Page 1 of 4
AN39.1-2 | Tongue — SDL Guide
Learning Objectives
- Describe the morphology, intrinsic and extrinsic muscles of the tongue with their attachments, nerve supply, and actions (AN39.1)
- Explain the embryological basis of tongue nerve supply — general sensory versus taste fibres (AN39.1)
- Describe the blood supply and lymphatic drainage of the tongue with clinical correlations (AN39.1)
- Explain the anatomical basis of hypoglossal nerve palsy and the clinical sign of tongue deviation (AN39.2)
- Correlate tongue anatomy with clinical conditions: lingual carcinoma, Ludwig's angina, and glossitis
INSTRUCTIONS
Work through this module section by section. Complete micro-quizzes before moving forward. Refer to dissection specimens and your atlas while reading.
References
- Gray's Anatomy for Students (Drake et al.) — Chapter 8: Head and Neck (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 3 — Head & Neck (Textbook)
- Clinically Oriented Anatomy (Moore et al.) — Oral Region (Textbook)
- OpenStax Anatomy and Physiology 2e — Digestive System (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 55-year-old beedi-maker from Cuddalore presents to a government hospital with a painless ulcer on the lateral border of his tongue that has been present for three weeks. On clinical examination, the neurologist asks him to protrude his tongue — it deviates to the left. There is also reduced sensation on the left anterior two-thirds of the tongue.
Which nerve is injured and where? Why does the tongue deviate to the affected side? Is the deviated tongue related to the ulcer?
Understanding tongue anatomy will allow you to answer each of these questions with confidence.
WHY THIS MATTERS
The tongue is one of the most functionally complex structures in the head and neck. As a medical student and future doctor, tongue anatomy is directly relevant to:
- Oral cancer — India has among the highest rates of oral squamous cell carcinoma in the world, with the lateral tongue border being the most common site; understanding lymphatic drainage guides surgical neck dissection
- Hypoglossal nerve palsy — seen in carotid endarterectomy complications, neck dissections, penetrating injuries, and posterior cranial fossa tumours
- Ludwig's angina — a life-threatening cellulitis of the floor of mouth spreading via sublingual and submandibular spaces; one of the most dangerous infections in dentistry
- Swallowing and speech disorders — tongue paralysis from stroke or motor neuron disease causes profound disability
- Regional anaesthesia — lingual nerve block for dental procedures requires precise anatomical knowledge
RECALL
Before we begin, recall key points from earlier anatomy:
- The oral cavity is divided into the vestibule and the oral cavity proper by the alveolar arches and teeth
- The mylohyoid muscle forms the muscular floor of the mouth — it is the key structure separating the sublingual and submandibular spaces
- The hypoglossal nerve (CN XII) is a pure motor nerve that exits the skull via the hypoglossal canal in the occipital bone
- Taste sensation is conveyed by CN VII (anterior 2/3), CN IX (posterior 1/3), and CN X (epiglottis/base)
- The tongue develops from two lingual swellings and the tuberculum impar (anterior 2/3) fused with the copula (posterior 1/3)
Part 1: Morphology and Muscle Groups of the Tongue (AN39.1)
Subdivisions of the Tongue

Figure: Extrinsic Muscles of the Tongue

Figure: Part 1: Morphology and Muscle Groups of the Tongue (AN39.1)
The tongue is divided into:
• Anterior 2/3 (oral/presulcal part) — visible in the mouth, separated from the posterior 1/3 by the sulcus terminalis (V-shaped groove) and the foramen caecum (remnant of thyroglossal duct origin)
• Posterior 1/3 (pharyngeal/postsulcal part) — faces the oropharynx; contains the lingual tonsil (lymphoid follicles)
• Root — fixed posterior attachment to the hyoid bone and mandible
• Tip (apex) — free anterior end
• Dorsum — superior surface with papillae
• Inferior surface — covered by thin mucosa; contains the lingual frenulum (midline fold connecting tongue to floor of mouth)
Papillae of the Tongue (Dorsal Surface)
| Papilla Type | Location | Function | Clinical Note |
|---|---|---|---|
| Filiform | Anterior 2/3, parallel rows | Touch/texture (no taste) | Coated tongue = excess keratin accumulation |
| Fungiform | Scattered among filiform | Taste (CN VII) | Visible as small red spots |
| Circumvallate (vallate) | Row of 8–12 along sulcus terminalis | Taste (CN IX) | Largest papillae; each surrounded by a moat |
| Foliate | Lateral borders, posterior | Taste (CN VII, CN IX) | Atrophy in iron deficiency anaemia |
Intrinsic Muscles of the Tongue
The intrinsic muscles are contained entirely within the tongue. They alter the shape of the tongue:
- Superior longitudinal — shortens tongue, turns tip up and broadens it
- Inferior longitudinal — shortens tongue, turns tip down
- Transverse — narrows and elongates tongue
- Vertical — flattens and widens tongue
All intrinsic muscles are supplied by the hypoglossal nerve (CN XII).
Extrinsic Muscles of the Tongue
These muscles arise outside the tongue and control its position:
| Muscle | Origin | Action | Nerve |
|---|---|---|---|
| Genioglossus | Mental spine of mandible | Protrudes and depresses tongue | CN XII |
| Hyoglossus | Body and greater horn of hyoid | Depresses and retracts tongue | CN XII |
| Styloglossus | Styloid process | Retracts and elevates tongue | CN XII |
| Palatoglossus | Palatine aponeurosis | Elevates posterior tongue; closes oropharyngeal isthmus | CN X (vagus) — NOT CN XII |
Key fact: Palatoglossus is the only tongue muscle NOT supplied by CN XII. It is supplied by the vagus (CN X) via the pharyngeal plexus.
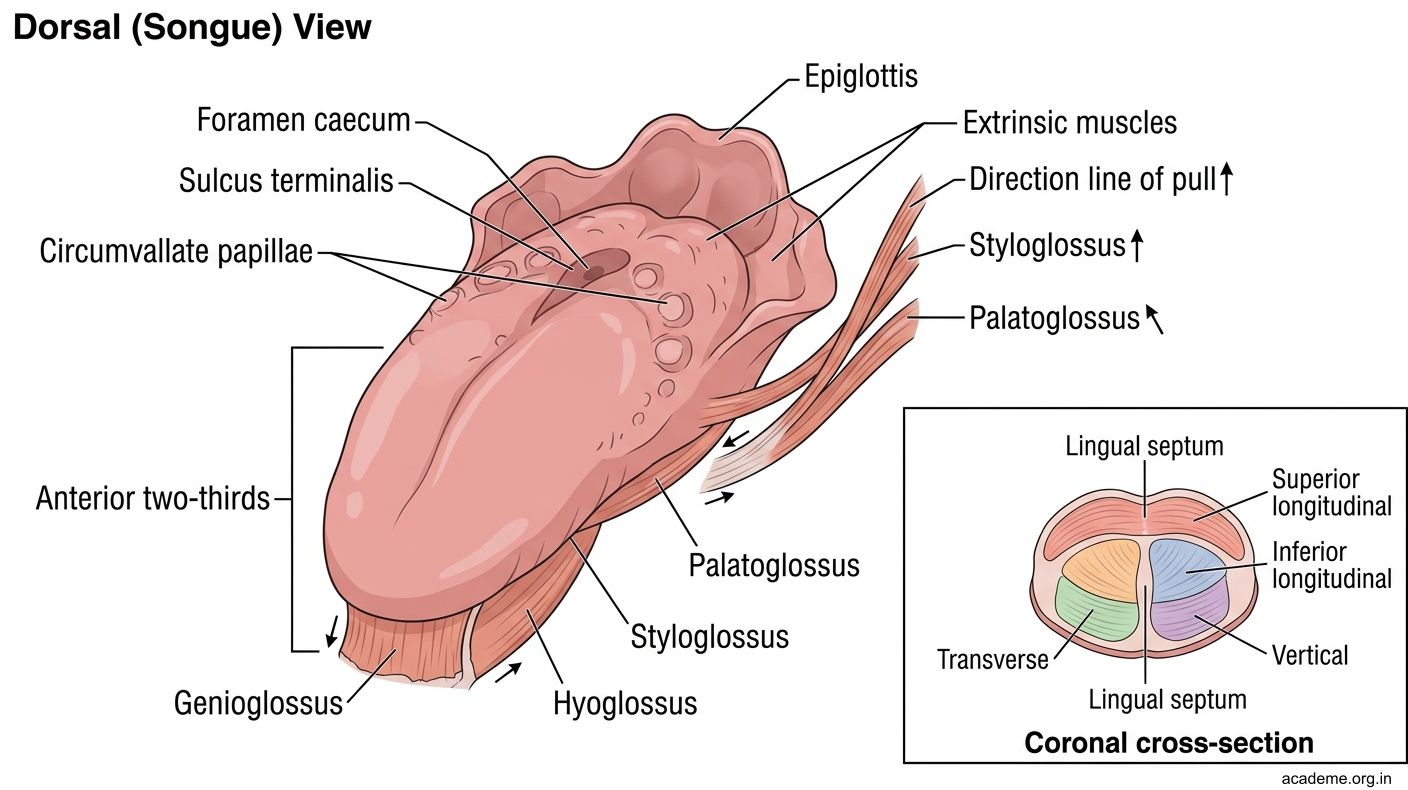
Figure: Part 1: Morphology and Muscle Groups of the Tongue (AN39.1)

Figure: Papillae of the Tongue (Dorsal Surface)
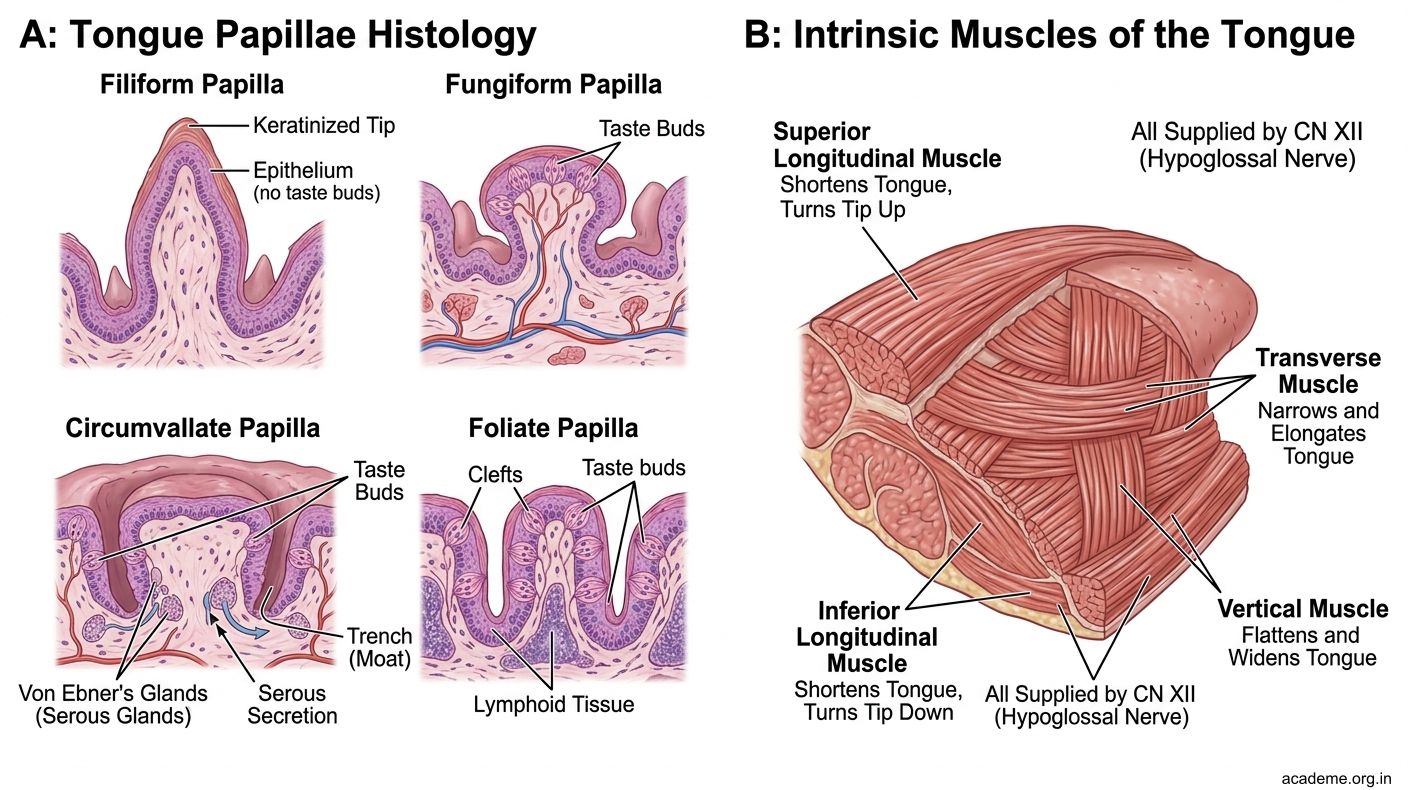
Figure: Papillae of the Tongue (Dorsal Surface)
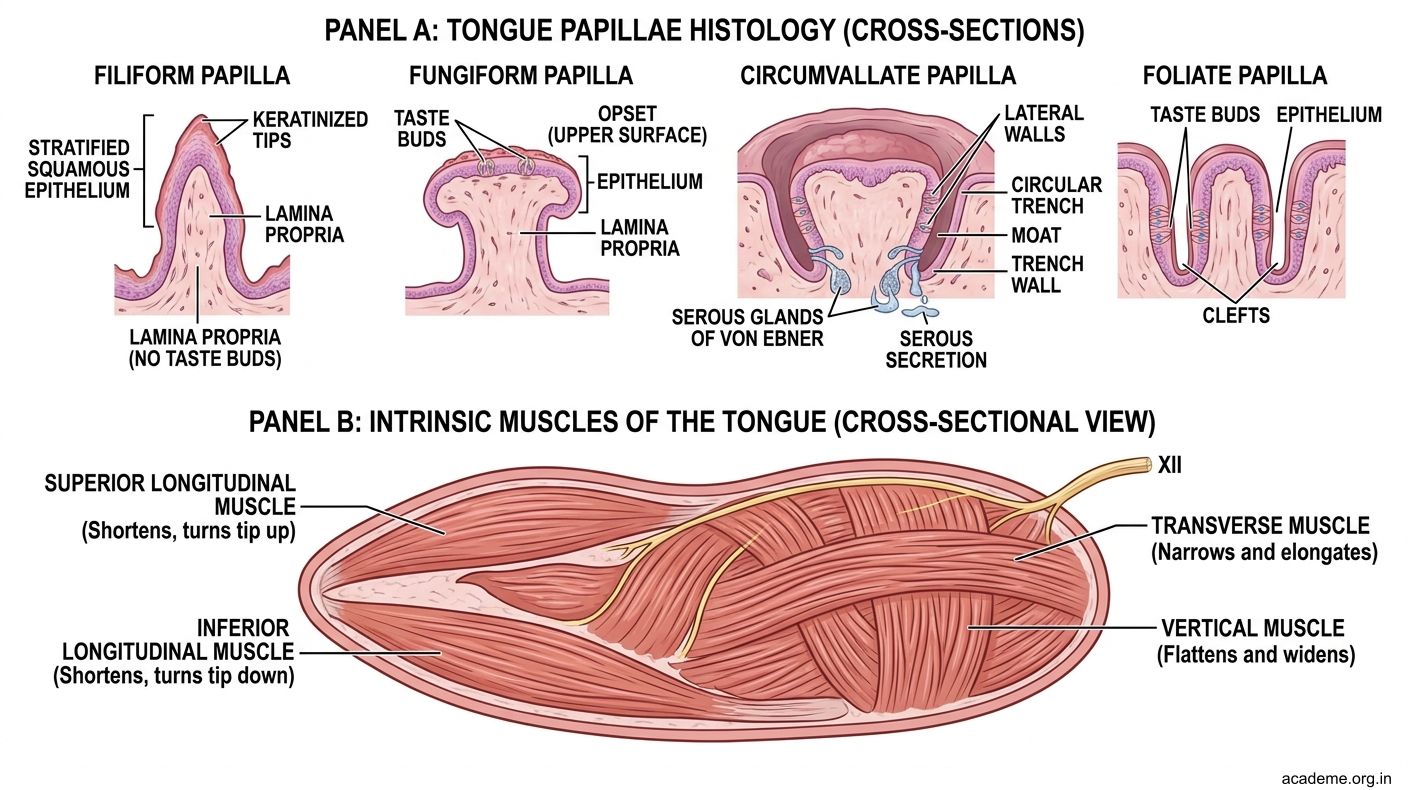
Figure: Papillae of the Tongue (Dorsal Surface)
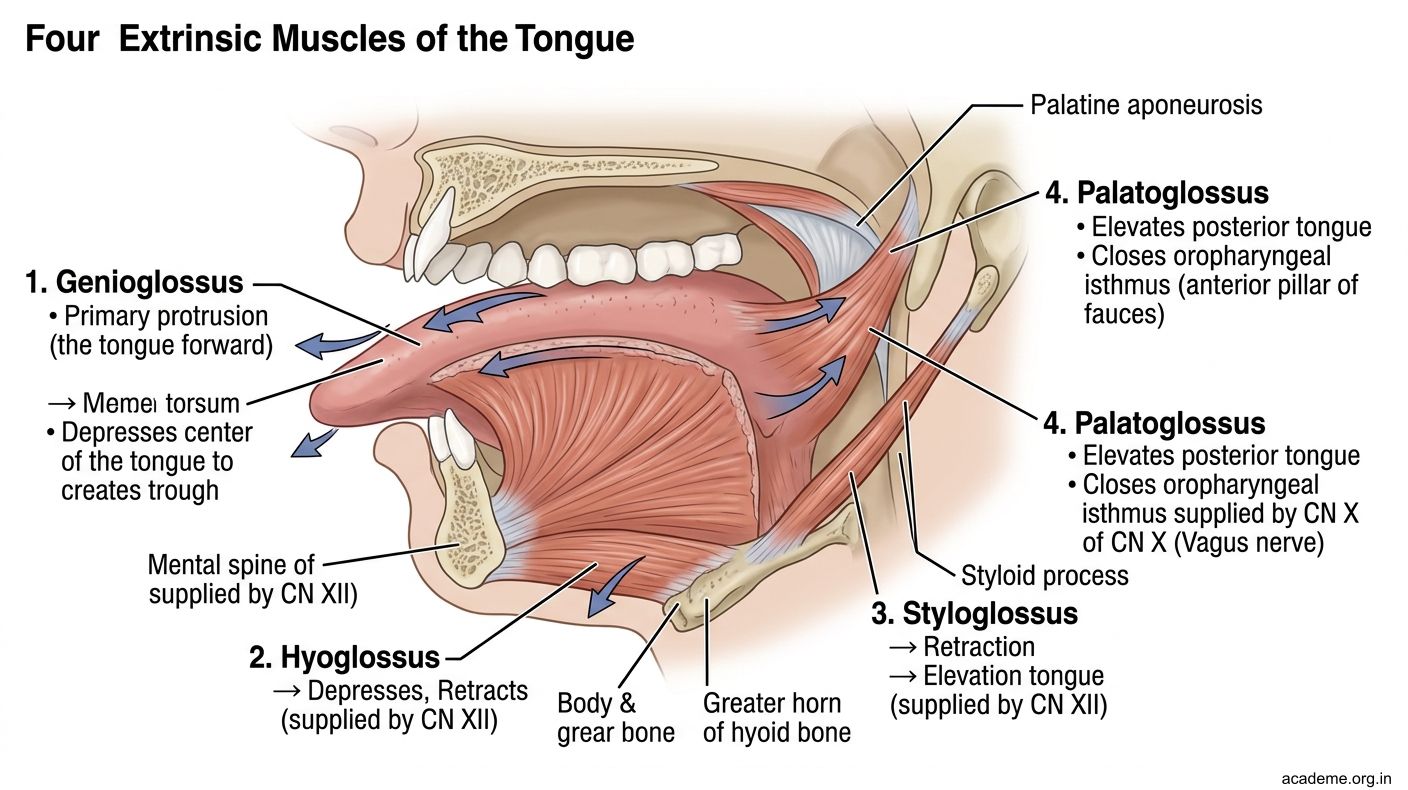
Figure: Extrinsic Muscles of the Tongue
Part 2: Blood Supply, Lymphatic Drainage, and Nerve Supply (AN39.1)
Blood Supply of the Tongue

Figure: Lymphatic Drainage — Clinically Critical (AN39.1)

Figure: Part 2: Blood Supply, Lymphatic Drainage, and Nerve Supply (AN39.1)
Arterial supply: The lingual artery (branch of the external carotid artery) is the primary supply. It enters the tongue between the hyoglossus and genioglossus muscles. Branches:
• Dorsal lingual arteries — supply posterior tongue and epiglottis
• Deep lingual artery — runs to the tip of tongue along the inferior surface (visible as a pulsating vessel)
• Sublingual artery — supplies floor of mouth
Clinical note: In tongue surgery or haemorrhage, the lingual artery must be ligated bilaterally because the two tongues share vascular anastomoses at the midline.
Venous drainage: The deep lingual vein runs with the lingual nerve and drains into the internal jugular vein via the lingual vein.
Lymphatic Drainage — Clinically Critical (AN39.1)
Understanding lymph drainage determines the extent of neck dissection in tongue cancer:
| Region of Tongue | Primary Nodes | Secondary Nodes |
|---|---|---|
| Tip | Submental nodes (level I) | Bilateral deep cervical (risk of bilateral spread) |
| Lateral borders | Submandibular nodes (level I), then deep cervical (level II-III) | Contralateral nodes possible |
| Posterior 1/3 | Deep cervical (level II-III) directly | Bilateral drainage common |
Clinical pearl: Tongue cancer at the tip or medial border has bilateral lymphatic drainage — necessitating bilateral neck dissection. Lateral border carcinoma drains ipsilaterally first.
Nerve Supply of the Tongue (AN39.1)
| Sensation | Area | Nerve |
|---|---|---|
| General sensory (touch/pain/temp) | Anterior 2/3 | Lingual nerve (CN V3 — mandibular) |
| Taste | Anterior 2/3 | Chorda tympani (CN VII) via lingual nerve |
| General sensory + taste | Posterior 1/3 | Glossopharyngeal nerve (CN IX) |
| General sensory + taste | Base/epiglottis | Vagus nerve (CN X) — superior laryngeal nerve |
| Motor | All intrinsic + all extrinsic (except palatoglossus) | Hypoglossal nerve (CN XII) |
Embryological basis of tongue nerve supply:
The anterior 2/3 develops from the first pharyngeal arch (general sensory = CN V3 — mandibular nerve). Taste buds migrate along with the chorda tympani (CN VII). The posterior 1/3 develops from the third pharyngeal arch (CN IX). The developmental boundary is the sulcus terminalis — not a mucosal fold, but the nerve supply boundary is sharp at this line.
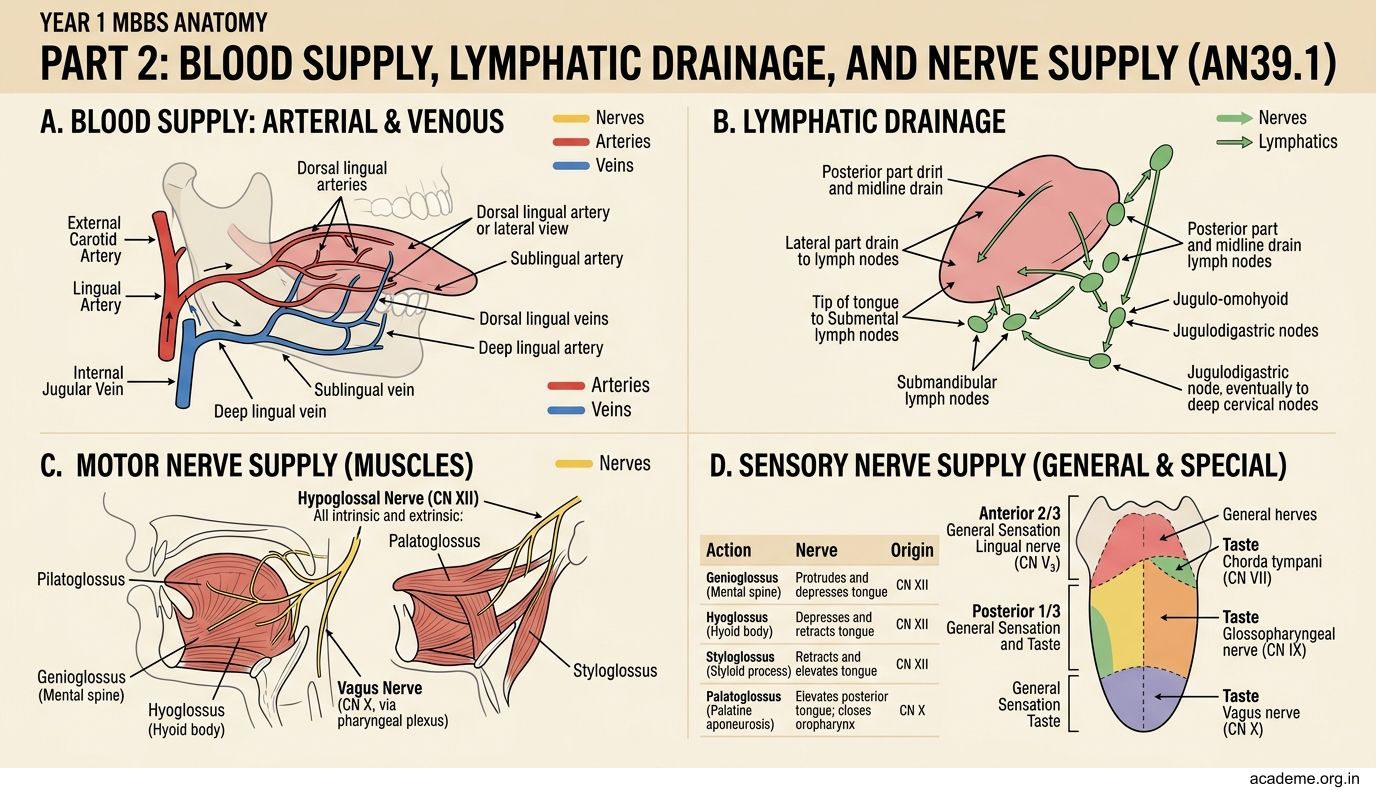
Figure: Part 2: Blood Supply, Lymphatic Drainage, and Nerve Supply (AN39.1)
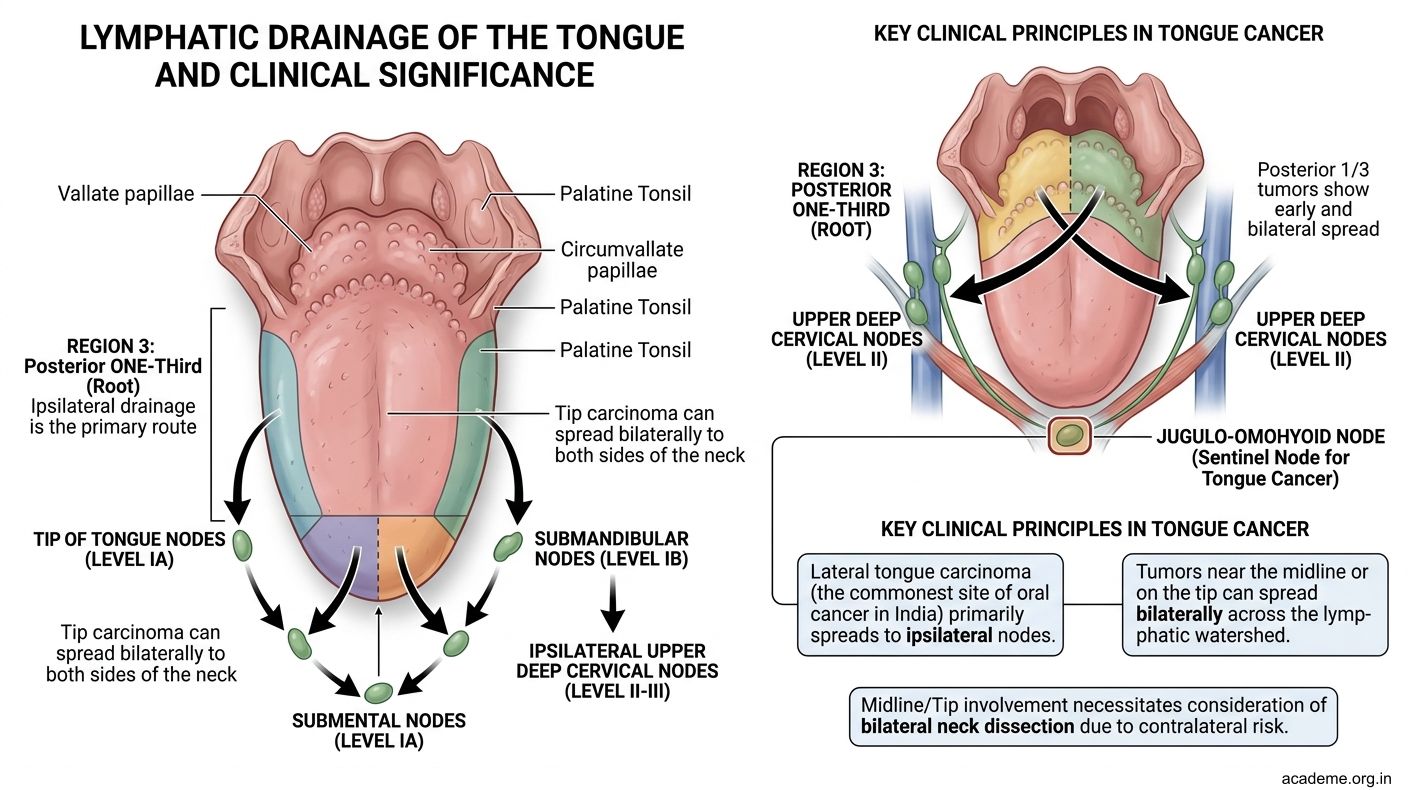
Figure: Lymphatic Drainage — Clinically Critical (AN39.1)

Figure: Nerve Supply of the Tongue (AN39.1)
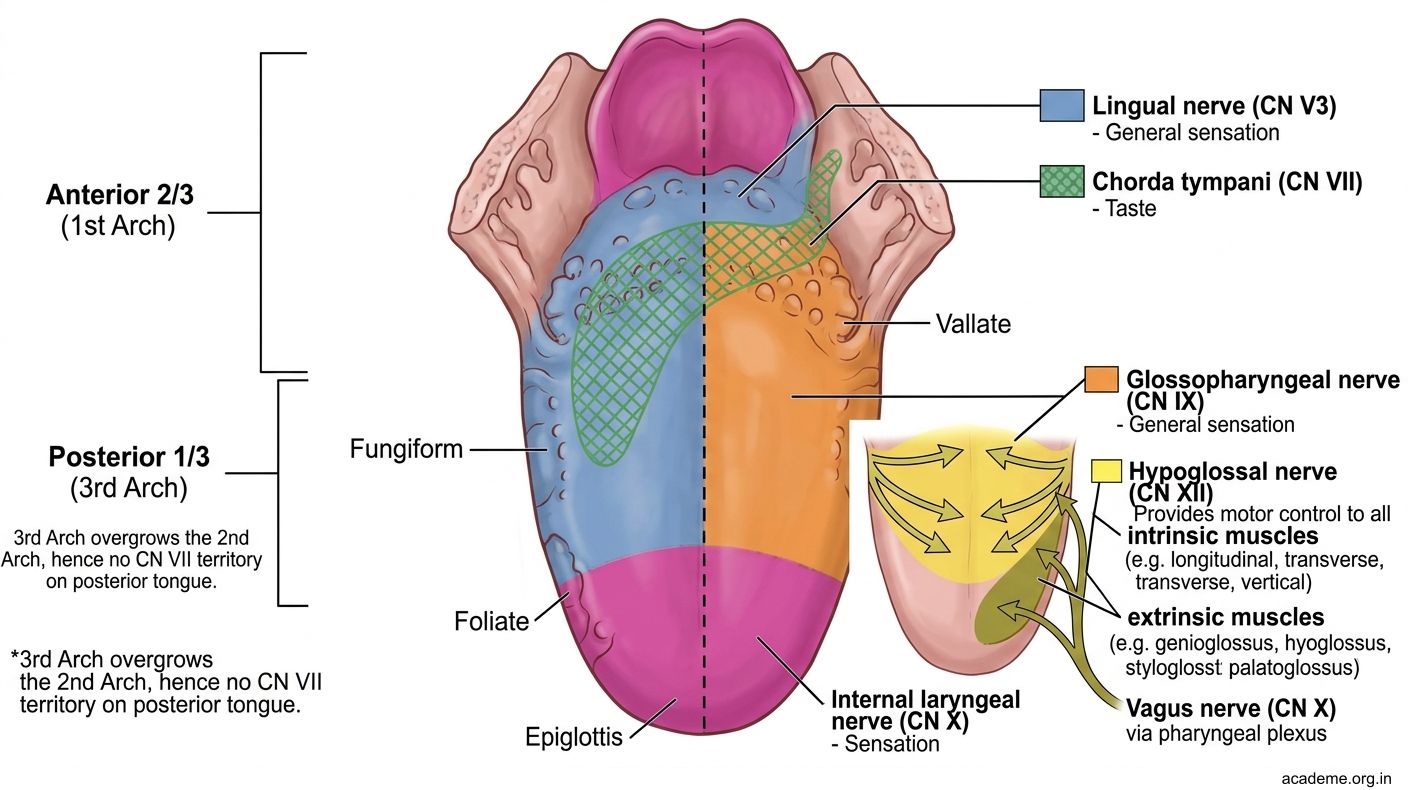
Figure: Nerve Supply of the Tongue (AN39.1)
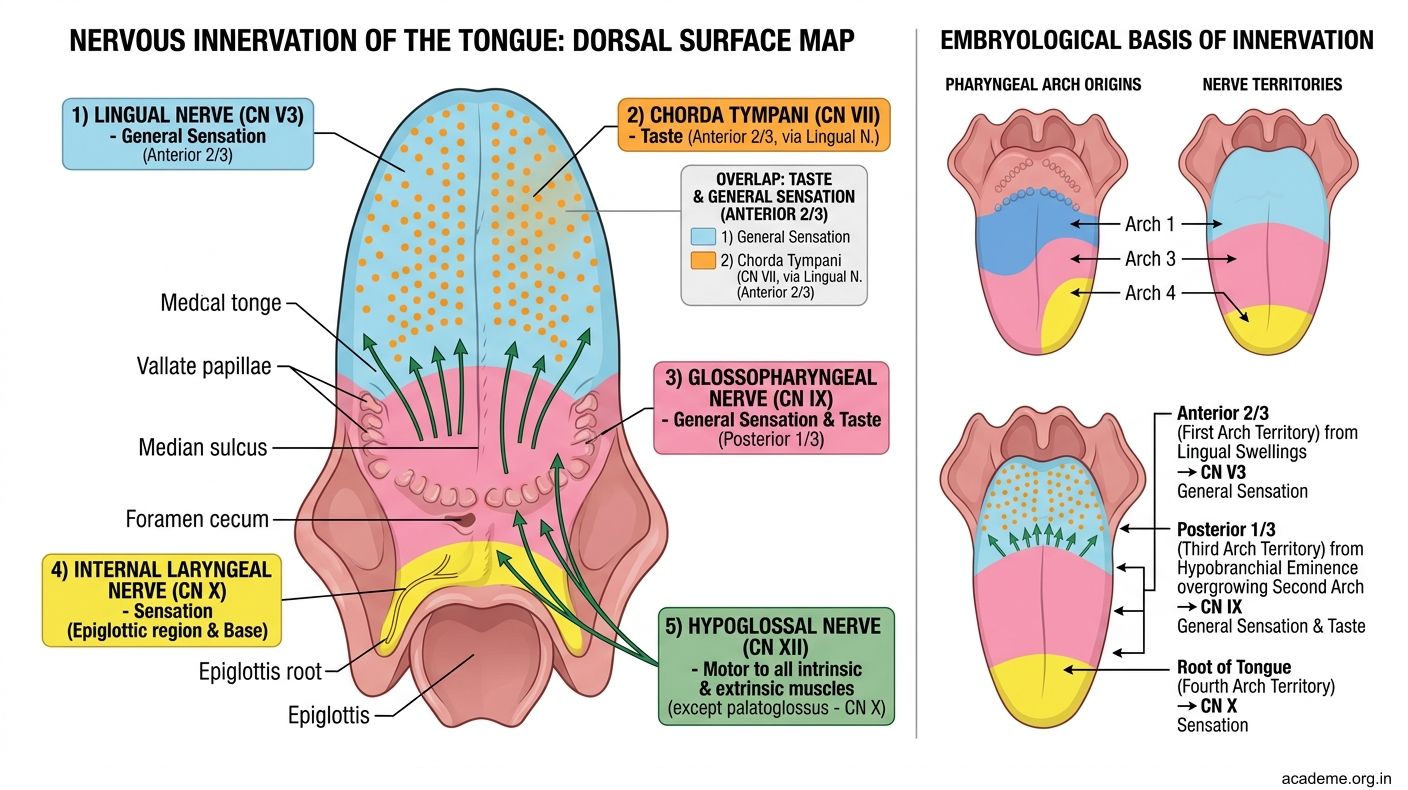
Figure: Nerve Supply of the Tongue (AN39.1)
SELF-CHECK — : Tongue Muscles and Nerve Supply
Which extrinsic tongue muscle is NOT supplied by the hypoglossal nerve?
A. Genioglossus
B. Hyoglossus
C. Palatoglossus
D. Styloglossus
Reveal Answer
Answer: C. Palatoglossus
A patient has loss of taste sensation on the right anterior 2/3 of the tongue but intact general sensation. Which nerve is most likely injured?
A. Right lingual nerve (CN V3)
B. Right chorda tympani (CN VII)
C. Right glossopharyngeal nerve (CN IX)
D. Right hypoglossal nerve (CN XII)
Reveal Answer
Answer: B. Right chorda tympani (CN VII)
The sulcus terminalis marks the boundary between anterior 2/3 and posterior 1/3 of the tongue. The foramen caecum at its apex represents the origin of which structure?
A. Lingual tonsil
B. Thyroglossal duct
C. Chorda tympani
D. Lingual frenulum
Reveal Answer
Answer: B. Thyroglossal duct
Part 3: Hypoglossal Nerve Palsy — Anatomical Basis (AN39.2)
Course of the Hypoglossal Nerve (CN XII)

Figure: Key Takeaways — Tongue (AN39.1-2)

Figure: The Lingual Nerve and its Relation to the Third Molar
The hypoglossal nerve:
1. Emerges from the hypoglossal canal (anterior condylar canal) in the occipital bone
2. Exits the skull and loops forward between the internal carotid artery and internal jugular vein
3. Hooks around the occipital artery
4. Passes deep to the digastric (posterior belly) and stylohyoid muscles
5. Runs on the lateral surface of hyoglossus
6. Passes superficial to the lingual artery (separated by hyoglossus)
7. Enters the tongue between genioglossus and mylohyoid
The C1 fibres: The hypoglossal nerve is "hitched" by fibres from the C1 spinal nerve as it loops around the carotid artery. These C1 fibres continue as the superior root of the ansa cervicalis (descending hypoglossi) — they supply the infrahyoid strap muscles (except thyrohyoid which is supplied by C1 only). These are NOT true CN XII fibres.
Clinical Features of Hypoglossal Nerve Palsy (AN39.2)
| Feature | Explanation |
|---|---|
| Tongue deviation to the affected side on protrusion | Genioglossus of the HEALTHY side protrudes its half of the tongue forward; the paralysed side lags behind, pushing the tongue toward the weak side |
| Ipsilateral wasting | Atrophy of tongue on the side of CN XII lesion (visible as hollowing or wrinkling of hemitongue) |
| Dysarthria | Difficulty with lingual consonants (L, N, T, D) |
| Dysphagia | Impaired bolus propulsion |
Memory aid for tongue deviation: "The tongue FALLS TOWARD the weak side" (like a tree falling toward the side the wood was cut).
Causes of hypoglossal nerve palsy in Indian clinical practice:
• Nasopharyngeal carcinoma — invades skull base at the hypoglossal canal (most common in South and Southeast Asian populations)
• Carotid endarterectomy / carotid artery surgery — nerve injury during dissection in the carotid triangle
• Neck dissection for oral/oropharyngeal malignancy — the nerve lies in the operative field
• Posterior fossa tumours (jugular foramen tumours involve CN IX, X, XI; hypoglossal canal tumours involve XII separately)
• Lateral medullary syndrome (Wallenberg) — central lesion; tongue deviation toward the contralateral side (the nucleus is injured, not the nerve)
• Penetrating neck injuries — common in road traffic accidents

Figure: Part 3: Hypoglossal Nerve Palsy — Anatomical Basis (AN39.2)
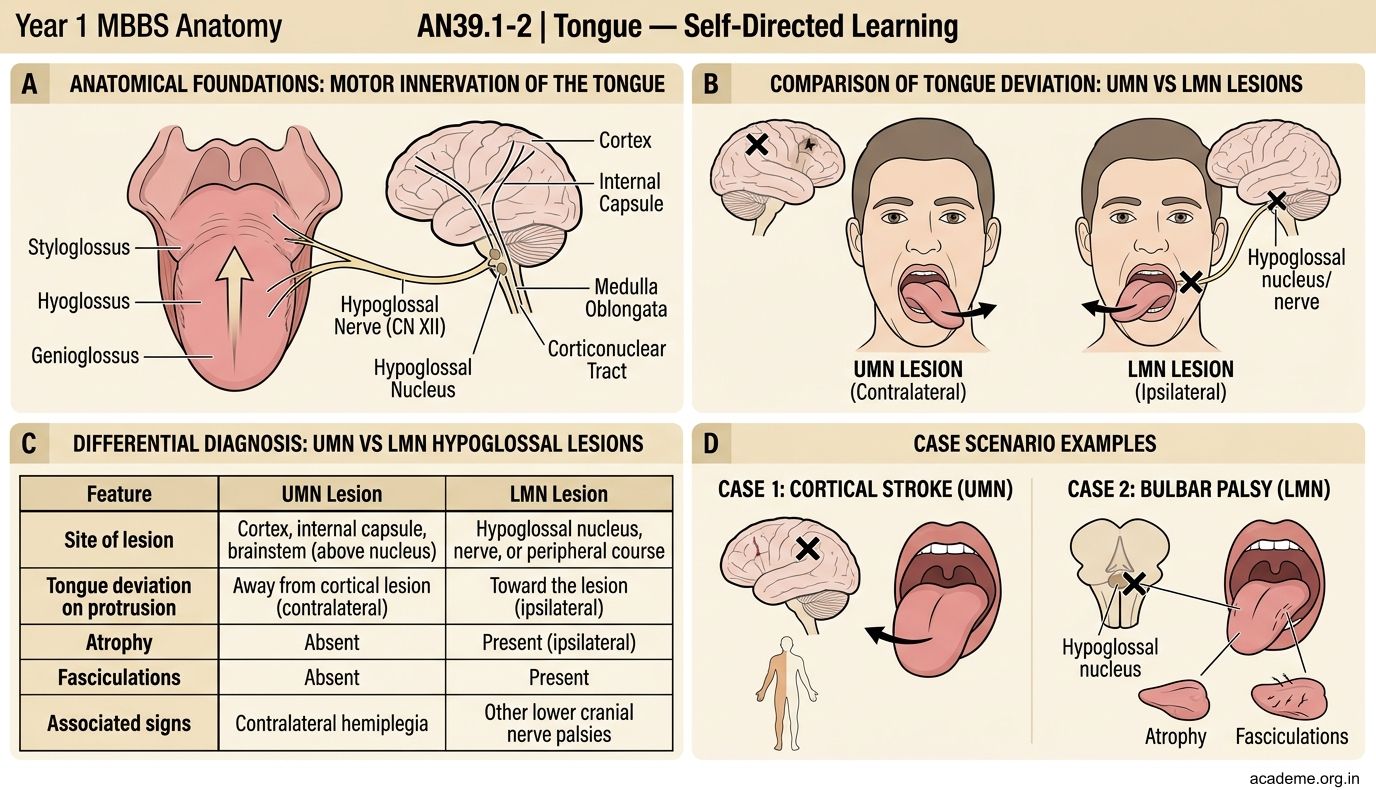
Figure: Part 3: Hypoglossal Nerve Palsy — Anatomical Basis (AN39.2)
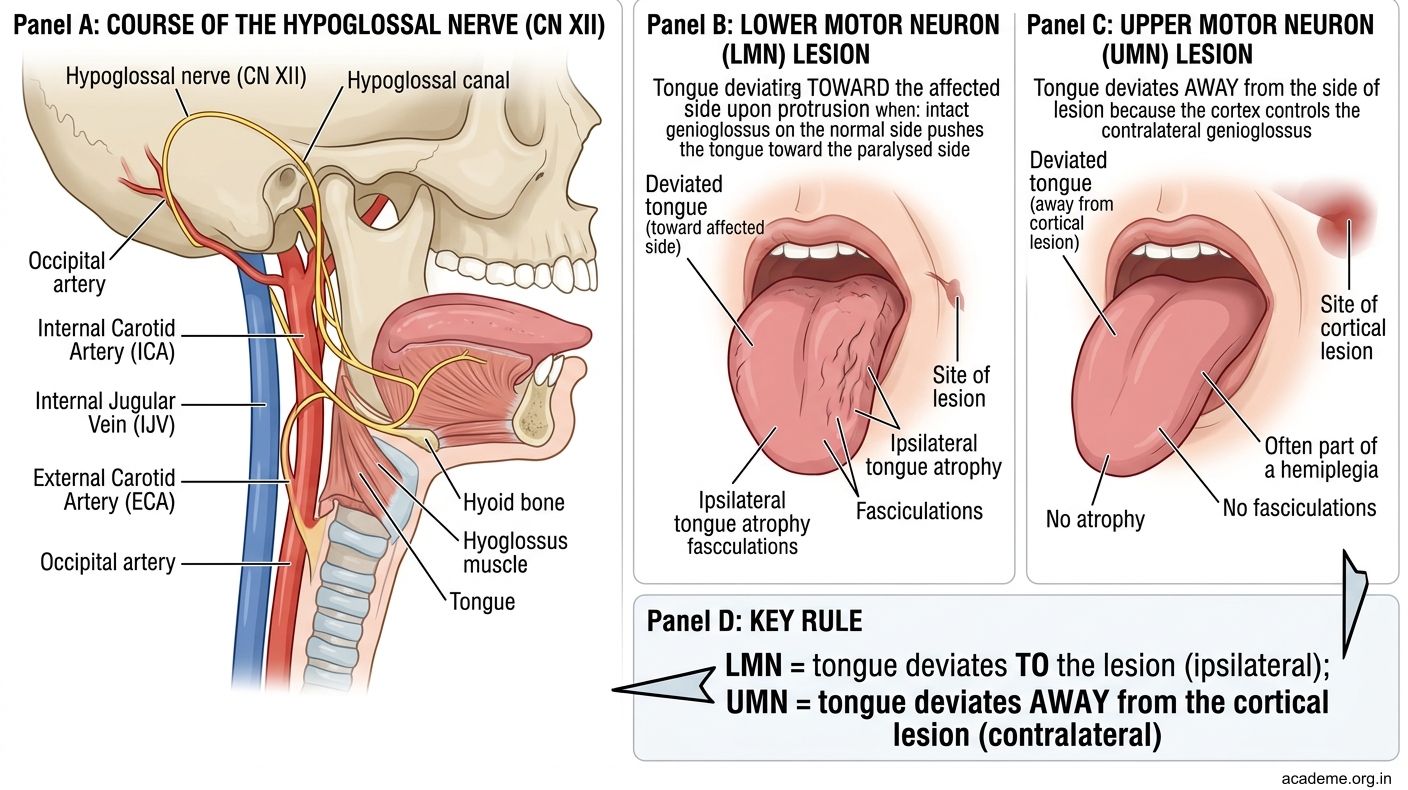
Figure: Part 3: Hypoglossal Nerve Palsy — Anatomical Basis (AN39.2)

Figure: Clinical Features of Hypoglossal Nerve Palsy (AN39.2)
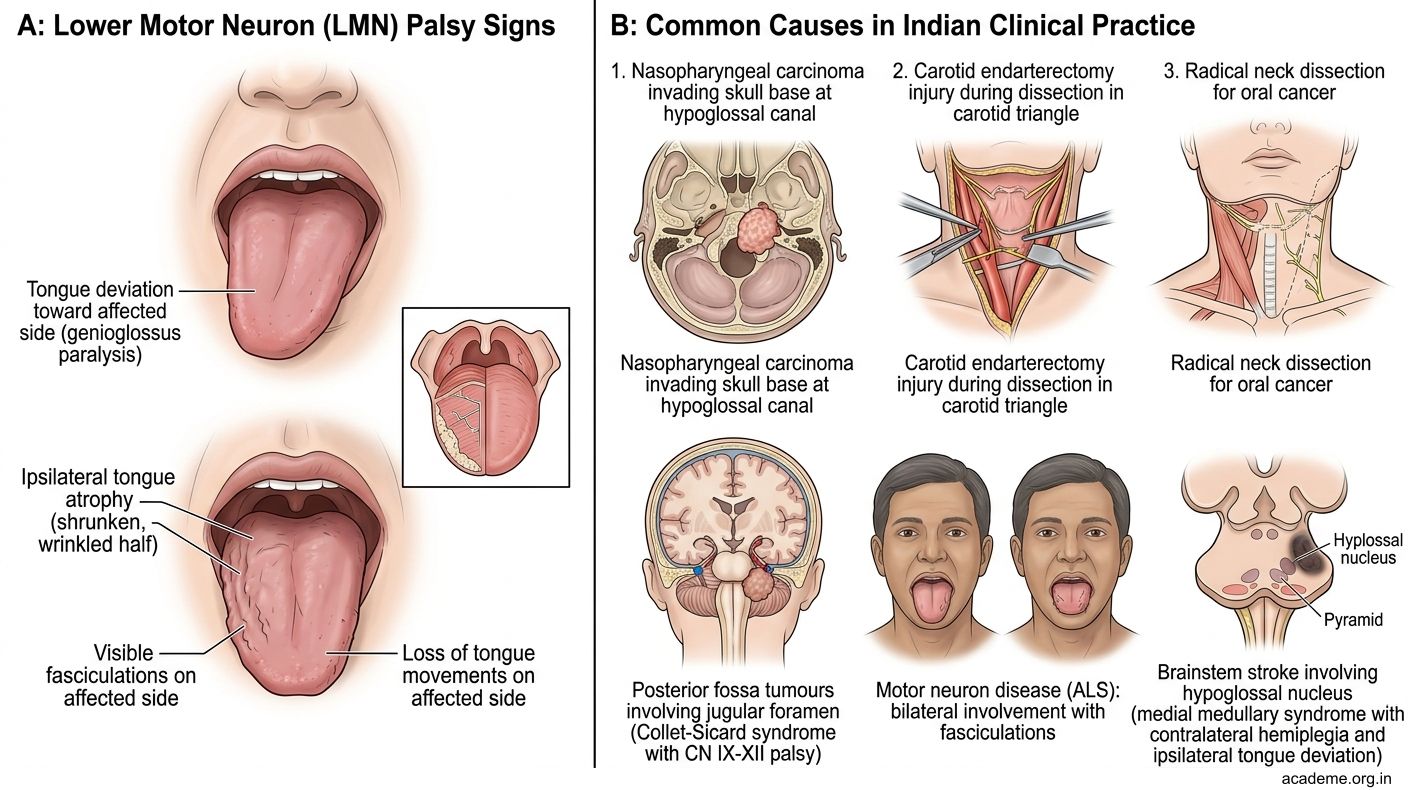
Figure: Clinical Features of Hypoglossal Nerve Palsy (AN39.2)
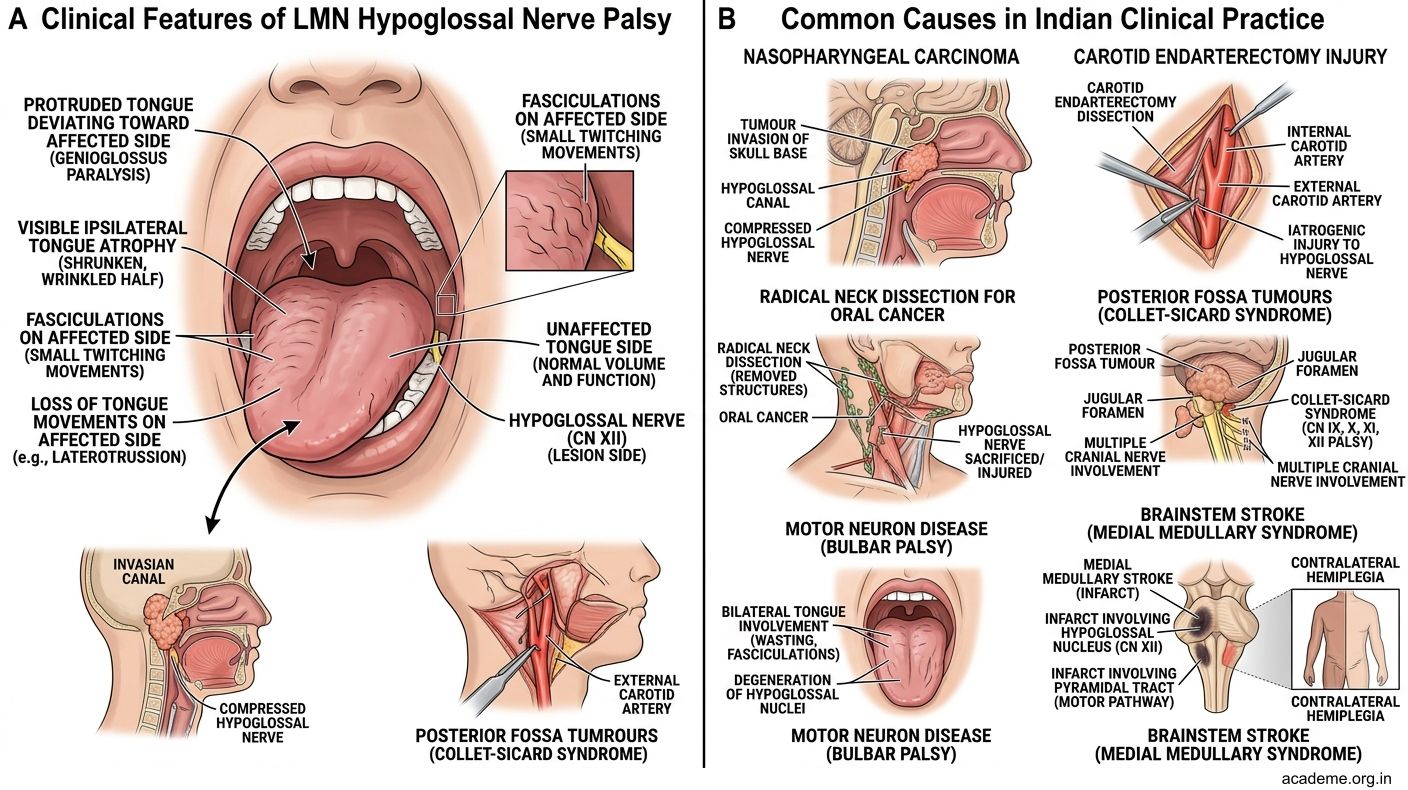
Figure: Clinical Features of Hypoglossal Nerve Palsy (AN39.2)
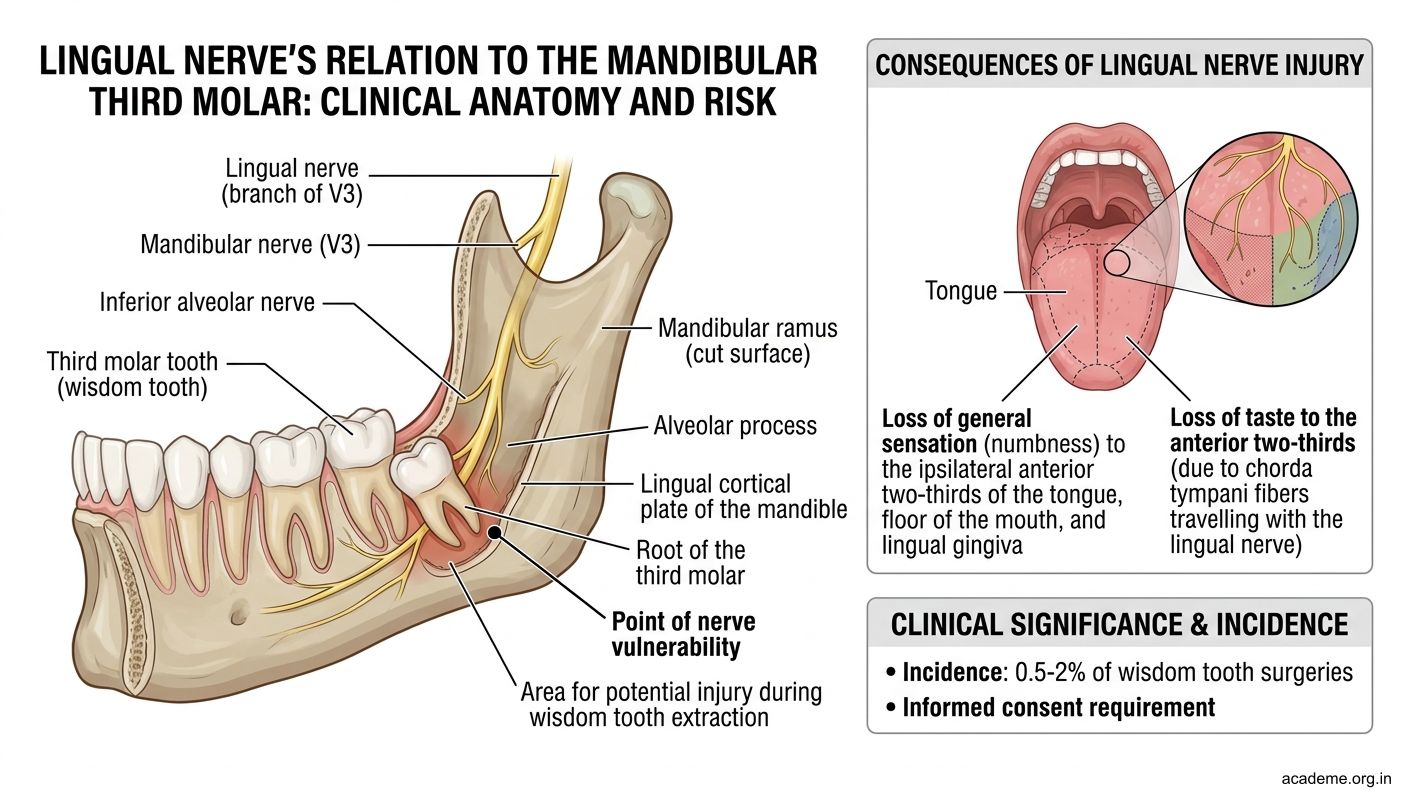
Figure: The Lingual Nerve and its Relation to the Third Molar
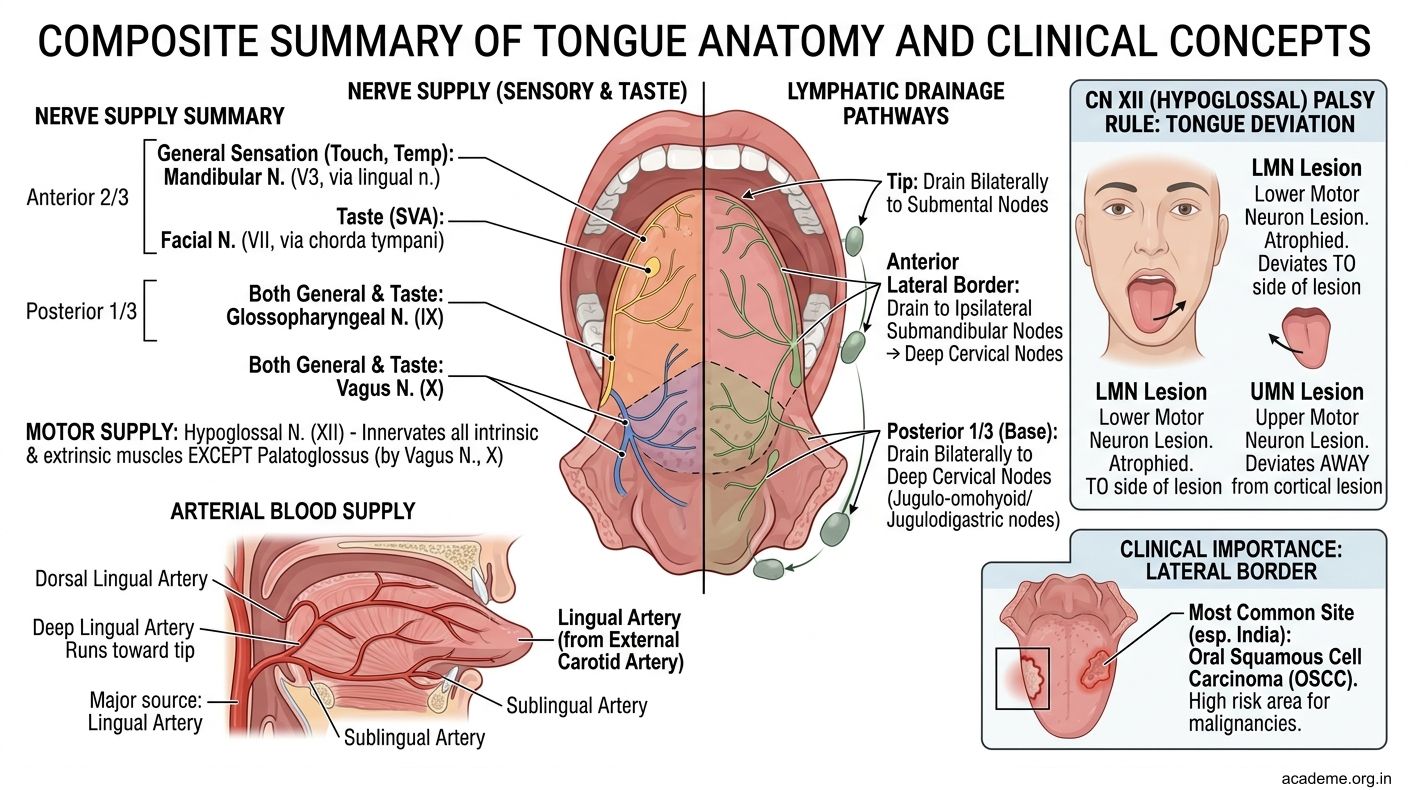
Figure: Key Takeaways — Tongue (AN39.1-2)
CLINICAL PEARL
The Lingual Nerve and its Relation to the Third Molar
The lingual nerve runs on the medial side of the mandible, immediately below the mucosa of the floor of mouth, in close proximity to the roots of the lower third molar (wisdom tooth). During surgical extraction of an impacted lower third molar, the lingual nerve is at risk of injury — resulting in loss of general sensation to the ipsilateral anterior 2/3 of the tongue and the floor of the mouth.
In Indian dental and maxillofacial practice, this is a well-known complication of wisdom tooth surgery. The incidence is estimated at 0.5–2%. Always inform patients of this risk during consent.
Additionally, the chorda tympani (taste fibres for anterior 2/3) joins the lingual nerve in the infratemporal fossa. Injury to the lingual nerve proximal to this junction also abolishes taste — creating the combination of lost general sensation + lost taste on the anterior 2/3.
REFLECT
Return to the hook case — the 55-year-old beedi-maker with a painless ulcer on the lateral tongue border and tongue deviation to the left on protrusion, with reduced anterior 2/3 sensation on the left.
- The tongue deviation to the left indicates CN XII palsy on which side? What is the anatomical explanation?
- The reduced sensation on the anterior 2/3 left indicates which nerve is affected and at what level?
- Could these two findings (CN XII palsy + lingual nerve deficit) be caused by a single lesion? Where would that lesion be?
- What is the significance of the painless lateral tongue ulcer in a beedi-maker from Cuddalore?
Discussion: Tongue deviation to the left = left CN XII palsy (the intact right genioglossus pushes the tongue left). Reduced anterior 2/3 left sensation = left lingual nerve injury. A single lesion at the left floor of mouth or retromolar region could compress both the lingual nerve and the hypoglossal nerve, as they run in proximity deep to hyoglossus. However, a more sinister explanation in this case is a left lateral tongue carcinoma with deep invasion — the primary tumour can invade the floor of mouth, compressing or invading both nerves. The painless nature, beedi use (tobacco without paper = highest risk for oral cancer), and lateral border site are classic for squamous cell carcinoma. This patient needs urgent biopsy and oncology referral.
KEY TAKEAWAYS
Key Takeaways — Tongue (AN39.1-2)
Muscles:
• Extrinsic (4): Genioglossus (protrudes), Hyoglossus (depresses), Styloglossus (retracts+elevates), Palatoglossus (elevates posterior tongue) — all CN XII except Palatoglossus (CN X)
• Intrinsic (4): Superior longitudinal, Inferior longitudinal, Transverse, Vertical — all CN XII
Nerve Supply:
• Anterior 2/3 — General sensory: CN V3 (lingual nerve) | Taste: CN VII (chorda tympani)
• Posterior 1/3 — General sensory + Taste: CN IX
• Base/epiglottis — CN X
• Motor all (except palatoglossus): CN XII
Blood Supply: Lingual artery (branch of external carotid) — deep lingual artery at tip
Lymphatics:
• Tip → submental nodes (bilateral risk)
• Lateral border → submandibular + ipsilateral deep cervical
• Posterior 1/3 → directly to deep cervical (bilateral)
Hypoglossal nerve palsy:
• Tongue DEVIATES to the affected (weak) side on protrusion
• Genioglossus is the key protruder — the healthy side wins
• Causes: nasopharyngeal Ca, carotid surgery, neck dissection, penetrating injuries