocation?
By the end of this module, you will understand the anatomy of the temporomandibular joint and the muscles of mastication well enough to answer these questions and reduce a dislocated jaw.
WHY THIS MATTERS
The temporal and infratemporal regions are central to dentistry, maxillofacial surgery, and neurology practice in India:
- Temporomandibular joint (TMJ) disorders — affecting up to 10–15% of the adult population; common presentation in dental OPDs
- Inferior alveolar nerve block — the most common nerve block in dentistry, delivered into the infratemporal fossa to anaesthetise the mandibular teeth
- Infratemporal fossa tumours — extensions of nasopharyngeal carcinoma (NPC), commonly seen in South India; present with trismus (inability to open mouth)
- Pterygoid venous plexus — routes for spread of dental infections to the cavernous sinus (life-threatening)
- TMJ dislocation — common emergency in casualty departments; requires knowledge of Hippocratic manoeuvre
RECALL
Before we begin, recall:
- The mandible is the only movable bone of the skull
- The trigeminal nerve (CN V) is the principal sensory and motor nerve of the head — CN V3 (mandibular) provides motor supply to all muscles of mastication
- The maxillary artery (terminal branch of external carotid artery) is the dominant vessel of the infratemporal fossa
- The foramen ovale (CN V3) and foramen spinosum (middle meningeal artery) are foramina in the base of the skull relevant to this region
Temporal and Infratemporal Fossae — Boundaries and Contents (AN33.1)
Temporal Fossa
- Boundaries: Superiorly/anteriorly — superior + inferior temporal lines; Anteriorly — frontal and zygomatic bones; Posteriorly — temporal bone; Inferiorly — zygomatic arch (roof of infratemporal fossa)
- Contents: Temporalis muscle, deep temporal vessels (from maxillary artery), deep temporal nerves (from CN V3), small amount of fat
- Floor: Formed by parts of the frontal, parietal, temporal, and sphenoid bones — this meeting point is called the pterion (weakest part of the skull; overlies the anterior branch of the middle meningeal artery — vulnerable in head trauma)
Infratemporal Fossa (ITF)
- Location: Deep to the ramus of mandible; below and medial to the zygomatic arch; behind the maxilla
- Boundaries:
- Lateral — ramus and coronoid process of mandible
- Medial — lateral pterygoid plate (sphenoid)
- Anterior — posterior surface of maxilla
- Superior — inferior surface of greater wing of sphenoid + squamous temporal bone (infratemporal surface)
- Posterior — open (communicates with the parapharyngeal space)
- No floor (opens inferiorly into the neck)
- Communications:
- With the temporal fossa — through the gap between zygomatic arch and skull (deep to masseter)
- With the pterygopalatine fossa — through the pterygomaxillary fissure (medially)
- With the middle cranial fossa — through foramen ovale (CN V3), foramen spinosum (middle meningeal vessels)
Contents of the ITF (the densely packed space):
1. Muscles: Lower head of lateral pterygoid + medial pterygoid (+ lower parts of temporalis)
2. Vessels: Maxillary artery (and its branches) + pterygoid venous plexus
3. Nerves: Mandibular nerve (CN V3) and its branches; chorda tympani (CN VII); otic ganglion

Figure: Temporal and Infratemporal Fossae — Boundaries and Contents (AN33.1)
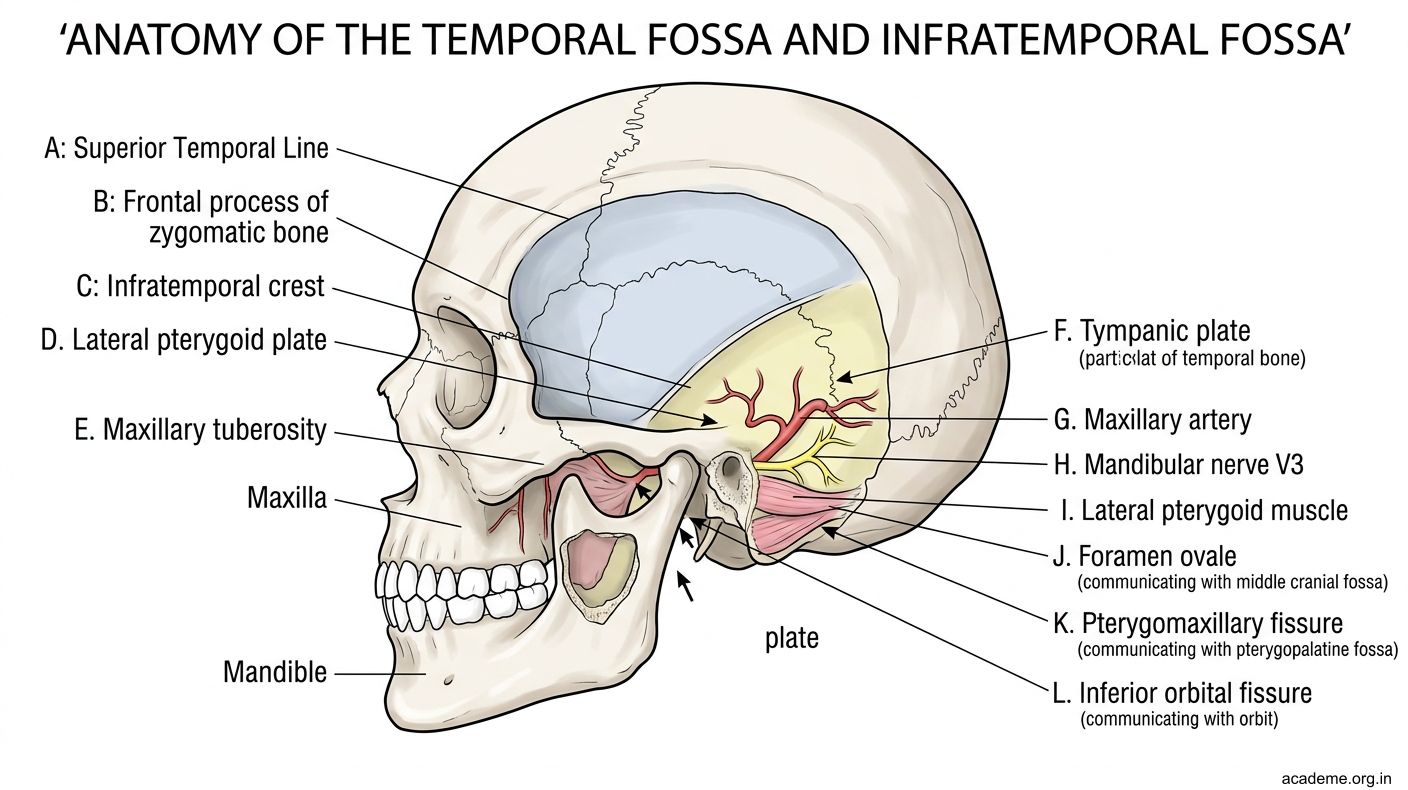
Figure: Temporal and Infratemporal Fossae — Boundaries and Contents (AN33.1)
Muscles of Mastication — Attachments, Actions, and Nerve Supply (AN33.2)
All four muscles of mastication are supplied by the anterior division of CN V3 (mandibular nerve) — specifically by the nerve to masseter, deep temporal nerves, and nerve to pterygoids.
1. Temporalis
- Origin: Temporal fossa (floor and walls) + temporal fascia
- Insertion: Coronoid process + anterior border of ramus of mandible
- Nerve: Deep temporal nerves (anterior division, CN V3)
- Action: Elevation (closing jaw) + Retraction of mandible (posterior fibres); anterior fibres also assist in protraction
- Clinical: Wasting of temporalis visible as hollowing of the temple in malnutrition and motor neuron disease; trismus (inability to open jaw) from temporalis spasm or invasion
2. Masseter
- Origin: Superficial head — lower border of zygomatic arch (anterior 2/3); Deep head — medial surface of zygomatic arch
- Insertion: Lateral surface of ramus and coronoid process of mandible
- Nerve: Masseteric nerve (anterior division, CN V3); enters through the mandibular notch
- Action: Elevation (main biting muscle) + some protraction (superficial head)
- Clinical: Hypertrophy with bruxism (teeth grinding — common in stressed students); parotid gland overlies the masseter
3. Medial Pterygoid
- Origin: Deep head — medial surface of lateral pterygoid plate; Superficial head — tuberosity of maxilla and pyramidal process of palatine bone
- Insertion: Medial surface of angle of mandible (pterygoid fossa)
- Nerve: Medial pterygoid nerve (main trunk, CN V3)
- Action: Elevation + protraction + medial excursion (side-to-side grinding)
- Note: Acts as a medial sling with masseter to suspend the mandible — together they form a "pterygomasseter sling"
4. Lateral Pterygoid
- Origin: Upper head — infratemporal surface and crest of greater wing of sphenoid; Lower head — lateral surface of lateral pterygoid plate
- Insertion: Pterygoid fovea on the neck of mandibular condyle; articular disc of TMJ (upper head)
- Nerve: Lateral pterygoid nerve (anterior division, CN V3)
- Action: Protraction + depression (opening jaw) — bilateral: opens mouth + protrudes; unilateral: side-to-side movement (lateral excursion to opposite side)
- Critical point: The lateral pterygoid is the ONLY muscle of mastication that opens the mouth — all others close it. If both lateral pterygoids contract simultaneously, the jaw protrudes and opens.
Memory Summary:
| Muscle | Elevation | Depression | Protraction | Retraction |
|---|---|---|---|---|
| Temporalis | ✓ (all) | ✓ (posterior) | ||
| Masseter | ✓ | ✓ (superficial) | ||
| Medial pterygoid | ✓ | ✓ | ||
| Lateral pterygoid | ✓ | ✓ |

Figure: Muscles of Mastication — Attachments, Actions, and Nerve Supply (AN33.2)
Temporomandibular Joint (TMJ) (AN33.3)
Type: Synovial condylar joint (modified hinge); bicondylar joint

Figure: Temporomandibular Joint (TMJ) (AN33.3)
Articulating Surfaces:
- Above: Articular tubercle (anterior part of mandibular fossa) + mandibular fossa (glenoid fossa) of the temporal bone — lined with fibrocartilage (NOT hyaline cartilage — important distinction)
- Below: Head (condyle) of the mandible — also covered with fibrocartilage
Articular Disc:
A fibrocartilaginous biconcave disc that divides the joint into two compartments:
- Upper (temporodiscal) compartment — gliding movements (protraction/retraction)
- Lower (discoidal) compartment — hinge/rotation movements (elevation/depression)
The disc is attached anteriorly to the upper head of the lateral pterygoid muscle, accounting for anterior disc displacement in TMJ disorders.
Ligaments:
1. Temporomandibular (lateral) ligament — thickening of the joint capsule; strongest ligament; limits posterior movement of the condyle
2. Sphenomandibular ligament — medial accessory ligament; from spine of sphenoid → lingula of mandibular foramen; not part of the capsule
3. Stylomandibular ligament — from styloid process → angle of mandible; separates parotid from submandibular gland
Movements:
1. Depression (opening): Rotation in lower compartment + translation (gliding forward) in upper compartment. Lateral pterygoid initiates opening; digastric + mylohyoid + geniohyoid assist.
2. Elevation (closing): Reverse; masseter, medial pterygoid, temporalis.
3. Protraction: Both lateral pterygoids; upper compartment gliding.
4. Retraction: Posterior fibres of temporalis + digastric.
5. Lateral excursion (chewing): Unilateral lateral pterygoid of the opposite side + ipsilateral masseter/temporalis.
Blood supply: Superficial temporal + maxillary arteries (branches of ECA)
Nerve supply: Auriculotemporal nerve + masseteric nerve (both from CN V3)

Figure: Memory Summary:
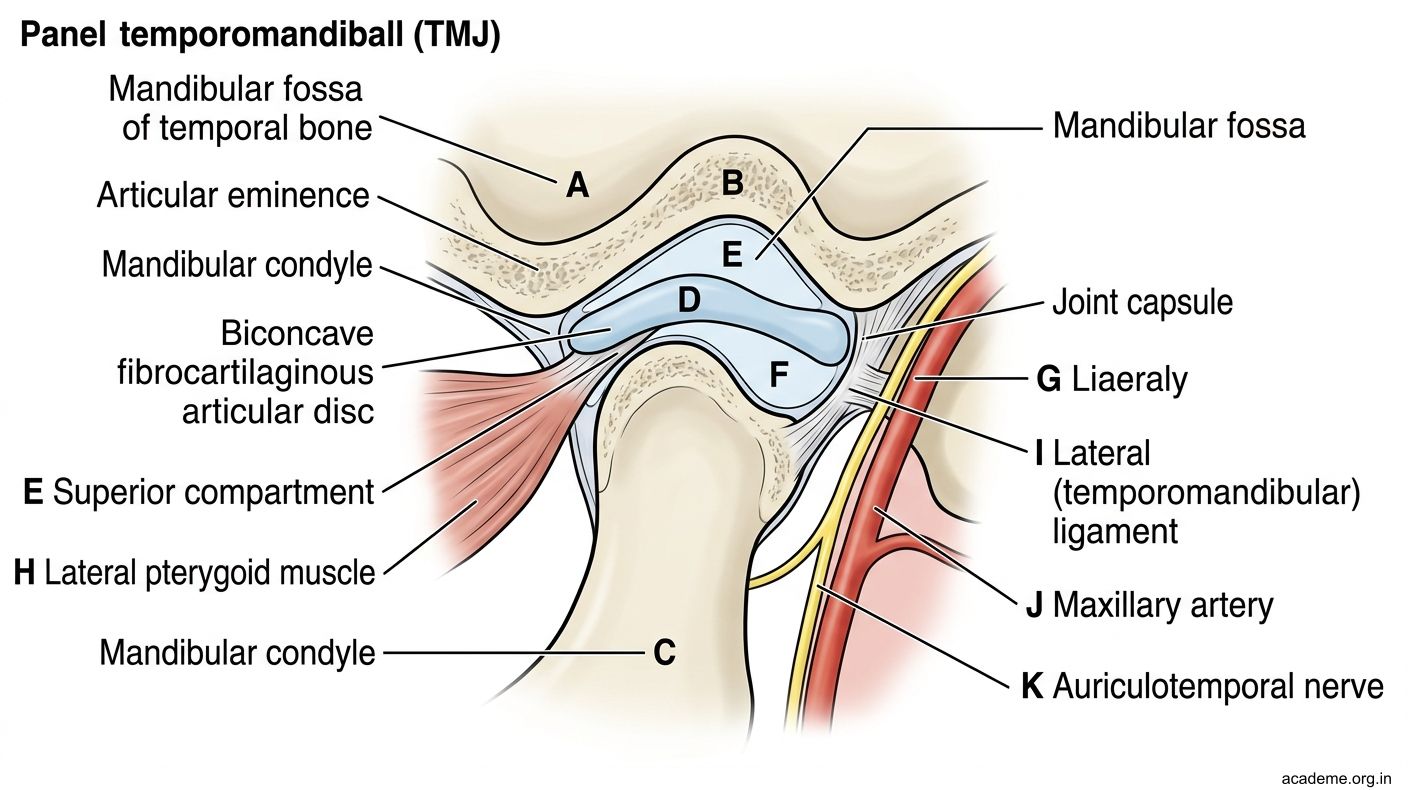
Figure: Temporomandibular Joint (TMJ) (AN33.3)
Pterygoid Venous Plexus and TMJ Dislocation (AN33.4 & AN33.5)
Pterygoid Venous Plexus (AN33.4)
The pterygoid venous plexus is a dense network of veins lying in the infratemporal fossa, surrounding the pterygoid muscles.
Tributaries: Middle meningeal veins, deep temporal veins, masseteric vein, infraorbital vein, greater palatine vein, sphenopalatine vein, inferior ophthalmic vein.
Drainage: → Maxillary vein → joins the superficial temporal vein to form the retromandibular vein → ultimately drains into the internal and external jugular veins.
Clinical significance:
1. Route for infection spread: Dental infections (especially upper molar teeth → pterygopalatine fossa → pterygoid plexus) can spread to the cavernous sinus via emissary veins (including a connection through foramen ovale and foramen of Vesalius). This is a potentially fatal complication.
2. Dangerous injections: Aspiration is mandatory before inferior alveolar nerve block — inadvertent injection into the pterygoid plexus causes a haematoma in the ITF.
3. Anastomosis with the cavernous sinus: Via the deep facial vein (from angular vein → pterygoid plexus), emissary veins through foramen ovale and foramen spinosum.
Dislocation of the TMJ (AN33.5)
Definition: Anterior dislocation — the condyle moves forward, over the articular tubercle, and becomes locked in front of it. It cannot return on its own because the elevator muscles (masseter, temporalis, medial pterygoid) hold it in spasm.
Why does it happen?
- Excessive mouth opening (wide yawning, prolonged dental procedures, general anaesthesia intubation)
- Laxity of the temporomandibular + capsular ligaments
- Shallow articular fossa or low articular tubercle
Clinical features:
- Mouth fixed open (cannot close)
- Jaw deviated toward the unaffected side (if unilateral)
- Pre-auricular hollow (condyle no longer palpable in the fossa)
- Pain and muscle spasm
Reduction — Hippocratic manoeuvre:
1. Stand facing the seated patient
2. Place thumbs (wrapped in gauze) on the lower molar teeth bilaterally
3. Fingers grip the lower border of the mandible
4. Apply firm downward and backward pressure: thumbs push molars down (clearing the articular tubercle), fingers lift the chin up
5. The condyle slides back into the mandibular fossa — a "clunk" is felt
Post-reduction: Bandage the jaw for 2–4 weeks; avoid wide opening; treat underlying hypermobility.

Figure: Pterygoid Venous Plexus (AN33.4)

Figure: Dislocation of the TMJ (AN33.5)

Figure: The Pterion — Where the Skull is Thinnest

Figure: Classic presentation

Figure: Temporal and Infratemporal Regions — Key Points
SELF-CHECK — : Temporal and Infratemporal Regions
Which muscle of mastication is the ONLY one capable of opening the mouth (depressing the mandible)?
A. Masseter
B. Medial pterygoid
C. Temporalis (posterior fibres)
D. Lateral pterygoid
Reveal Answer
Answer: D. Lateral pterygoid
The articular surfaces of the TMJ are lined with which type of cartilage (unusual for a synovial joint)?
A. Hyaline cartilage
B. Elastic cartilage
C. Fibrocartilage
D. Calcified cartilage
Reveal Answer
Answer: C. Fibrocartilage
Dental infections can spread from the infratemporal fossa to the cavernous sinus via the pterygoid venous plexus through which pathway?
A. Superior ophthalmic vein directly
B. Emissary veins through foramen ovale and foramen spinosum
C. Internal jugular vein retrograde
D. Inferior petrosal sinus
Reveal Answer
Answer: B. Emissary veins through foramen ovale and foramen spinosum
CLINICAL PEARL
The Pterion — Where the Skull is Thinnest
The pterion is the H-shaped suture where four bones meet: frontal, parietal, temporal, and greater wing of sphenoid. It is the thinnest point of the skull (as little as 2–3 mm). Directly deep to it runs the anterior division of the middle meningeal artery (a branch of the maxillary artery, entering the skull through foramen spinosum).
A blow to the temple (assault, road traffic accident, fall in an elderly person) fractures the thin pterion and tears the middle meningeal artery → extradural (epidural) haematoma — blood accumulates between the skull and the dura mater, stripping the dura.
Classic presentation: Lucid interval → progressive headache → contralateral hemiplegia → ipsilateral dilated pupil (herniation) → coma.
This is a surgical emergency — burr hole craniotomy at the pterion to evacuate the haematoma. Every doctor must know this anatomy.
REFLECT
A dentist gives an inferior alveolar nerve block. The patient reports sudden swelling in the cheek and difficulty opening the mouth. What anatomical complication has occurred? Which vascular structure has been inadvertently injected or traumatised? How could this have been prevented?
KEY TAKEAWAYS
Temporal and Infratemporal Regions — Key Points
- Pterion: H-shaped suture, thinnest skull point; overlies middle meningeal artery (anterior branch) — risk of extradural haematoma.
- ITF contents: Lateral + medial pterygoid muscles, maxillary artery, pterygoid venous plexus, CN V3 branches, chorda tympani, otic ganglion.
- Muscles of mastication (all CN V3): Temporalis (elevation + retraction), Masseter (elevation), Medial pterygoid (elevation + protraction), Lateral pterygoid (ONLY opener + protraction).
- TMJ: Bicondylar synovial joint; fibrocartilage lined; articular disc divides into upper (gliding) and lower (hinge) compartments; anterior disc attached to lateral pterygoid.
- TMJ dislocation: Condyle locks anterior to articular tubercle; reduce with Hippocratic manoeuvre (thumbs on lower molars, push down and back).
- Pterygoid venous plexus: Connects to cavernous sinus via foramen ovale emissary veins — route for dental infection → intracranial spread.