Page 1 of 4
AN41.1-3 | Eyeball — SDL Guide
Learning Objectives
- Describe and demonstrate the coats (layers) of the eyeball and the structure of each coat (AN41.1)
- Describe the refractive media of the eye and trace the pathway of aqueous humour from production to drainage (AN41.1)
- Explain the anatomical basis of cataract, glaucoma, and central retinal artery occlusion (AN41.2)
- Describe the position, nerve supply, and actions of intraocular muscles (AN41.3)
- Correlate eyeball anatomy with clinical conditions encountered in Indian ophthalmology practice
INSTRUCTIONS
Read the module carefully and refer to the cross-section of the eyeball in your atlas. The micro-quizzes will test your understanding of clinical applications.
References
- Gray's Anatomy for Students (Drake et al.) — Chapter 8: Orbit and Eyeball (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 3 — Head & Neck (Textbook)
- Khurana's Comprehensive Ophthalmology (Textbook)
- OpenStax Anatomy and Physiology 2e — Special Senses: Vision (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 68-year-old woman from Pondicherry presents to the eye outpatient department with gradual painless deterioration of vision in her right eye over the past year. Ophthalmoscopy reveals an absent red reflex and a grey-white opacity of the lens. Her intraocular pressure is 28 mmHg (normal: 10–21 mmHg).
What are the two diagnoses? What is the anatomical structure involved in each? How does aqueous humour drainage relate to the raised intraocular pressure?
Understanding the anatomy of the eyeball layers, refractive media, and aqueous circulation is essential to answer these questions — and to understand a large portion of Indian ophthalmology practice.
WHY THIS MATTERS
The eyeball is clinically relevant to Indian medicine in particular because:
- Cataracts account for approximately 66% of blindness in India — more than any other cause; cataract surgery (phacoemulsification) is the most common surgical procedure in ophthalmology
- Glaucoma (raised intraocular pressure) affects an estimated 12 million Indians and is the second leading cause of blindness; it is often asymptomatic until advanced
- Central retinal artery occlusion — a stroke of the eye — requires emergency management and understanding the vessel's anatomy
- Diabetic retinopathy — India has the world's second largest diabetic population; retinal changes are the most common cause of new blindness in working-age adults
- Fundoscopy (ophthalmoscopy) is a basic clinical skill taught in second year — you cannot interpret what you see without knowing retinal anatomy
RECALL
Before we begin, recall:
- The orbit is a bony pyramid formed by frontal, sphenoid, ethmoid, maxilla, zygomatic, lacrimal, and palatine bones
- The optic nerve (CN II) exits via the optic canal (sphenoid bone)
- CN III (oculomotor), CN IV (trochlear), CN VI (abducens), and CN V1 (ophthalmic) enter the orbit via the superior orbital fissure
- The ciliary ganglion in the orbit provides parasympathetic supply to the pupillary constrictor and ciliary muscle
Part 1: Coats of the Eyeball (AN41.1)
The eyeball is approximately 24 mm in diameter and consists of three concentric coats (tunics):

Figure: Part 1: Coats of the Eyeball (AN41.1)
1. Outer Fibrous Coat (Tunica Fibrosa)
Two parts:
• Sclera (posterior 5/6) — opaque, white, tough fibrous coat; provides structural support; site of attachment of extraocular muscles; the optic nerve pierces it posteriorly at the lamina cribrosa (a sieve-like area — the weakest point, site of glaucomatous cupping)
• Cornea (anterior 1/6) — transparent, avascular, highly refractive (accounts for approximately 2/3 of total refractive power); the junction with the sclera is the limbus (contains stem cells for corneal epithelial renewal); five layers: epithelium → Bowman's membrane → stroma → Descemet's membrane → endothelium
Clinical note: The cornea has the highest density of sensory nerve endings in the body (supplied by CN V1 — ophthalmic, via long ciliary nerves) — hence extreme sensitivity to foreign bodies and corneal abrasions.
2. Middle Vascular Coat (Tunica Vasculosa = Uvea)
Three parts from back to front:
• Choroid — posterior 2/3; highly vascular layer between sclera and retina; nourishes the outer layers of the retina; pigmented (black) to prevent internal reflection; choriocapillaris = dense capillary network
• Ciliary body — annular thickening at the junction of choroid and iris; contains the ciliary muscle (smooth muscle for accommodation — changes lens shape; innervated by CN III parasympathetic via ciliary ganglion); connected to the lens by zonular fibres (suspensory ligament of lens); secretes aqueous humour via ciliary processes
• Iris — thin, pigmented, muscular diaphragm with the pupil at its centre; contains:
- Sphincter pupillae (circular) — constricts pupil (miosis); parasympathetic (CN III via ciliary ganglion)
- Dilator pupillae (radial) — dilates pupil (mydriasis); sympathetic (long ciliary nerve from superior cervical ganglion via nasociliary nerve)
3. Inner Neural Coat (Retina)
Two layers:
• Outer pigmented layer (RPE) — single layer of pigmented cells attached to choroid; does NOT detach in retinal detachment
• Inner neural/sensory layer — contains photoreceptors (rods for scotopic/dim-light vision; cones for photopic/colour vision)
Key regions of the retina:
• Macula lutea — lateral to optic disc; the region of highest cone density; responsible for central detailed vision; has a central depression — the fovea centralis (purest cone region, no rods, no overlying cells → highest visual acuity)
• Optic disc (blind spot) — medial to macula; where optic nerve fibres exit; NO photoreceptors → physiological blind spot; the lamina cribrosa of the sclera supports it
Chambers of the Eyeball
| Chamber | Location | Contents |
|---|---|---|
| Anterior chamber | Between cornea and iris | Aqueous humour |
| Posterior chamber | Between iris and lens | Aqueous humour |
| Vitreous chamber | Behind lens | Vitreous body (gel-like, not regenerated) |
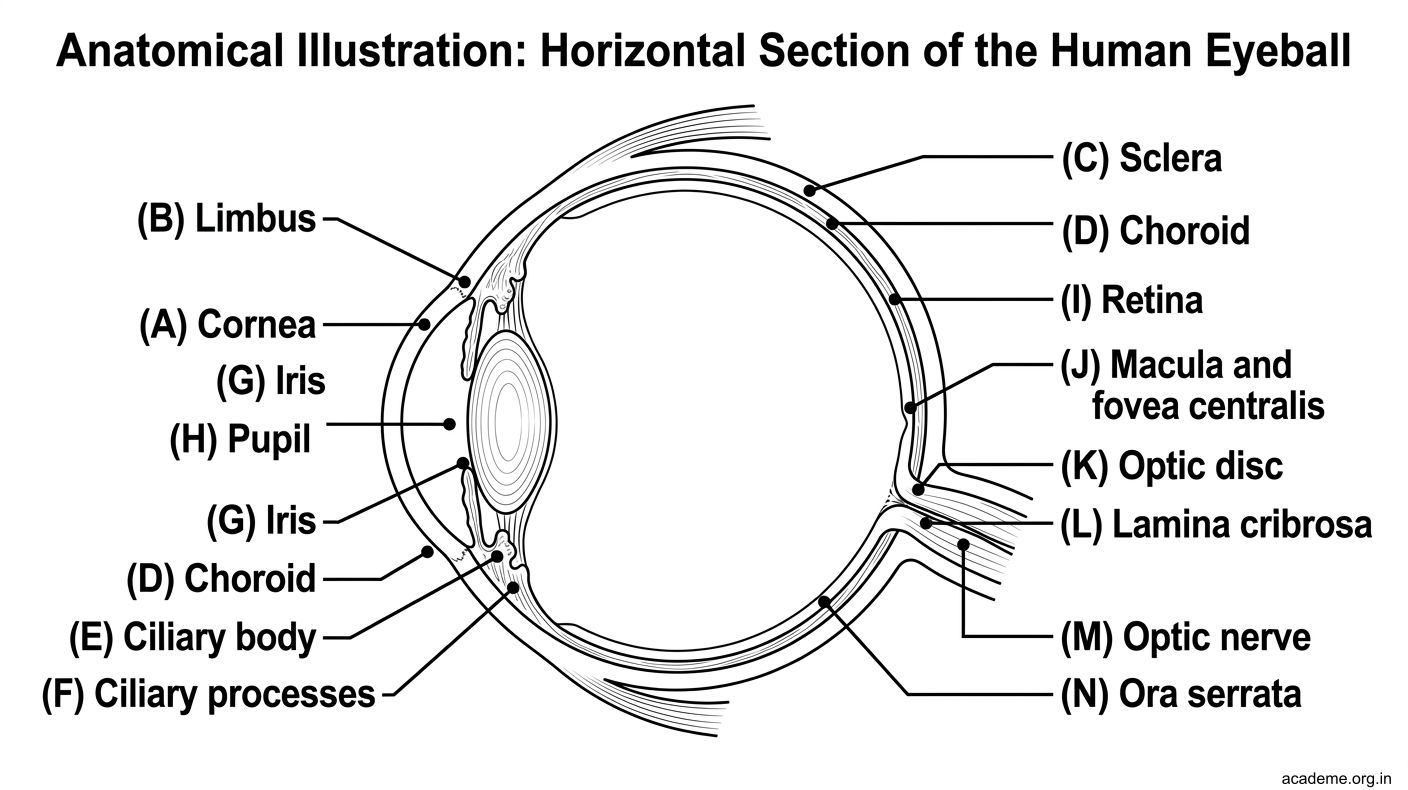
Figure: Part 1: Coats of the Eyeball (AN41.1)
Part 2: Refractive Media, Aqueous Humour, and Glaucoma (AN41.1, AN41.2)
Refractive Media

Figure: Central Retinal Artery Occlusion (CRAO) — Anatomical Basis (AN41.2)

Figure: Cataract — Anatomical Basis (AN41.2)

Figure: Glaucoma — Anatomical Basis (AN41.2)

Figure: Aqueous Humour — Production and Drainage

Figure: Part 2: Refractive Media, Aqueous Humour, and Glaucoma (AN41.1, AN41.2)
Light passes through four refractive media before reaching the retina:
1. Cornea — greatest refractive power (~43 dioptres); fixed; avascular; nourished by aqueous humour and tear film; responsible for most refractive errors when its shape is abnormal (astigmatism)
2. Aqueous humour — fills anterior and posterior chambers; refractive index similar to water
3. Lens — biconvex crystalline structure; approximately 9–10 dioptres (variable with accommodation); suspended by zonular fibres from the ciliary body; lacks blood vessels and nerves; nourished by aqueous humour; composed of lens fibres (elongated transparent cells, no nuclei) arranged in concentric layers around the nucleus
4. Vitreous body — gel filling the vitreous chamber (99% water + hyaluronic acid + collagen fibrils); maintains eyeball shape; not regenerated if lost (as in penetrating trauma)
Aqueous Humour — Production and Drainage
Production:
• Secreted by the non-pigmented epithelium of the ciliary processes (in the ciliary body) by active secretion + ultrafiltration
• Flows from the posterior chamber → through the pupil → into the anterior chamber
Drainage (trabecular pathway — 90%):
• From the anterior chamber angle (iridocorneal angle/irido-corneal angle) → trabecular meshwork (spongy tissue at the limbus) → Canal of Schlemm (circular venous sinus at the limbus) → aqueous veins → episcleral veins → venous system
Uveoscleral drainage (10%):
• Across the ciliary body stroma into the suprachoroidal space → out through the sclera
Glaucoma — Anatomical Basis (AN41.2)
Glaucoma = raised intraocular pressure (>21 mmHg) damaging the optic nerve at the lamina cribrosa (the weakest point in the sclera where nerve fibres exit).
Types:
• Open-angle glaucoma (chronic) — the iridocorneal angle is open but the trabecular meshwork is dysfunctional; aqueous outflow is reduced; slow progressive optic nerve damage; painless and asymptomatic until late; most common type
• Closed-angle glaucoma (acute) — the iris physically occludes the iridocorneal angle, blocking drainage; causes sudden elevation of IOP → red eye, severe headache, halos around lights, nausea; ophthalmic emergency
Optic disc changes in glaucoma: increased cup-to-disc ratio (cupping of optic disc due to atrophy at the lamina cribrosa), nasal shift of blood vessels, flame-shaped haemorrhages.
Cataract — Anatomical Basis (AN41.2)
Cataract = opacity of the lens or its capsule, causing visual loss.
Why the lens becomes opaque:
The lens has no blood supply — it depends entirely on aqueous humour diffusion for nutrition. When lens fibres degenerate (due to aging, diabetes, radiation, trauma, congenital infections), they lose transparency.
Types:
• Nuclear cataract — affects the central lens nucleus; causes index myopia (patients initially read better without glasses), then progressive blurring
• Cortical cataract — affects the peripheral lens cortex; spoke-like opacities on slit-lamp
• Posterior subcapsular cataract — posterior capsule; affects near vision early; common in steroid use and diabetes
Surgical anatomy: In phacoemulsification, the anterior lens capsule is opened (continuous curvilinear capsulotomy), the lens nucleus is emulsified and removed through a 2–3 mm corneal incision, and an intraocular lens is implanted within the remaining capsule bag.
Central Retinal Artery Occlusion (CRAO) — Anatomical Basis (AN41.2)
The central retinal artery (branch of ophthalmic artery, from internal carotid) enters the optic nerve 1 cm behind the eyeball, travels within the optic nerve sheath, and enters the eye at the optic disc. It is a functional end-artery — no anastomoses within the retina.
In CRAO: Sudden, painless, monocular loss of vision ("curtain falling"). The entire inner retinal layers lose blood supply (outer layers supplied by choroid via diffusion — survives).
Fundoscopic findings:
• Pale, milky retina (oedema of infarcted inner layers)
• Cherry-red spot at the macula — the fovea is thin enough that the choroidal circulation (behind it) shows through → appears red against the white surrounding oedema

Figure: Chambers of the Eyeball
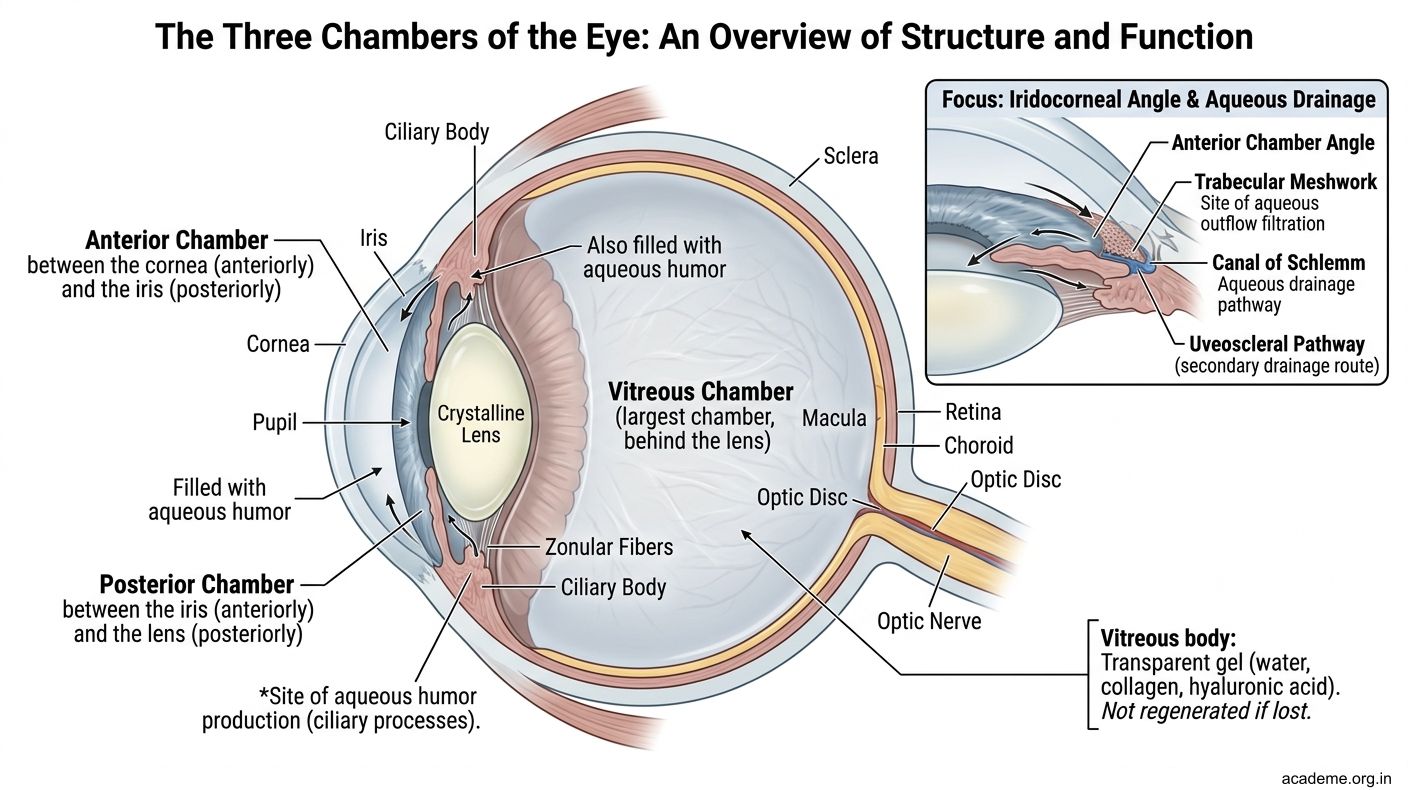
Figure: Chambers of the Eyeball
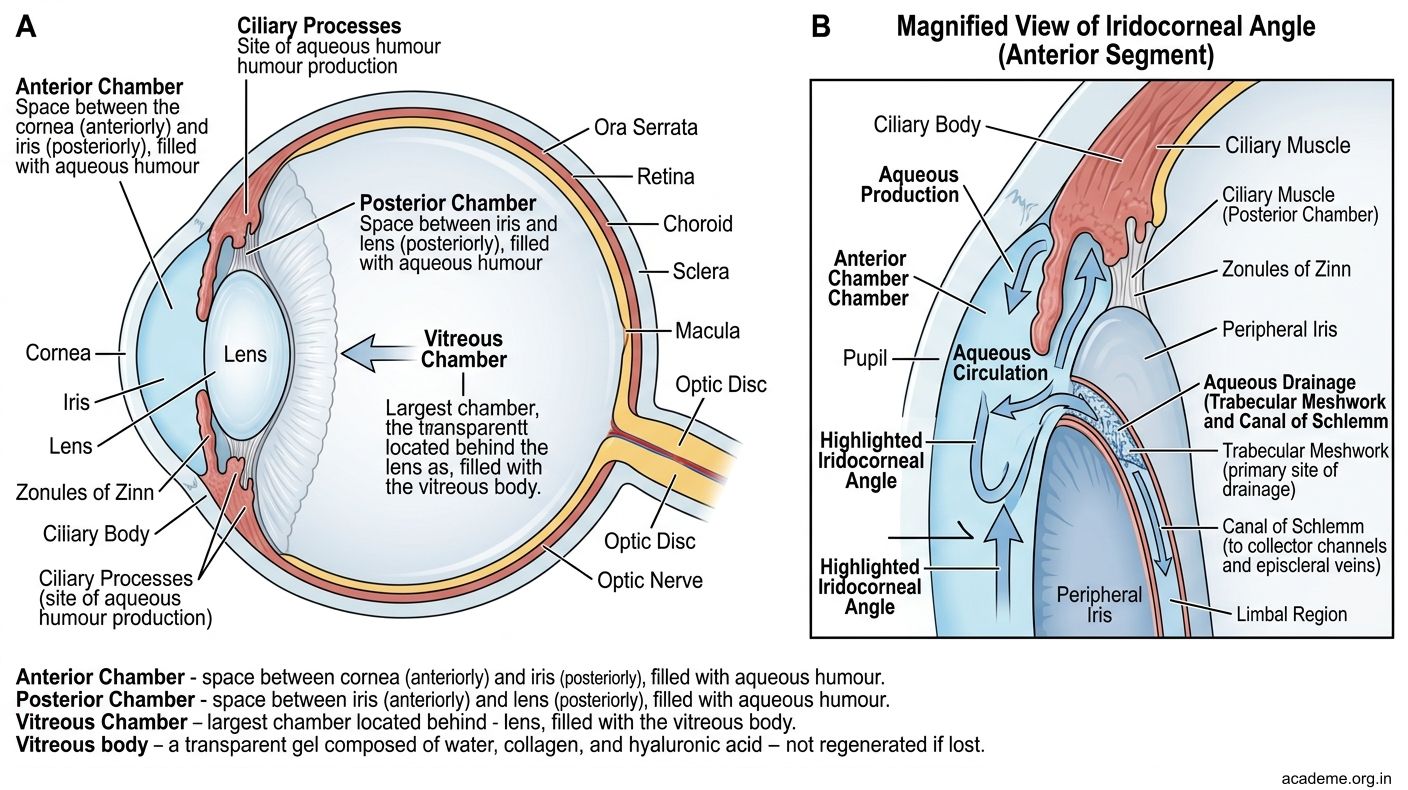
Figure: Chambers of the Eyeball
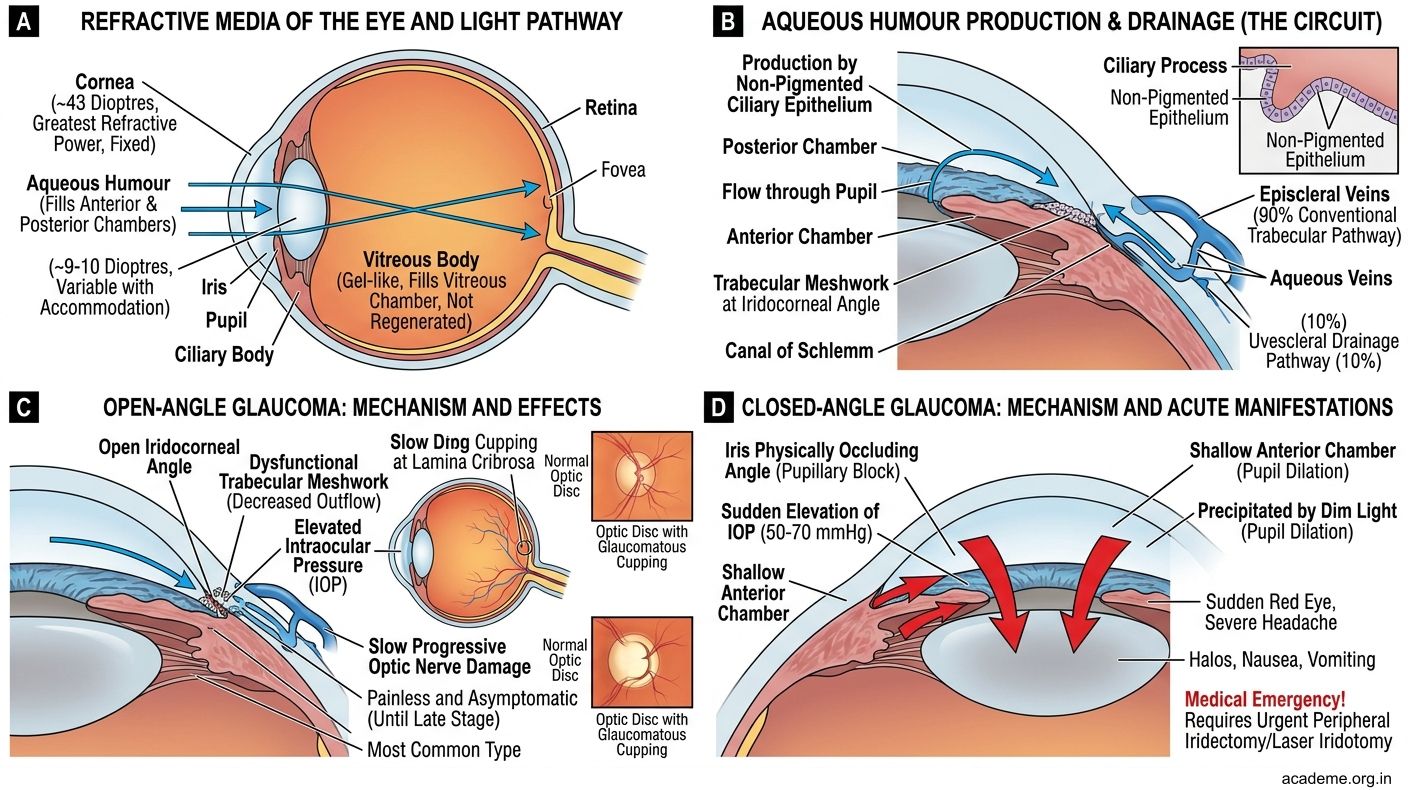
Figure: Part 2: Refractive Media, Aqueous Humour, and Glaucoma (AN41.1, AN41.2)
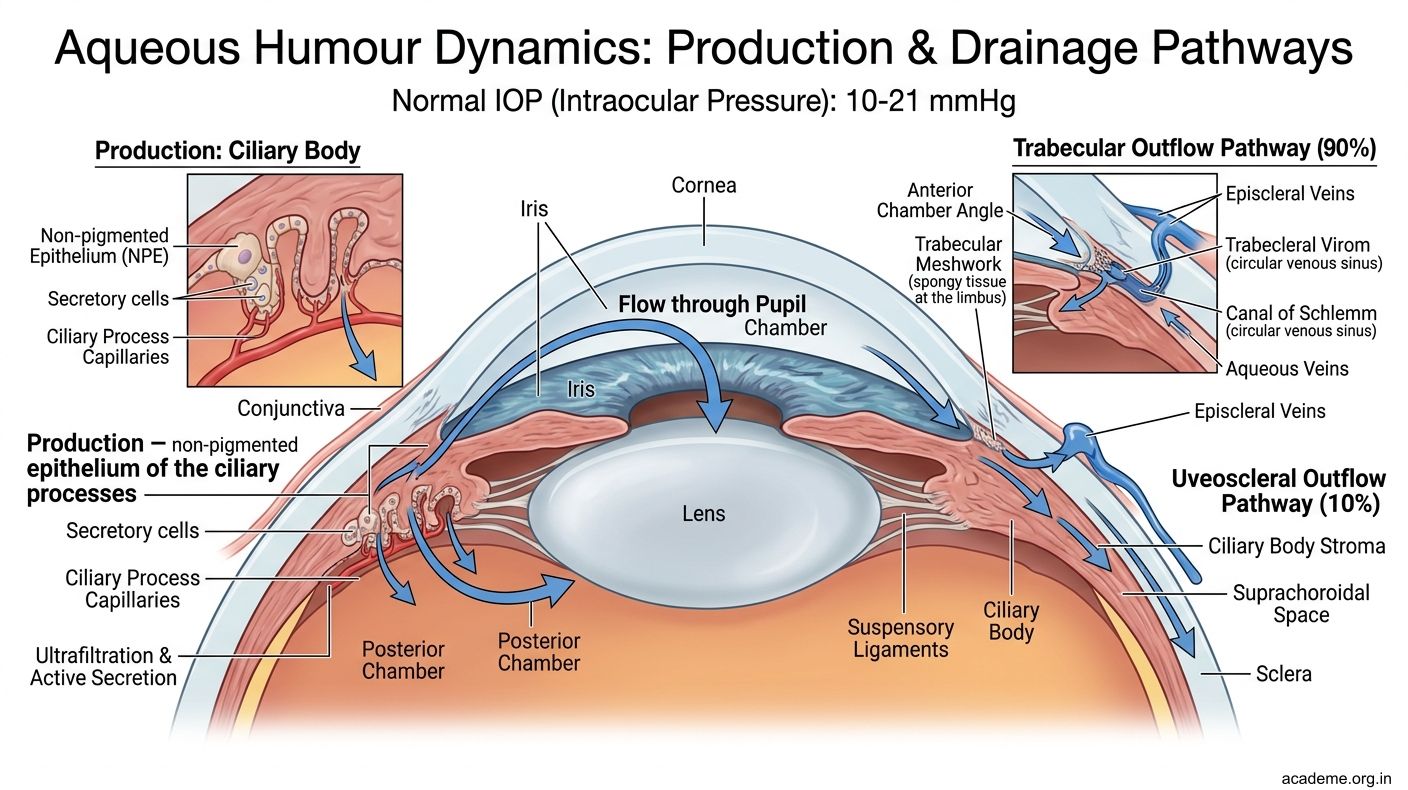
Figure: Aqueous Humour — Production and Drainage
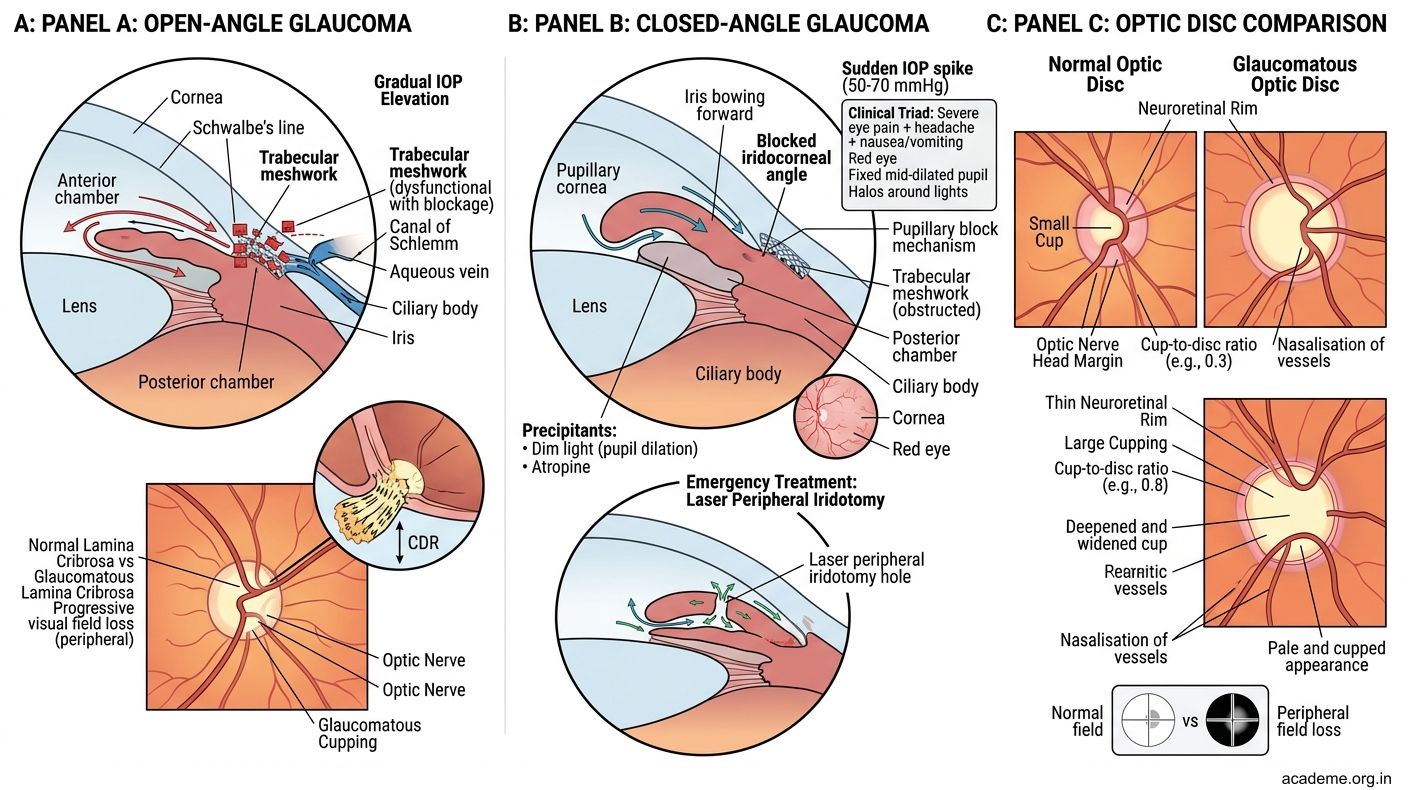
Figure: Glaucoma — Anatomical Basis (AN41.2)
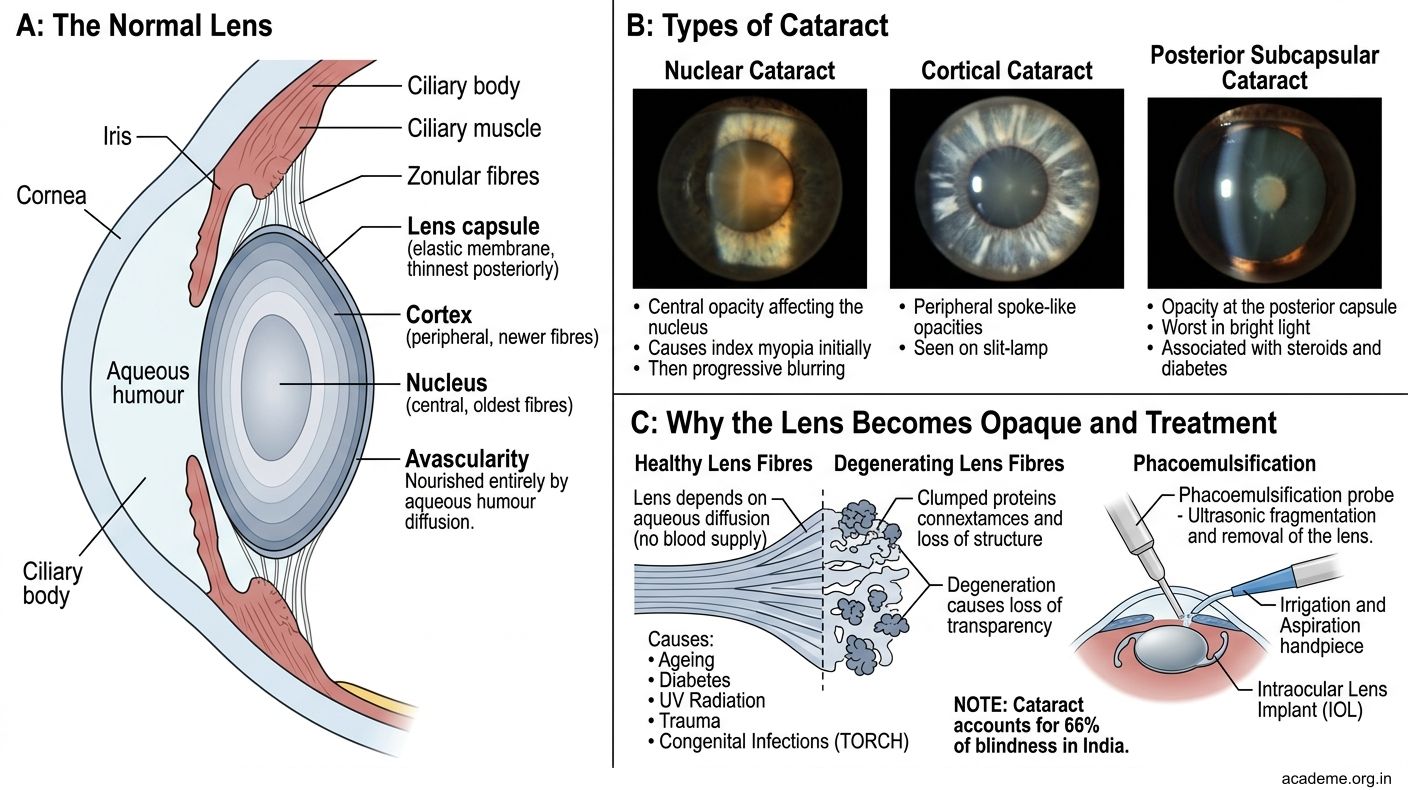
Figure: Cataract — Anatomical Basis (AN41.2)
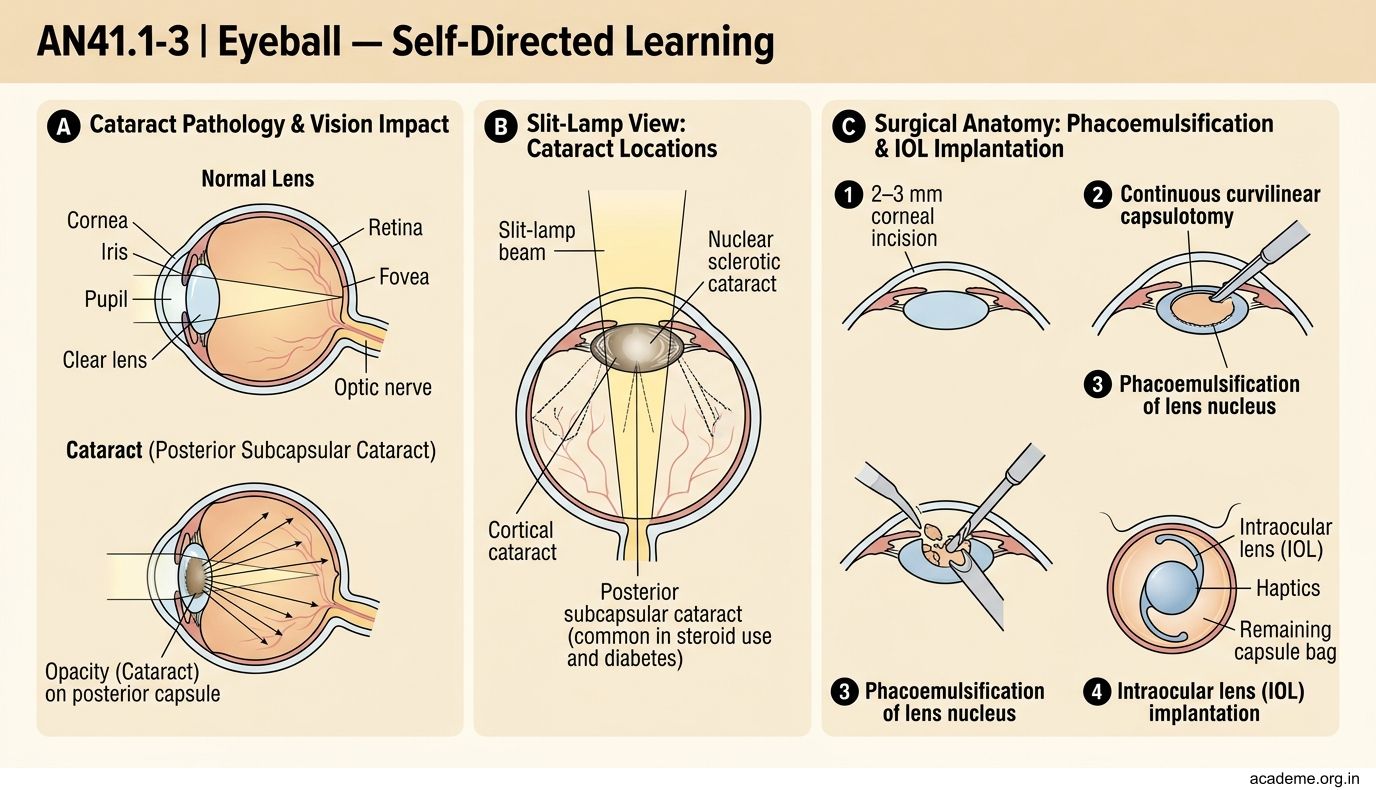
Figure: Central Retinal Artery Occlusion (CRAO) — Anatomical Basis (AN41.2)
SELF-CHECK — : Eyeball Coats and Refractive Media
Aqueous humour is produced by the ciliary processes and drains primarily via which structure?
A. Vitreous body
B. Canal of Schlemm and trabecular meshwork at the iridocorneal angle
C. Posterior ciliary arteries
D. Central retinal vein
Reveal Answer
Answer: B. Canal of Schlemm and trabecular meshwork at the iridocorneal angle
The central retinal artery is a functional end-artery. In central retinal artery occlusion, the fovea shows a "cherry-red spot" because:
A. The fovea has the highest cone density and retains circulation
B. The thin fovea allows the underlying choroidal circulation to be visible against the surrounding white infarcted retina
C. The cherry-red colour is due to haemorrhage at the fovea
D. The fovea has separate collateral supply from the posterior ciliary arteries
Reveal Answer
Answer: B. The thin fovea allows the underlying choroidal circulation to be visible against the surrounding white infarcted retina
Part 3: Intraocular Muscles — Position, Nerve Supply, and Actions (AN41.3)
Intraocular Muscles

Figure: Key Takeaways — Eyeball (AN41.1-3)

Figure: Acute Angle-Closure Glaucoma — A Medical Emergency

Figure: Pupillary Light Reflex Pathway (Summary)
There are two intraocular muscles — smooth muscles contained within the eyeball itself (distinct from the seven extraocular skeletal muscles):
1. Sphincter Pupillae
• Circular smooth muscle fibres arranged concentrically around the pupil margin
• Located in the iris
• Action: Constricts the pupil (miosis)
• Nerve supply: Parasympathetic — preganglionic fibres from the Edinger-Westphal nucleus (CN III) → ciliary ganglion → short ciliary nerves → sphincter pupillae
• Clinical: In CN III palsy, parasympathetic fibres are compressed first (they run on the outside of the nerve trunk) → fixed dilated pupil (mydriasis)
2. Dilator Pupillae
• Radially arranged smooth muscle fibres in the iris (like spokes of a wheel)
• Action: Dilates the pupil (mydriasis)
• Nerve supply: Sympathetic — postganglionic fibres from the superior cervical ganglion → internal carotid plexus → ophthalmic artery → long ciliary nerves → dilator pupillae
• Clinical: Horner's syndrome (sympathetic chain lesion) → loss of dilator pupillae + Müller's muscle in upper lid → miosis + mild ptosis (partial)
3. Ciliary Muscle
• Ring of smooth muscle in the ciliary body
• Action: Accommodation — when it contracts, the zonular fibres relax → the lens becomes more convex (increasing refractive power) → near vision
• When it relaxes, zonular fibres become taut → lens flattens → far vision
• Nerve supply: Parasympathetic — same pathway as sphincter pupillae (CN III → ciliary ganglion → short ciliary nerves)
• Clinical: Cycloplegia (paralysis of accommodation) is produced by atropine (muscarinic antagonist), which blocks both sphincter pupillae (causing dilation) and ciliary muscle (preventing accommodation) — used for fundoscopy and refraction testing
Pupillary Light Reflex Pathway (Summary)
Afferent: Retina → optic nerve → optic tract → pretectal nucleus (midbrain)
Efferent: Edinger-Westphal nucleus (CN III) → oculomotor nerve → ciliary ganglion → short ciliary nerves → sphincter pupillae
Direct response: light in one eye → that pupil constricts
Consensual response: light in one eye → both pupils constrict (decussation at pretectal nucleus to both Edinger-Westphal nuclei)
| Condition | Afferent pupil defect | Efferent defect |
|---|---|---|
| Optic nerve lesion (left) | Left RAPD — swinging torch shows left pupil dilates | — |
| CN III palsy (left) | — | Left pupil fixed and dilated, doesn't respond to direct or consensual |
| Horner's (left sympathetic) | — | Left pupil constricted (miosis), partial ptosis |

Figure: Part 3: Intraocular Muscles — Position, Nerve Supply, and Actions (AN41.3)
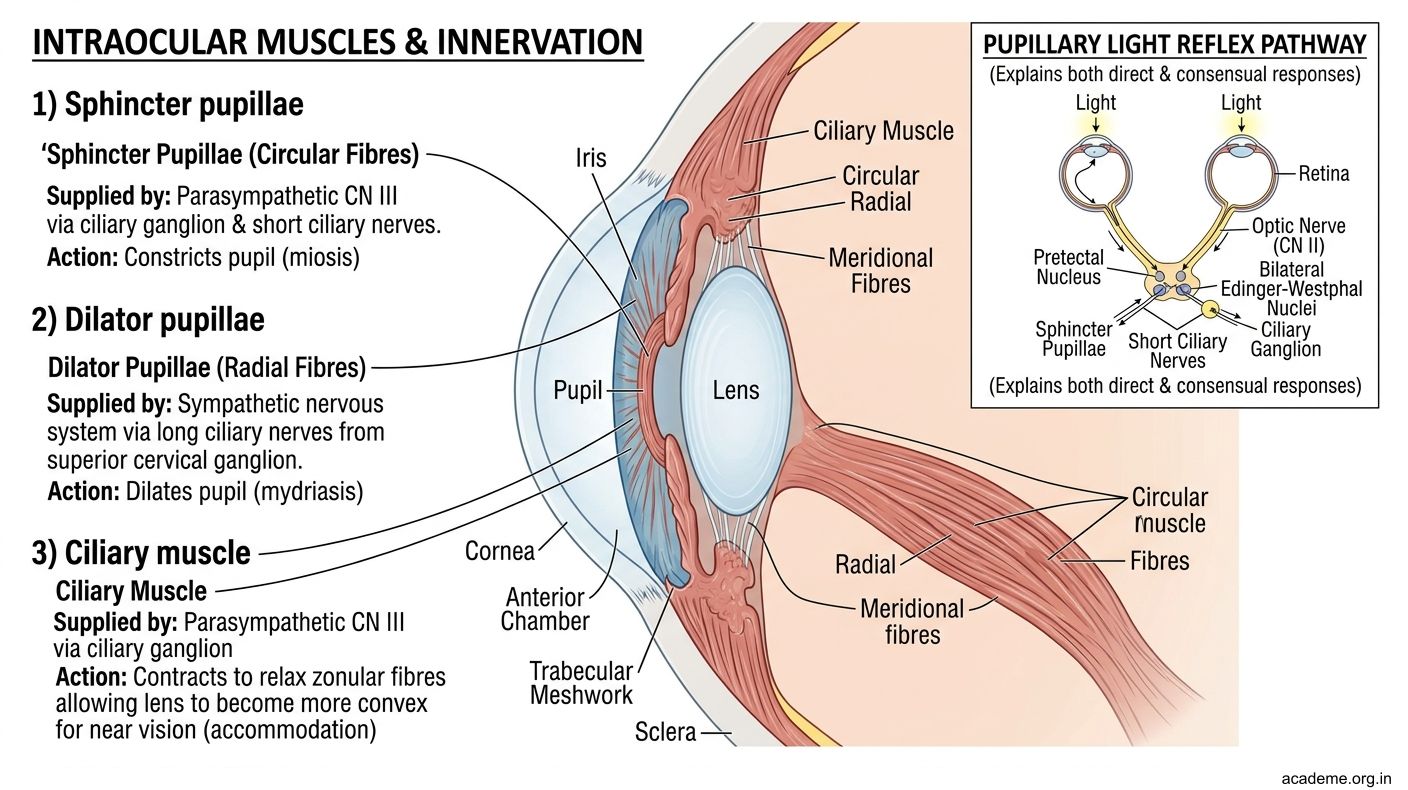
Figure: Part 3: Intraocular Muscles — Position, Nerve Supply, and Actions (AN41.3)
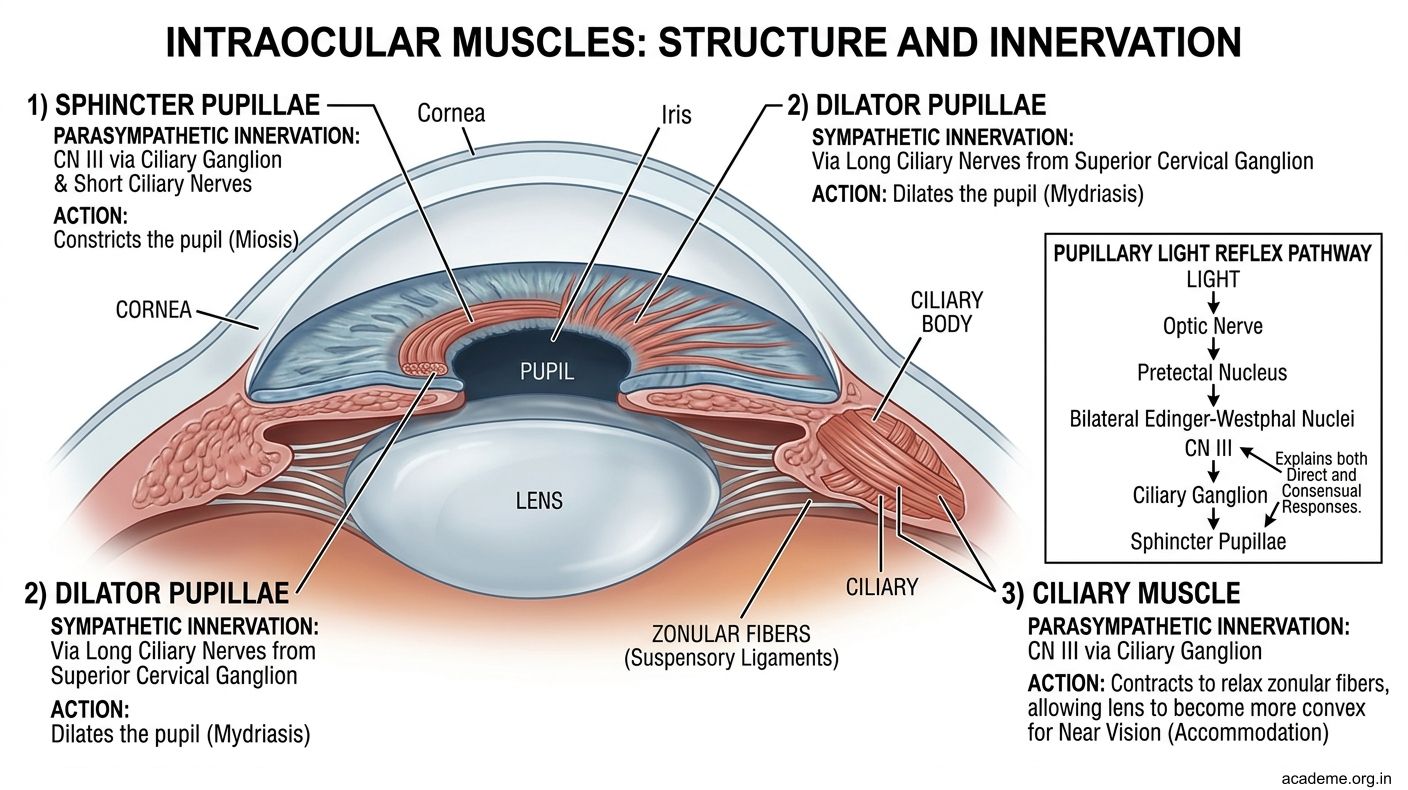
Figure: Part 3: Intraocular Muscles — Position, Nerve Supply, and Actions (AN41.3)
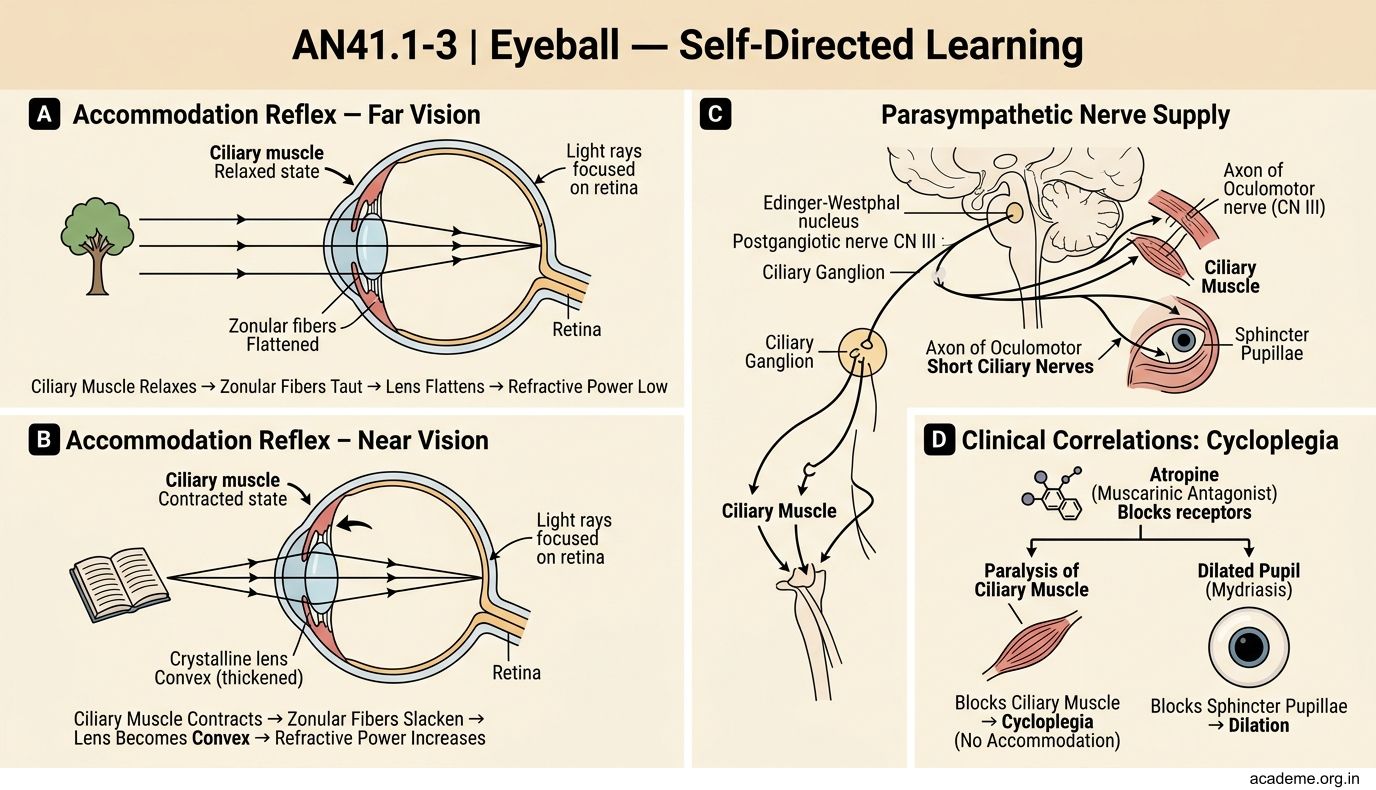
Figure: Pupillary Light Reflex Pathway (Summary)
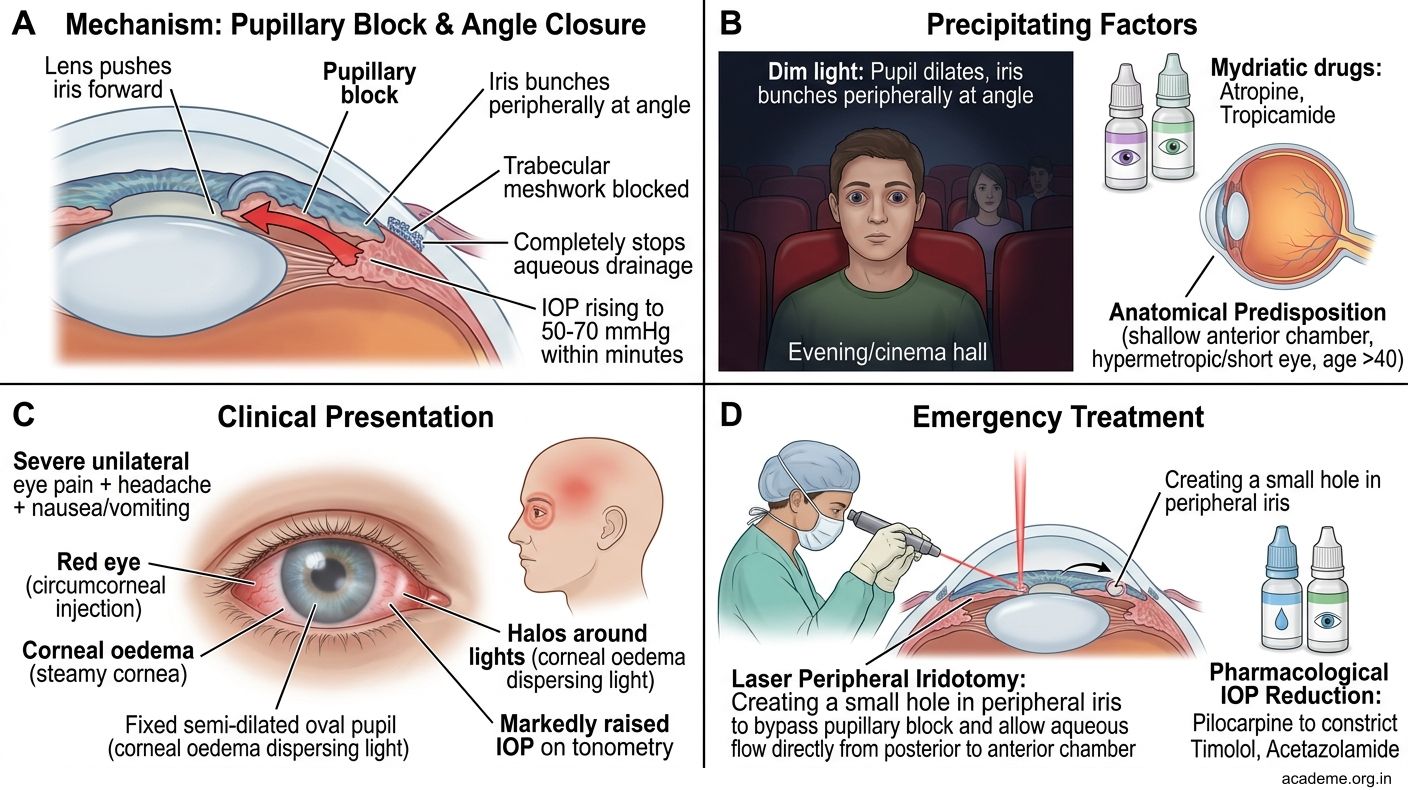
Figure: Acute Angle-Closure Glaucoma — A Medical Emergency
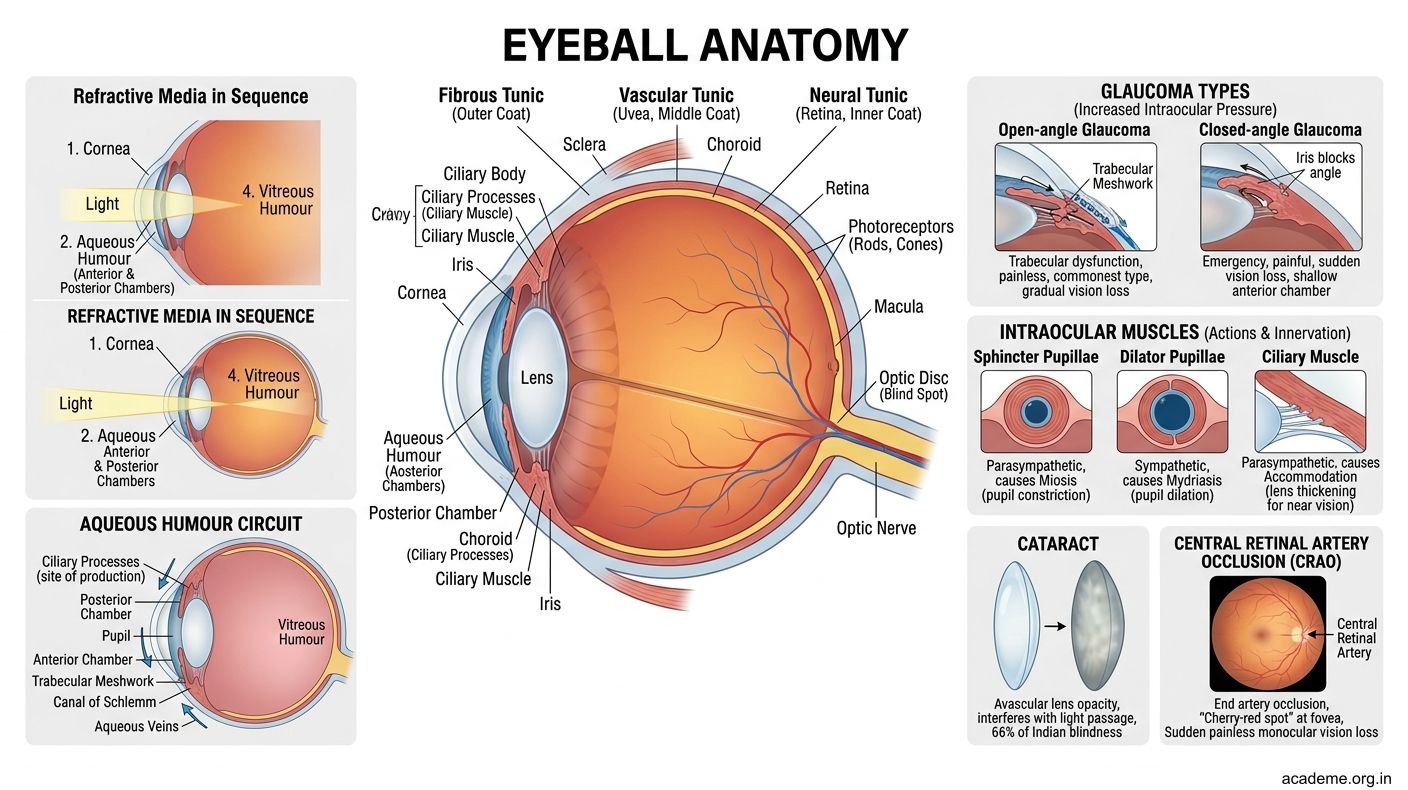
Figure: Key Takeaways — Eyeball (AN41.1-3)
CLINICAL PEARL
Acute Angle-Closure Glaucoma — A Medical Emergency
Unlike open-angle glaucoma (which is painless and insidious), acute angle-closure glaucoma is one of the true ophthalmic emergencies.
It occurs when the iris is pushed forward (by pupillary block from the lens) and occludes the iridocorneal angle — suddenly blocking all aqueous drainage. IOP can rise to 50–70 mmHg within minutes.
Presentation triad: Severe unilateral eye pain + headache + nausea/vomiting + red eye + sudden vision loss + halos around lights
Precipitating factors: dim light (pupil dilates → iris bunches at the angle) — explains why attacks often occur in the evening or in darkened cinema halls. Also precipitated by mydriatic eye drops (atropine, tropicamide).
Anatomically predisposed eyes: Hypermetropic (far-sighted) eyes have a shallower anterior chamber and a narrower angle — predisposing to angle closure.
Treatment: Emergency IV acetazolamide (reduces aqueous secretion) + topical pilocarpine (constricts pupil, pulling iris away from angle) + laser peripheral iridotomy (creates a hole in the iris allowing aqueous to bypass the pupillary block).
In Indian clinical practice, hyperosmotic agents (mannitol 20% IV) are used for rapid IOP reduction before laser treatment.
REFLECT
Return to the hook case — the 68-year-old woman with:
1. Absent red reflex + grey-white lens opacity (right eye)
2. Raised IOP = 28 mmHg
- The absent red reflex is due to opacity of which refractive medium? What is the diagnosis?
- The raised IOP is due to impaired drainage of aqueous humour. Trace the normal pathway of aqueous from production to drainage. At which anatomical point is this pathway obstructed in the most common type of glaucoma?
- If the optic disc shows cupping (cup-to-disc ratio > 0.6), which part of the sclera is being damaged by the raised IOP?
- If this patient also has diabetes, what additional retinal complication should you look for on fundoscopy?
Discussion: The absent red reflex with grey-white opacity = cataract (lens opacity). The red reflex normally comes from light reflecting off the vascular choroid through a transparent lens. Aqueous humour is produced by ciliary processes → posterior chamber → through pupil → anterior chamber → trabecular meshwork → Canal of Schlemm → aqueous veins. In open-angle glaucoma (most common), the trabecular meshwork is dysfunctional, impeding outflow. The optic disc cupping occurs at the lamina cribrosa of the sclera — the weakest sieve-like area where retinal nerve fibres exit. In diabetes, look for diabetic retinopathy — microaneurysms, haemorrhages, hard exudates, new vessel formation (proliferative retinopathy).
KEY TAKEAWAYS
Key Takeaways — Eyeball (AN41.1-3)
Three Coats:
• Outer fibrous: Cornea (transparent, anterior 1/6, most refraction) + Sclera (opaque, posterior 5/6)
• Middle uvea: Choroid (nourishes retina) + Ciliary body (secretes aqueous, accommodation) + Iris (sphincter = CN III parasympathetic; dilator = sympathetic)
• Inner: Retina (rods = dim light; cones = colour/acuity); Fovea = highest acuity; Optic disc = blind spot + lamina cribrosa
Refractive Media (anterior to posterior): Cornea → Aqueous → Lens → Vitreous
Aqueous Humour Circuit:
Ciliary processes → posterior chamber → pupil → anterior chamber → trabecular meshwork → Canal of Schlemm → aqueous veins
Glaucoma: raised IOP → optic disc cupping at lamina cribrosa
• Open-angle: trabecular meshwork dysfunction (painless, commonest)
• Closed-angle: iris blocks iridocorneal angle (acute emergency, painful)
Cataract: lens opacity; most common cause of Indian blindness; treated by phacoemulsification
CRAO: central retinal artery (end-artery) occlusion → sudden painless monocular blindness; cherry-red spot at macula (thin fovea + intact choroidal supply)
Intraocular Muscles:
• Sphincter pupillae (miosis) — CN III parasympathetic via ciliary ganglion
• Dilator pupillae (mydriasis) — sympathetic (superior cervical ganglion → long ciliary nerve)
• Ciliary muscle (accommodation, near vision) — CN III parasympathetic