Page 1 of 4
AN43.1-9 | Head & neck Joints, Histology, Development, Radiography & Surface marking — SDL Guide
Learning Objectives
- Describe and demonstrate the movements of the atlantooccipital and atlantoaxial joints with the muscles producing those movements (AN43.1)
- Identify, describe, and draw the microanatomy of pituitary, thyroid, parathyroid, tongue, salivary glands, tonsil, epiglottis, cornea, and retina (AN43.2)
- Identify, describe, and draw the microanatomy of olfactory epithelium, eyelid, lip, sclero-corneal junction, optic nerve, cochlea-organ of Corti, pineal gland (AN43.3)
- Describe the development and developmental basis of congenital anomalies of face, palate, tongue, branchial apparatus, pituitary, thyroid, and eye (AN43.4)
- Demonstrate clinical examination of cranial nerves, palpation of carotid arteries, facial artery, superficial temporal artery, and surface anatomy of major H&N structures (AN43.5–43.6)
- Identify anatomical structures in skull X-rays (PA, lateral) and cervical spine X-rays (AP and lateral) (AN43.7)
- Describe the anatomical route for carotid and vertebral angiogram (AN43.8–43.9)
INSTRUCTIONS
This is an integration module. Work systematically through each topic. The histology sections require concurrent practical lab revision. The radiography section is best studied alongside actual X-ray films.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head & Neck (Textbook)
- Gray's Anatomy for Students — Chapters 8 & 9 (Textbook)
- Inderbir Singh's Textbook of Human Histology (Textbook)
- Langman's Medical Embryology — Head and Neck (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 3-year-old child is brought to a paediatric surgery OPD in Chennai with a midline neck swelling that moves with swallowing and protrusion of the tongue. An X-ray of the cervical spine shows an unusual widening of the atlantoaxial interval. A second patient — a newborn — has a cleft lip and palate.
What developmental defects explain these two presentations? What is the normal embryological origin of the midline neck structure? What is the safe range for the atlantoaxial interval on X-ray?
This integration module ties together the joints, histology, embryology, surface anatomy, and radiology of the head and neck region — essential for the clinical year examinations and for patient care.
WHY THIS MATTERS
This module covers the integrative and applied aspects of head and neck anatomy:
- Atlantoaxial instability — important in Down syndrome (lax transverse ligament), rheumatoid arthritis, and post-traumatic C1-C2 injuries; a missed diagnosis can cause spinal cord compression
- Thyroglossal duct cyst — the most common midline neck swelling in children; moves with tongue protrusion (attached to hyoid bone via the tract)
- Cleft lip and palate — among the most common congenital anomalies in India; requires multidisciplinary surgical and speech therapy management
- Branchial cyst — anterior to sternocleidomastoid muscle; remnant of 2nd pharyngeal arch cleft; clinical differential diagnosis of lateral neck swellings
- Skull X-rays — still used in India for trauma assessment, sinusitis, and intracranial calcifications at the primary care level
RECALL
Before we begin, recall:
- The atlas (C1) has no vertebral body (it was absorbed into the dens of the axis). It has anterior and posterior arches with two lateral masses
- The axis (C2) has the dens (odontoid process) — the absorbed atlas body — which acts as a pivot for rotation
- The pharyngeal arches are numbered 1–6 (the 5th is vestigial); each contributes bones, muscles, nerves, and arteries to specific head and neck structures
- The thyroid gland develops from the foramen caecum of the tongue and descends along the thyroglossal duct to its final position in the neck
Part 1: Atlantooccipital and Atlantoaxial Joints (AN43.1)
Atlantooccipital Joint

Figure: Atlantoaxial Joint

Figure: Part 1: Atlantooccipital and Atlantoaxial Joints (AN43.1)
- Type: Synovial, ellipsoid (condyloid) joint — bilateral between occipital condyles and superior articular facets of atlas
- Movements: Nodding (yes movement) — flexion and extension; small amount of lateral flexion (but NO rotation)
- Muscles producing flexion: Prevertebral muscles (longus capitis, rectus capitis anterior)
- Muscles producing extension: Suboccipital muscles (rectus capitis posterior major and minor, obliquus capitis superior); trapezius; splenius capitis
- Ligaments: Anterior and posterior atlanto-occipital membranes; capsular ligaments
Atlantoaxial Joint
- Type: Three joints: Two lateral synovial joints (atlas lateral masses on axis superior articular facets) + One median atlantoaxial joint (dens of axis articulating with anterior arch of atlas + held by transverse ligament of atlas)
- Movements: Rotation (no movement) — head rotation (shaking "no"); approximately 40–45° each side; contributes 50% of total cervical rotation
- Key ligament: Transverse ligament of atlas — the most important stabilising structure; keeps the dens against the anterior arch of atlas; prevents dens from compressing the spinal cord
The alar ligaments (from dens to occipital condyles) limit excessive rotation.
Atlantoaxial interval (ADI) on lateral cervical X-ray:
• Adults: ≤ 3 mm
• Children: ≤ 5 mm
• >3 mm in adults = transverse ligament rupture or laxity; immediate neurosurgical concern
Clinical conditions causing atlantoaxial instability:
• Down syndrome — lax transverse ligament due to connective tissue hypotonia; all Down syndrome patients should have cervical X-ray before contact sports
• Rheumatoid arthritis — pannus formation erodes the transverse ligament
• Odontoid fractures (Type II most common) — dens fracture at the base; high-velocity trauma
• Grisel syndrome — non-traumatic atlantoaxial subluxation from ligamentous laxity due to head and neck infection (retropharyngeal abscess, tonsillitis) — seen in children
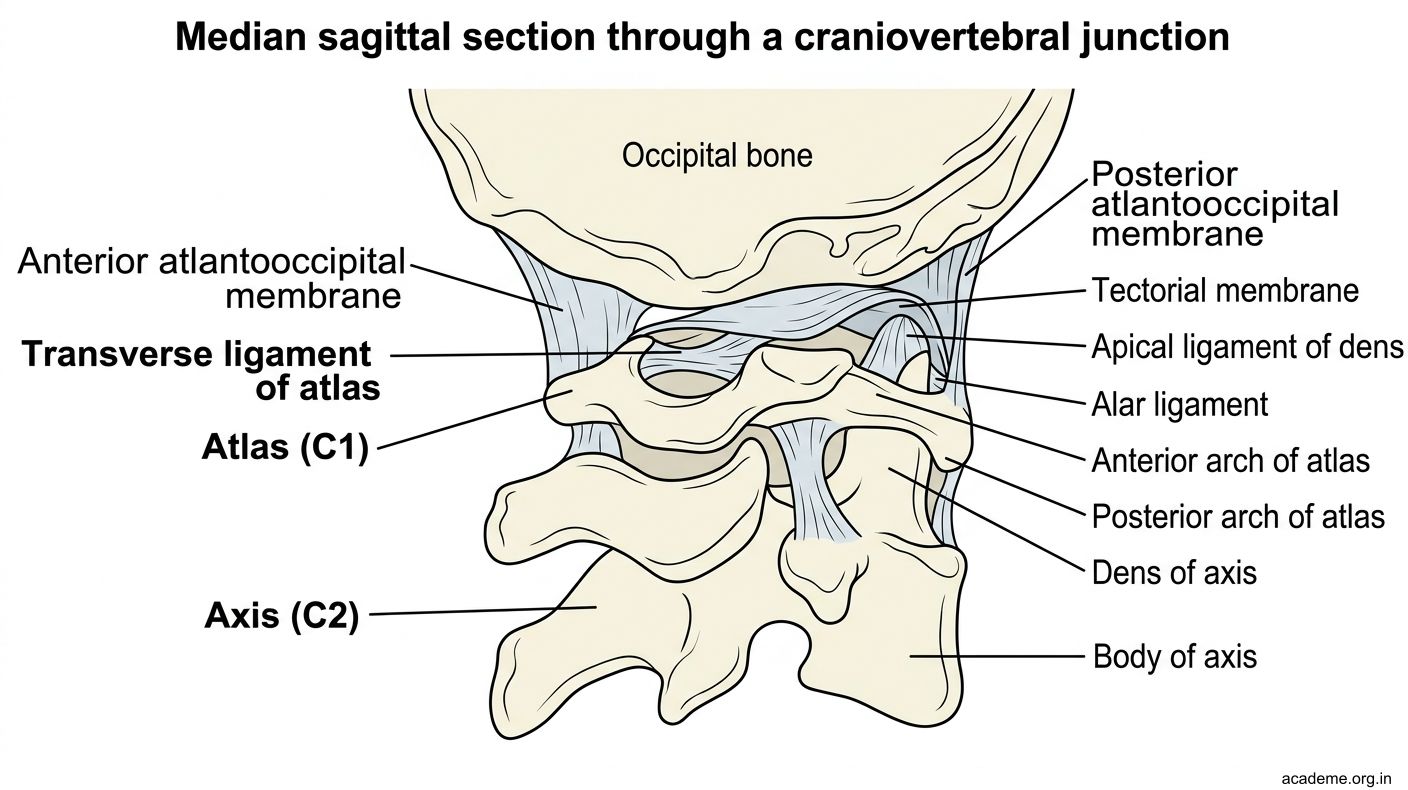
Figure: Part 1: Atlantooccipital and Atlantoaxial Joints (AN43.1)
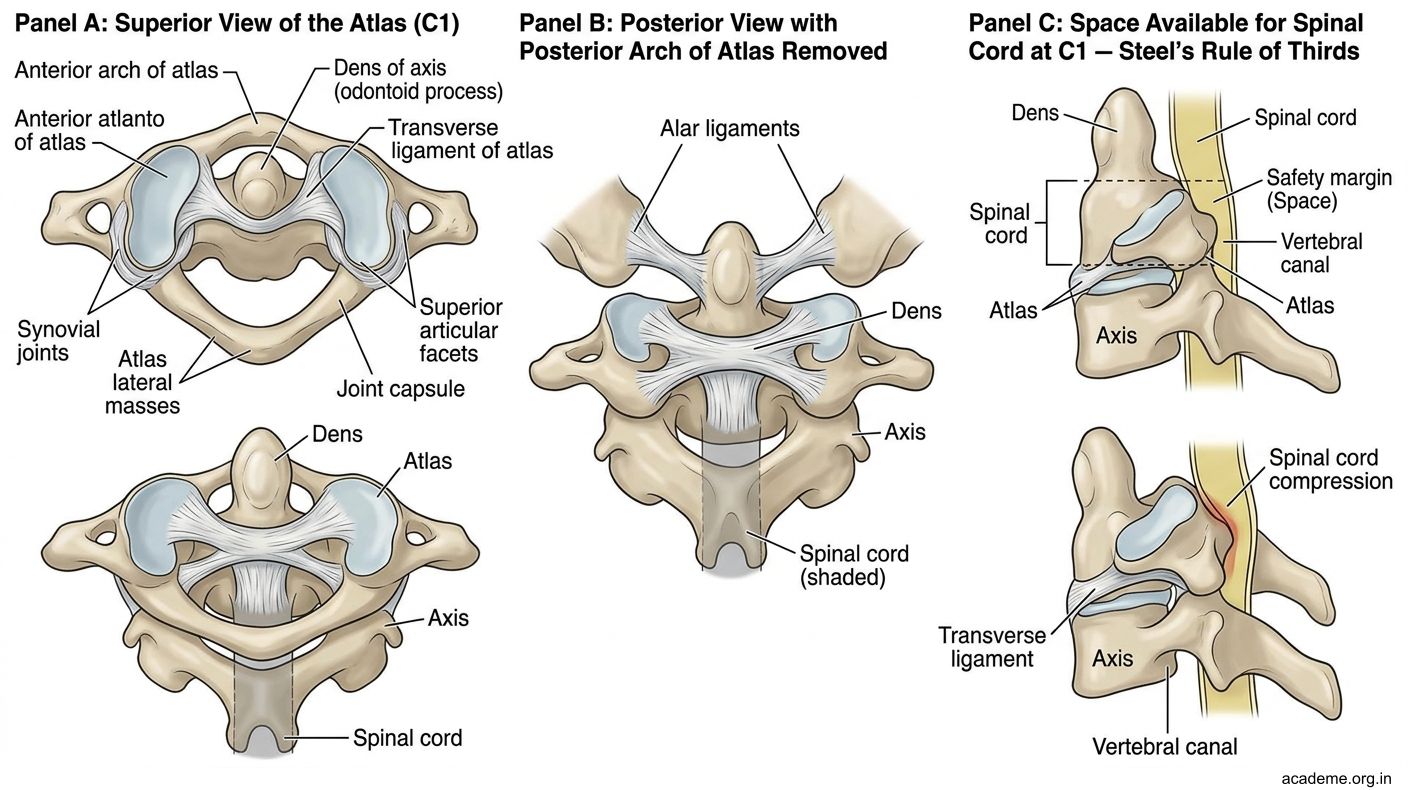
Figure: Atlantoaxial Joint
Part 2: Head & Neck Histology (AN43.2–43.3)
Key H&N Structures in Histology Practicals (AN43.2)
Thyroid Gland:
• Follicles — spherical units surrounded by simple cuboidal-to-columnar follicular cells
• Colloid — eosinophilic material in the follicle lumen (stored thyroglobulin)
• Parafollicular (C) cells — pale, larger cells between follicles; secrete calcitonin
• Key ID feature: Pink colloid within follicles + surrounding epithelium
Parathyroid Gland:
• Chief (principal) cells — small, dark-staining; secrete PTH
• Oxyphil cells — larger, acidophilic (pink), appear after puberty; function uncertain
• Fat cells — increase with age
• Key ID feature: Densely packed chief cells with scattered pink oxyphil cells; very little stroma
Pituitary Gland (Hypophysis):
• Anterior lobe (adenohypophysis): Acidophils (somatotropes, lactotropes) + Basophils (corticotropes, thyrotropes, gonadotropes) + Chromophobes
• Posterior lobe (neurohypophysis): Pituicytes (glial cells) + Herring bodies (axon terminals storing ADH and oxytocin)
• Key ID feature: Anterior = cellular with colour variation; posterior = pale, paucicellular with Herring bodies
Salivary Glands:
• Parotid — purely serous acini (basophilic, zymogen granules); striated ducts
• Submandibular — mixed (predominantly serous with some mucous); serous demilunes capping mucous acini
• Sublingual — predominantly mucous; few serous demilunes
Palatine Tonsil:
• Stratified squamous non-keratinised epithelium covering + invaginated to form crypts
• Germinal centres (lymphoid follicles with active B-cell proliferation) in connective tissue
• Capsule of fibrous tissue partially enclosing it
• Key ID feature: Crypts lined by squamous epithelium infiltrated by lymphocytes + germinal centres
Cornea:
• 5 layers (anterior to posterior): Stratified squamous non-keratinised epithelium → Bowman's membrane (acellular collagen) → Stroma (regularly arranged collagen lamellae = transparency) → Descemet's membrane (thick basement membrane) → Endothelium (simple squamous = active fluid pump)
• Key ID feature: Regular collagen lamellae in stroma; no blood vessels; regular stratified squamous epithelium anteriorly
Retina:
• 10 layers (from outermost → innermost): RPE → Photoreceptors → Outer limiting membrane → Outer nuclear → Outer plexiform → Inner nuclear → Inner plexiform → Ganglion cell layer → Nerve fibre layer → Inner limiting membrane
• Simplified: RPE (outermost) → Rods/Cones → Bipolar cells → Ganglion cells → Nerve fibres (innermost)
Additional structures for AN43.3:
• Epiglottis: Elastic cartilage core + lingual surface = stratified squamous; laryngeal surface = pseudostratified ciliated columnar (respiratory) with transition zone
• Olfactory epithelium: Pseudostratified columnar with Olfactory receptor cells (bipolar neurons, CN I), Supporting (sustentacular) cells, and Basal cells; Bowman's olfactory glands in lamina propria
• Cochlea — Organ of Corti: Sits on basilar membrane in scala media; Hair cells (inner and outer) with stereocilia; Tectorial membrane above; Tunnel of Corti between inner and outer pillar cells; hair cell deflection → CN VIII (cochlear) signal
SELF-CHECK — : Joints and Histology
Which ligament is the most critical stabiliser of the atlantoaxial joint, and its failure in rheumatoid arthritis leads to atlantoaxial instability?
A. Anterior longitudinal ligament
B. Transverse ligament of atlas
C. Alar ligament
D. Ligamentum nuchae
Reveal Answer
Answer: B. Transverse ligament of atlas
On histological examination, a gland shows spherical follicles filled with pink colloid and lined by simple cuboidal-to-columnar cells. Occasional larger pale cells are seen between follicles. This gland is:
A. Parathyroid gland
B. Pituitary gland (anterior lobe)
C. Thyroid gland
D. Adrenal gland
Reveal Answer
Answer: C. Thyroid gland
The parotid gland is distinguished histologically from the sublingual gland because the parotid contains:
A. Only mucous acini
B. Mixed acini with mucous predominance
C. Only serous acini
D. Abundant adipose tissue and mucous acini
Reveal Answer
Answer: C. Only serous acini
Part 3: Development of H&N Structures (AN43.4)
Pharyngeal (Branchial) Arches — Overview

Figure: Development of the Thyroid Gland

Figure: Development of the Tongue
| Arch | Skeletal derivatives | Muscles | Nerve | Artery |
|---|---|---|---|---|
| 1st (mandibular) | Malleus, incus, mandible, maxilla, zygomatic, squamous temporal | Muscles of mastication, tensor tympani, tensor palati, mylohyoid, ant. digastric | CN V (trigeminal) | Maxillary artery |
| 2nd (hyoid) | Stapes, styloid process, lesser horn of hyoid, upper body of hyoid | Muscles of facial expression, stapedius, stylohyoid, post. digastric | CN VII (facial) | Stapedial artery (regresses) |
| 3rd | Greater horn + lower body of hyoid | Stylopharyngeus | CN IX (glossopharyngeal) | Common carotid, proximal internal carotid |
| 4th | Thyroid cartilage, epiglottis | Pharyngeal constrictors, cricothyroid | CN X (vagus) — superior laryngeal | Aortic arch (left), right subclavian (right) |
| 6th | Cricoid + arytenoid cartilages | Intrinsic laryngeal muscles (except cricothyroid) | CN X (vagus) — recurrent laryngeal | Ductus arteriosus (left), right pulmonary (right) |
Development of the Face
The face develops from 5 processes surrounding the stomodeum (primitive mouth):
• Frontonasal process (1 midline) — forms forehead, bridge of nose, medial nose, philtrum of upper lip, primary palate
• Maxillary processes (2 lateral) — form cheeks, lateral upper lip, secondary palate
• Mandibular processes (2 inferior) — form lower jaw, lower lip, lower face
Cleft lip: Failure of fusion of the maxillary process with the medial nasal process of the frontonasal process. Usually paramedian (lateral to philtrum). Can be unilateral or bilateral. Associated with maternal folic acid deficiency, phenytoin use, and chromosomal anomalies.
Cleft palate: Failure of fusion of the two palatine shelves (from maxillary processes) with each other and/or with the primary palate anteriorly and the nasal septum superiorly. Can be isolated or associated with cleft lip.
Development of the Tongue
- Anterior 2/3: Two lingual swellings + tuberculum impar from the 1st pharyngeal arch → hence general sensory = CN V3, taste = CN VII (chorda tympani accompanies)
- Posterior 1/3: Copula (from 2nd and 3rd arches) → the 3rd arch overgrows the 2nd → hence CN IX supplies posterior 1/3
- Epiglottis: 4th arch + hypobranchial eminence → CN X (superior laryngeal nerve)
Development of the Thyroid Gland
The thyroid develops from the floor of the pharynx at the foramen caecum (between anterior 2/3 and posterior 1/3 of tongue — at the apex of the sulcus terminalis) and descends in front of the pharynx as the thyroglossal duct. It reaches its final position in the neck by week 7. The thyroglossal duct normally obliterates.
Thyroglossal duct cyst: Failure of obliteration → cyst along the thyroglossal duct path; most commonly at or below the hyoid bone; moves upward on swallowing AND on tongue protrusion (connected to tongue via the duct remnant through the hyoid bone — Sistrunk's procedure excises the cyst + middle 1/3 of hyoid bone).
Development of the Pituitary Gland:
• Adenohypophysis (anterior lobe) — from Rathke's pouch (ectodermal upward evagination of the roof of stomodeum)
• Neurohypophysis (posterior lobe) — from infundibulum (neuroectodermal downward outgrowth of hypothalamus)
Craniopharyngioma — tumour arising from Rathke's pouch remnants in the sella turcica → bitemporal hemianopia (compresses optic chiasm) + hypopituitarism
Development of the Eye:
• Optic vesicle (evagination from prosencephalon) → invaginates to form optic cup (double-layered: outer = retinal pigment epithelium, inner = neural retina)
• Lens vesicle — from surface ectoderm induced by the optic cup
• Cornea — from surface ectoderm + neural crest cells
• Congenital anomalies: Coloboma (failure of fetal fissure closure) → notch in iris/retina/choroid; Congenital cataract (rubella, galactosaemia, chromosomal); Cyclopia (failure of forebrain cleavage)

Figure: Pharyngeal (Branchial) Arches — Overview
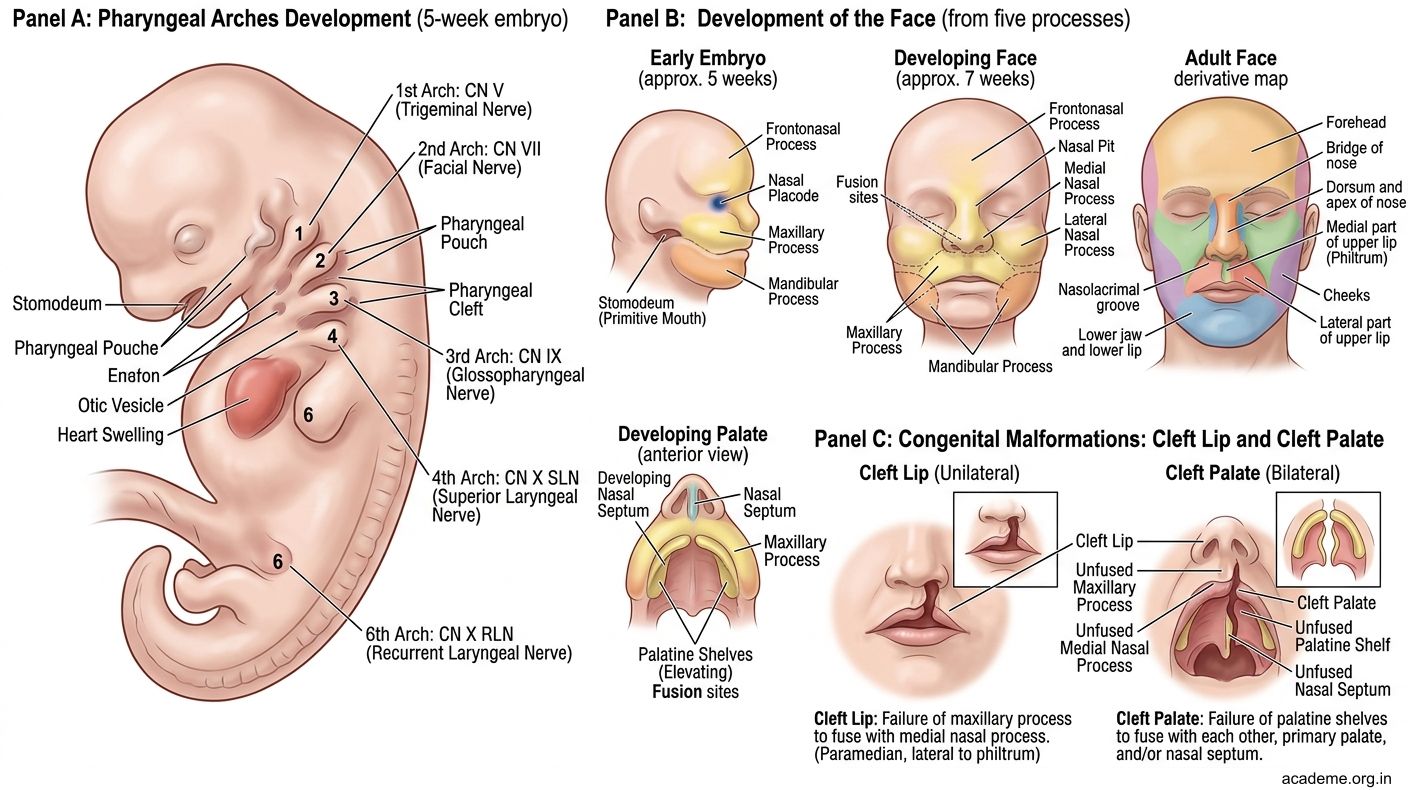
Figure: Pharyngeal (Branchial) Arches — Overview
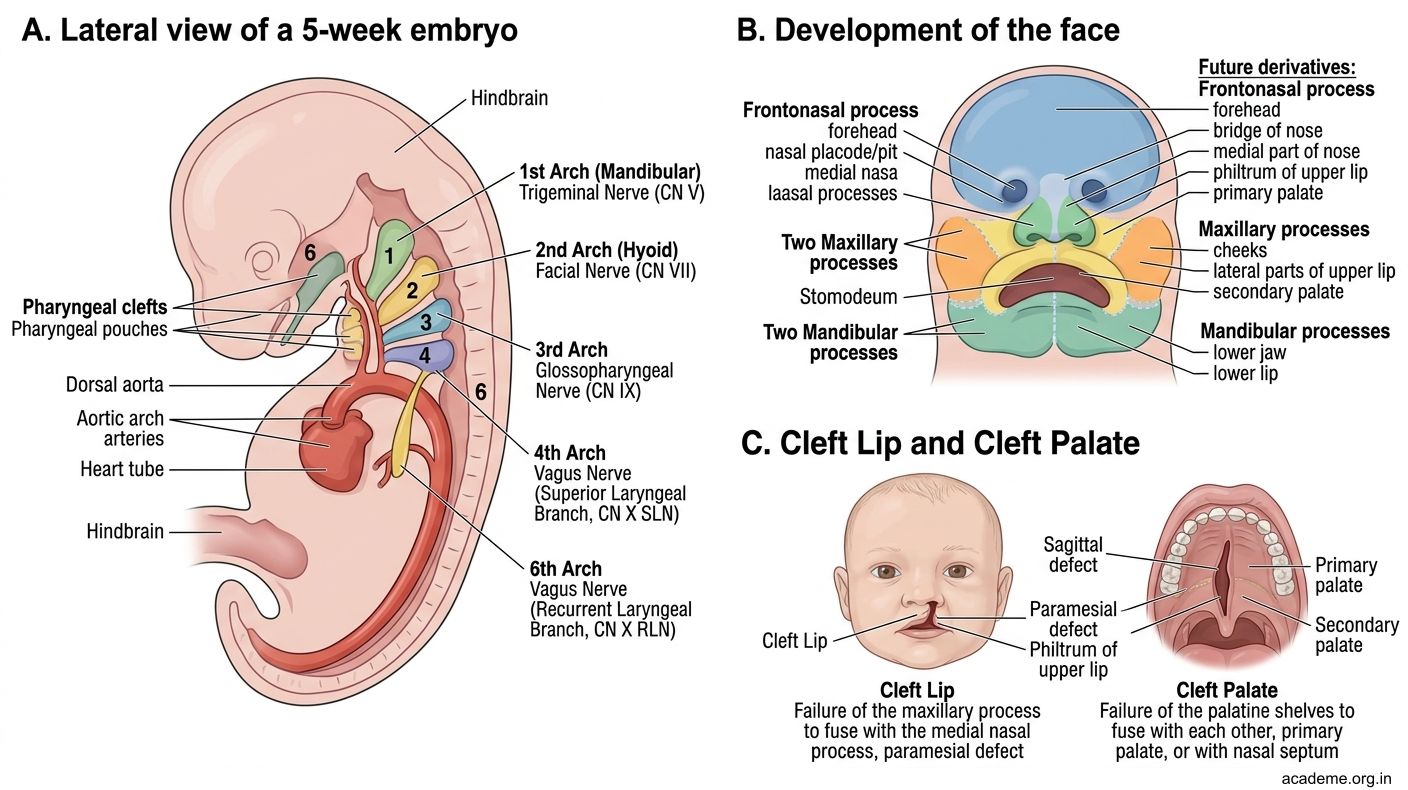
Figure: Pharyngeal (Branchial) Arches — Overview
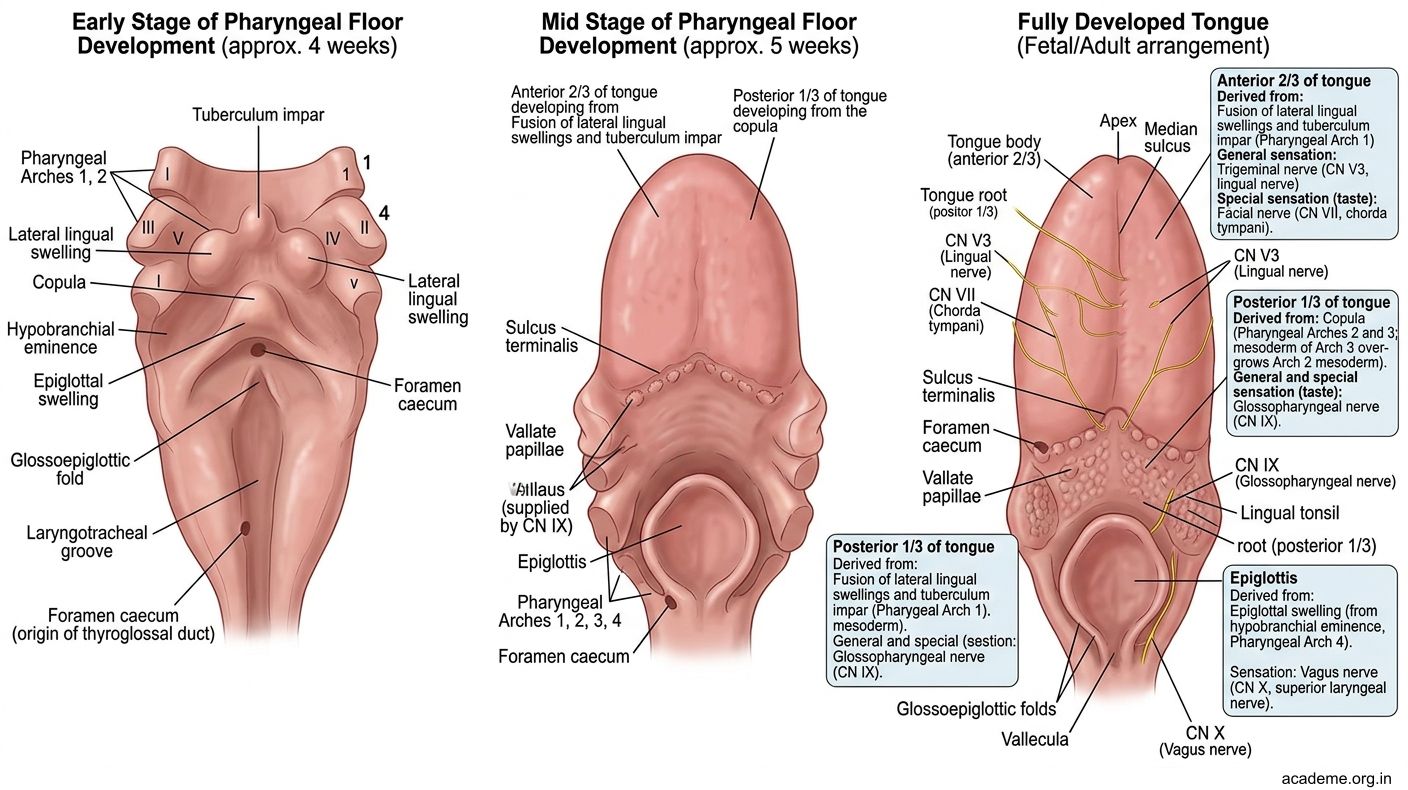
Figure: Development of the Tongue
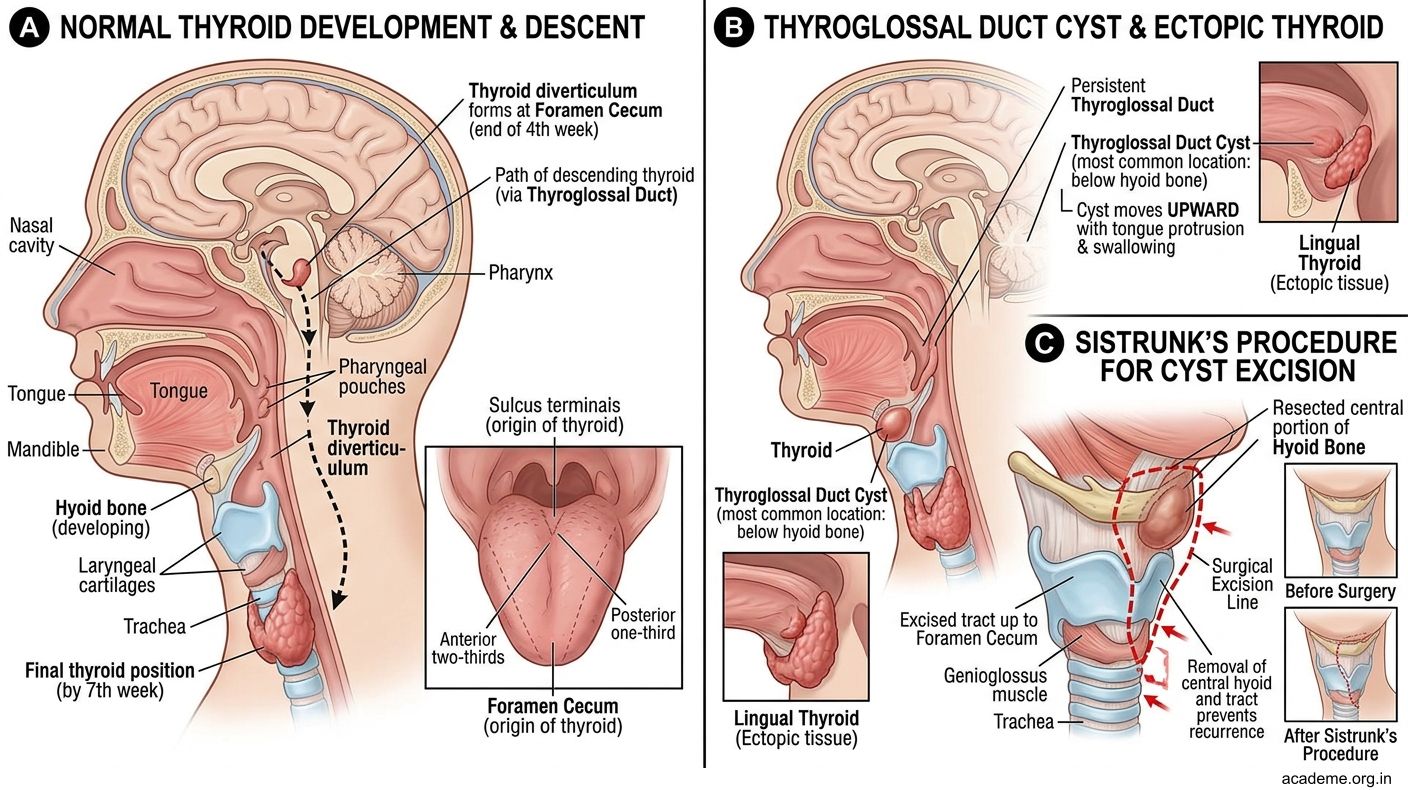
Figure: Development of the Thyroid Gland
Part 4: Surface Anatomy and Radiography of the H&N (AN43.5–43.9)
Clinical Examination and Surface Projections (AN43.5–43.6)

Figure: The Dangerous Area of the Face — Cavernous Sinus Thrombosis

Figure: Carotid and Vertebral Angiogram (AN43.8–43.9)

Figure: Clinical Examination and Surface Projections (AN43.5–43.6)
Hyoid bone: C3 vertebral level; palpable in the midline just above the thyroid cartilage; moves with swallowing; fracture is rare but seen in strangulation/hanging — classic forensic finding
Thyroid cartilage (laryngeal prominence/Adam's apple): C4-C5 level; the thyroid notch is palpable superiorly; in males, the notch is angular; in females, more rounded; the inferior border is at C5
Cricoid cartilage: C6 vertebral level; the cricothyroid membrane is palpable between the thyroid and cricoid cartilages — site of emergency cricothyrotomy (when intubation is impossible)
Carotid arteries:
• Common carotid artery — palpate by compressing it against the carotid tubercle (C6) — the anterior tubercle of the transverse process of C6 (Chassaignac's tubercle); lies medial to SCM
• External carotid — has branches above the hyoid (facial, occipital, etc.)
• Internal carotid — no branches in the neck
Facial artery: Crosses the inferior border of the mandible at the anterior border of masseter — palpable here as a pulse; curves to the angle of mouth and nose
Superficial temporal artery: Palpable in the pre-auricular region (anterior to the tragus); branches on the temporal scalp; temporal artery biopsy site for giant cell (temporal) arteritis — the most common cause of vasculitis in adults over 50
External jugular vein: Visible on surface from angle of mandible, crossing SCM obliquely downward, to the midpoint of the clavicle; used for emergency venous access when peripheral veins are collapsed
Pterion: Junction of frontal, parietal, temporal, and greater wing of sphenoid — the thinnest part of the skull; overlies the anterior division of the middle meningeal artery; a blow to the temple → epidural haematoma
H&N Radiography (AN43.7)
Skull X-ray — lateral view, key structures:
• Pituitary fossa (sella turcica) — in the body of sphenoid; look for enlargement (pituitary tumour) or double floor (asymmetric)
• Calcified pineal gland — midline; displacement indicates space-occupying lesion
• Vascular markings — middle meningeal artery grooves on inner table
• Frontal sinus, maxillary sinus (not well seen), mastoid air cells
Skull X-ray — PA (frontal) view:
• Crista galli — midline bony projection of ethmoid
• Frontal and ethmoidal air sinuses
• Petrous ridge — dense horizontal line crossing the orbits; the dense petrous temporal bone
• Superior orbital fissure — oval lucency within each orbit
• Foramen rotundum — round lucency below each superior orbital fissure (CN V2)
Cervical spine X-ray — lateral view:
• Atlantoaxial interval (ADI) — distance between anterior arch of atlas and dens: ≤3 mm adults, ≤5 mm children
• Prevertebral soft tissue — anterior to C2-C3 = ≤7 mm (widening = retropharyngeal abscess or haematoma)
• Anterior and posterior vertebral lines, spinolaminar line, posterior spinal line (spinous processes) — step = fracture-dislocation
• C7 body is usually the most prominent on lateral view (cervicothoracic junction)
Carotid and Vertebral Angiogram (AN43.8–43.9)
Carotid angiogram anatomical route:
• Femoral artery (most common access) → Seldinger technique → aorta → common carotid artery → internal carotid artery → carotid siphon → intracranial circulation (MCA, ACA)
• Alternatively: radial or brachial artery access
• Structures visualised: Internal carotid artery, carotid bifurcation, common carotid
Vertebral angiogram:
• Femoral artery → subclavian artery → vertebral artery (first branch of subclavian, runs in transverse foramina of C6-C1) → basilar artery → posterior cerebral arteries (PCA)
• Normal vertebral artery enters the transverse foramen at C6 (occasionally C5 or C7 — important variant)
Indications in Indian practice: stroke, carotid stenosis, cerebral aneurysm, AVM, vertebrobasilar TIA
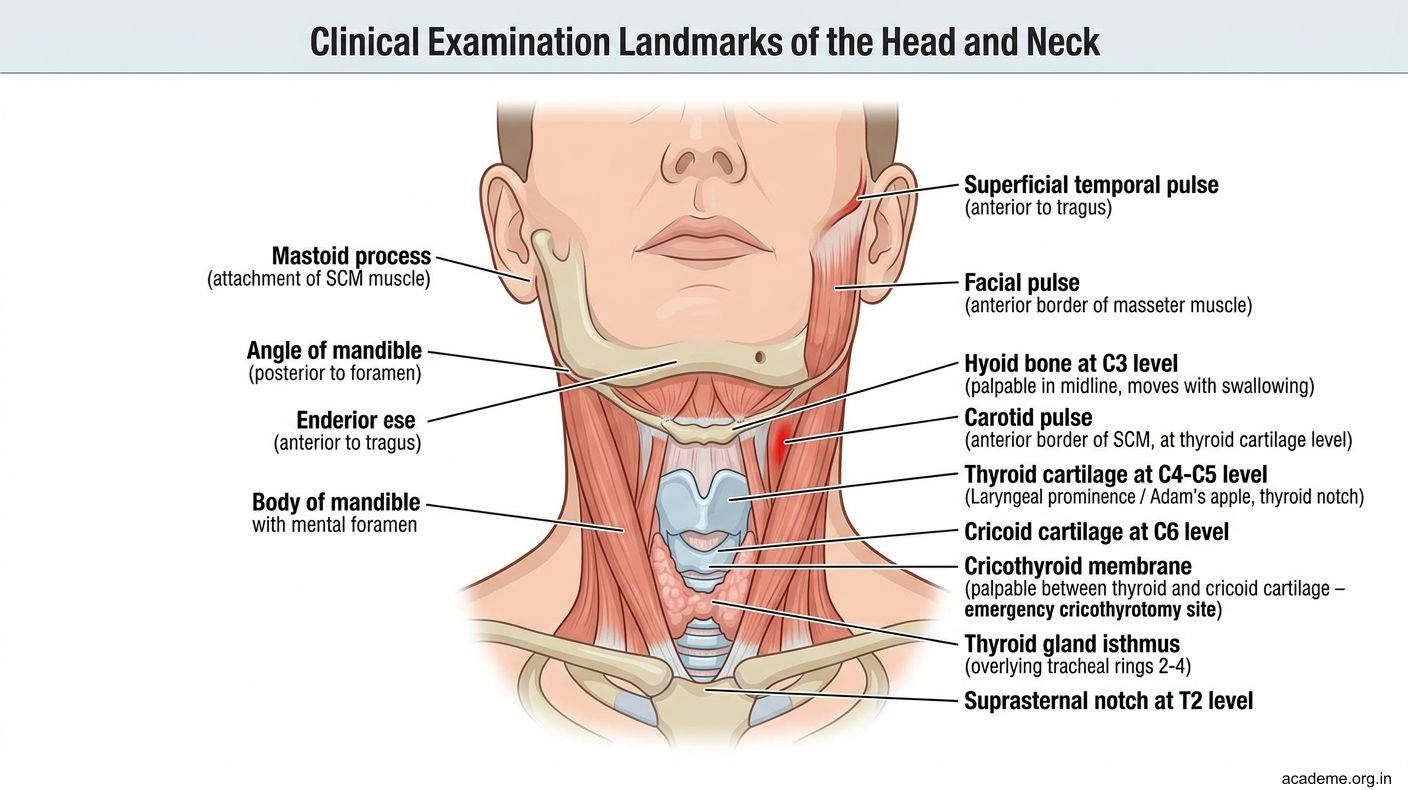
Figure: Clinical Examination and Surface Projections (AN43.5–43.6)
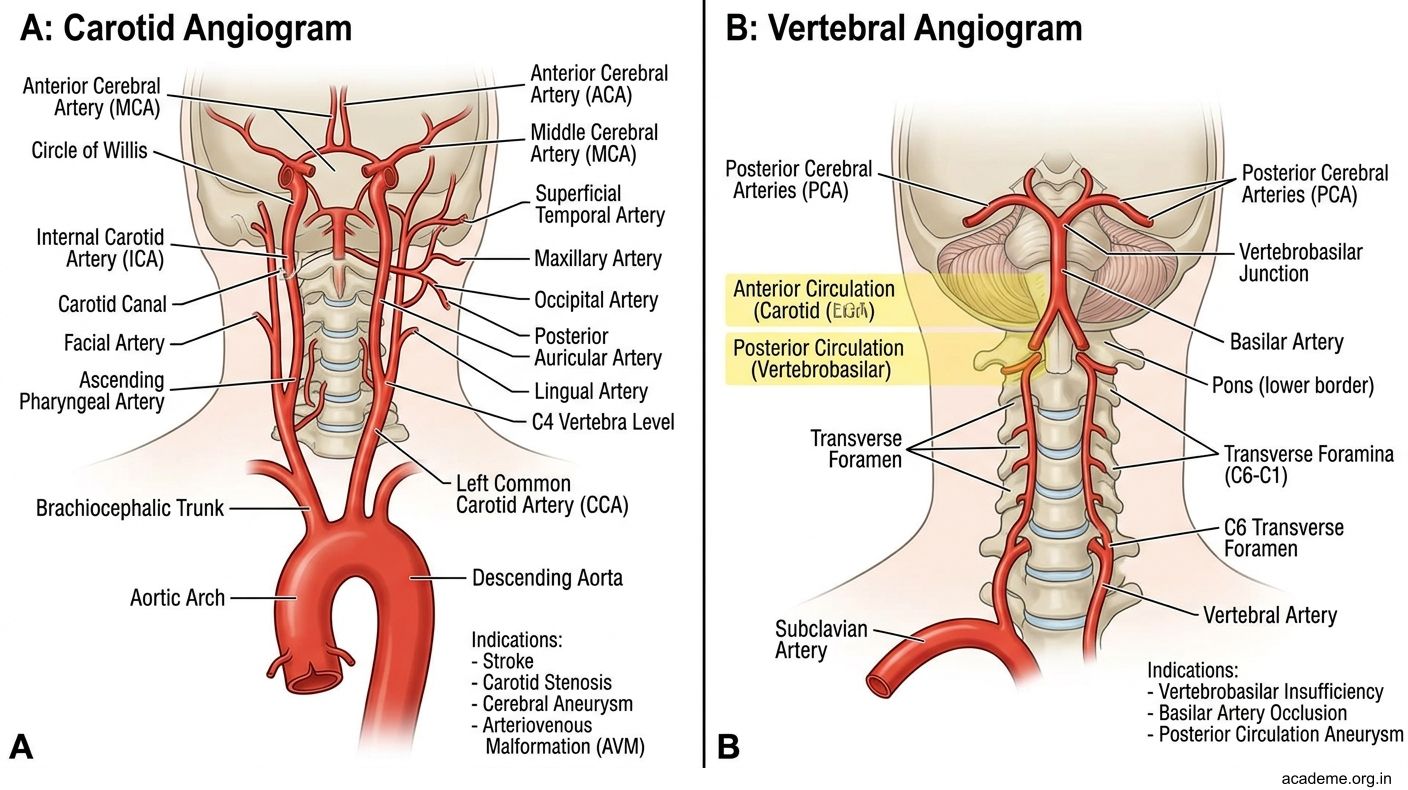
Figure: Carotid and Vertebral Angiogram (AN43.8–43.9)
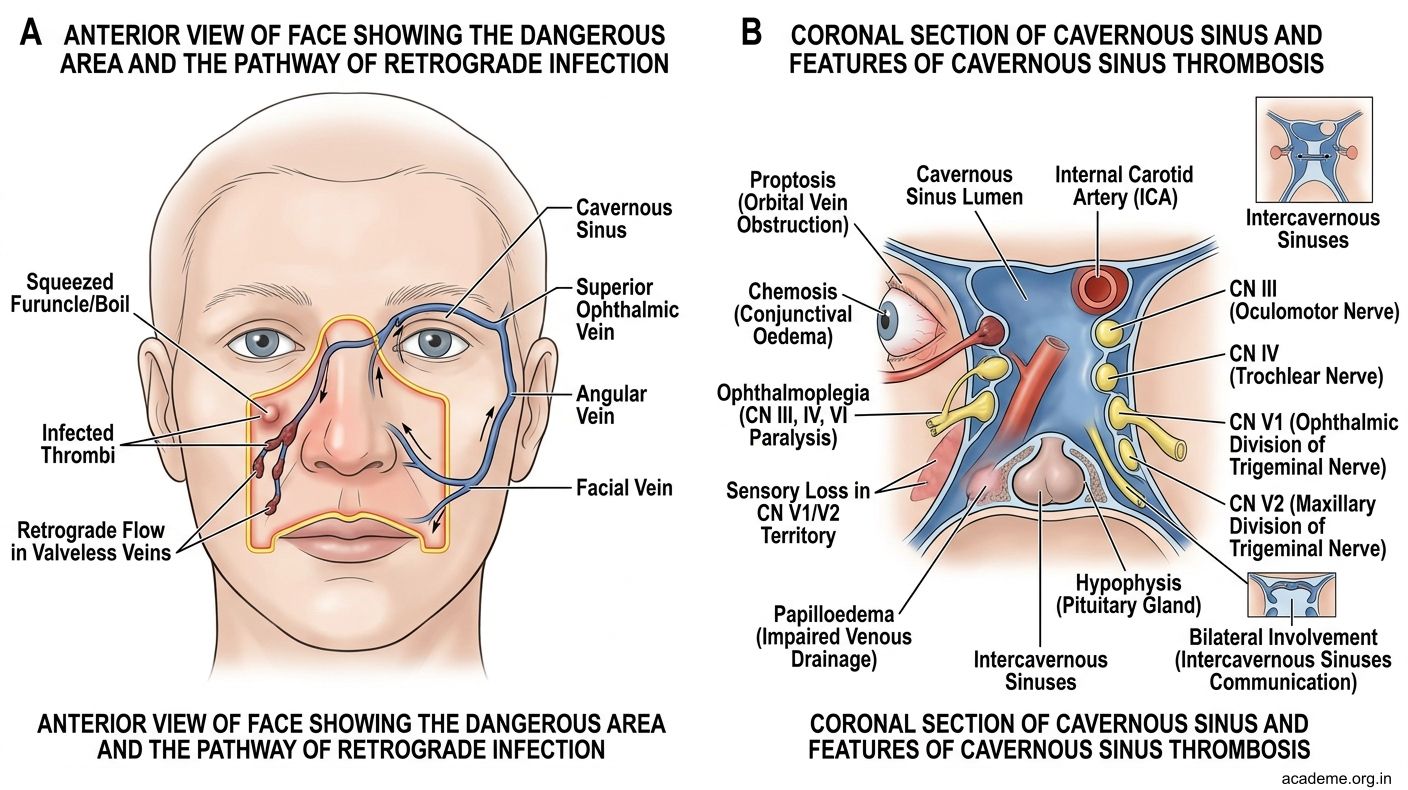
Figure: The Dangerous Area of the Face — Cavernous Sinus Thrombosis
SELF-CHECK — : Development and Radiology
A thyroglossal duct cyst differs from a branchial cyst in that it moves on:
A. Swallowing only
B. Tongue protrusion only
C. Both swallowing and tongue protrusion
D. Deep inspiration
Reveal Answer
Answer: C. Both swallowing and tongue protrusion
On a lateral skull X-ray, the pituitary fossa (sella turcica) is seen in the body of which bone?
A. Temporal bone
B. Ethmoid bone
C. Sphenoid bone
D. Occipital bone
Reveal Answer
Answer: C. Sphenoid bone
The cricothyroid membrane, used for emergency cricothyrotomy, lies between which two cartilages?
A. Epiglottis and thyroid cartilage
B. Thyroid cartilage and cricoid cartilage
C. Cricoid cartilage and first tracheal ring
D. Arytenoid cartilage and thyroid cartilage
Reveal Answer
Answer: B. Thyroid cartilage and cricoid cartilage
CLINICAL PEARL
The Dangerous Area of the Face — Cavernous Sinus Thrombosis
The facial vein in the face is unique: it lacks valves and is connected to the cavernous sinus in the cranial cavity via:
• Superior ophthalmic vein (drains the medial angle of the eye → cavernous sinus)
• Pterygoid venous plexus (via deep facial vein → emissary veins → cavernous sinus)
The dangerous area of the face is the region around the nose, upper lip, and medial cheek — bordered by the corners of the mouth and the bridge of the nose. Squeezing or incising an infected furuncle (boil) in this area can push infected thrombi in retrograde fashion into the cavernous sinus, causing cavernous sinus thrombosis.
Features of cavernous sinus thrombosis: Proptosis (orbital vein obstruction), chemosis (conjunctival oedema), ophthalmoplegia (CN III, IV, VI run in the cavernous sinus wall), facial pain (CN V1, V2 run in the sinus wall), and fever. It is a life-threatening emergency requiring IV antibiotics (anti-staphylococcal + anaerobic cover) and anticoagulation.
This is why surgeons are taught: "Never squeeze a boil on the face — especially in the dangerous area."
REFLECT
Return to the hook cases:
Case 1 — 3-year-old with midline neck swelling that moves with swallowing and tongue protrusion:
1. From which embryological structure does this cyst derive, and what is the normal fate of this structure?
2. Why does the swelling move with tongue protrusion specifically?
3. Why is middle 1/3 hyoidectomy included in the surgical procedure (Sistrunk's operation)?
Case 2 — Newborn with cleft lip and palate:
1. Which embryological processes failed to fuse to cause (a) the cleft lip and (b) the cleft palate?
2. In the lateral cervical X-ray showing ADI of 5 mm in a 3-year-old — is this normal or abnormal? What is the clinical concern if it were >5 mm?
Discussion: Case 1 = thyroglossal duct cyst; normal thyroglossal duct obliterates after thyroid descends; attachment to tongue base via duct remnant + passage through hyoid bone → moves with tongue protrusion + swallowing; middle 1/3 hyoidectomy removes the tract remnant that passes through/above the hyoid (to prevent recurrence). Case 2 cleft lip = failure of maxillary process–medial nasal process fusion; cleft palate = failure of palatine shelf fusion. ADI of 5 mm in a 3-year-old is the upper limit of normal in children; >5 mm = transverse ligament rupture or laxity — risk of cord compression with neck flexion.
KEY TAKEAWAYS
Key Takeaways — H&N Joints, Histology, Development, Radiology (AN43.1-9)
Joints:
• Atlantooccipital: nodding (flexion/extension) — ellipsoid joint
• Atlantoaxial: rotation — transverse ligament of atlas is key stabiliser; ADI ≤3 mm adults, ≤5 mm children
Histology Key IDs:
• Thyroid: pink colloid follicles + C cells
• Parathyroid: chief cells + pink oxyphil cells
• Pituitary: anterior = acidophils/basophils/chromophobes; posterior = pituicytes + Herring bodies
• Parotid = serous only; Submandibular = mixed (predominantly serous); Sublingual = predominantly mucous
• Cornea: regular collagen stroma (transparency), avascular
• Retina: RPE → rods/cones → bipolar → ganglion cells
Development:
• Pharyngeal arches 1-6: 1=CN V (jaw, malleus, incus); 2=CN VII (facial muscles, stapes); 3=CN IX (stylopharyngeus); 4=CN X superior laryngeal; 6=CN X recurrent laryngeal
• Tongue: anterior 2/3 from 1st arch (CN V3/VII); posterior 1/3 from 3rd arch (CN IX)
• Thyroid: foramen caecum → thyroglossal duct → descends to neck; cyst = failure of obliteration
• Cleft lip = maxillary process + medial nasal process fusion failure
• Cleft palate = palatine shelf fusion failure
Surface Anatomy:
• Hyoid = C3; Thyroid cartilage = C4-5; Cricoid = C6 (cricothyrotomy site)
• Carotid pulsation: compress against C6 (Chassaignac's tubercle)
Radiology:
• Lateral skull: sella turcica (sphenoid), pineal gland, middle meningeal artery grooves
• Cervical spine lateral: ADI, prevertebral soft tissue (>7 mm at C2-C3 = retropharyngeal abscess)