Page 1 of 6
AN44.1-7 | Anterior abdominal wall — SDL Guide
The anterior abdominal wall is far more than a protective cover — it is a dynamic muscular sheet that breathes, generates intra-abdominal pressure, protects viscera, and provides the surgical access routes used in nearly every abdominal operation. In this module you will master its layered structure, the planes and regions used to localise abdominal pain, the ingenious mechanics of the rectus sheath, the inguinal canal that gives rise to the commonest hernias in men, and the basis of the incisions your surgeons will use.
Learning Outcomes
- Describe the planes, regions, and quadrants of the abdomen and their clinical use in localising pathology (AN44.1)
- Identify the fascia, nerves, and blood vessels of the anterior abdominal wall (AN44.2)
- Describe the formation of the rectus sheath above and below the arcuate line, and its contents (AN44.3)
- Describe the boundaries, contents, and floor of the inguinal canal; define Hesselbach's triangle (AN44.4)
- Explain the anatomical basis of direct and indirect inguinal hernia (AN44.5)
- Describe the attachments and actions of the muscles of the anterior abdominal wall (AN44.6)
- Describe common abdominal incisions with anatomical basis and clinical importance (AN44.7)
PREREQUISITES
Familiarity with general features of vertebrae (lumbar), the rib cage, and the concept of fascial layers is helpful. Basic NCERT knowledge of the digestive system is assumed.
References
- Gray's Anatomy for Students (Drake et al.) — Abdomen chapter (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 2 — Anterior Abdominal Wall (Textbook)
- Clinically Oriented Anatomy (Moore et al.) — Anterior Abdominal Wall (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy | ~50 min
CLINICAL SCENARIO
A 28-year-old vegetable vendor in Chennai notices a bulge in his right groin that appears when he lifts heavy loads and disappears when he lies down. By the time he reaches the government hospital, the bulge has become hard, painful, and irreducible. The surgical resident diagnoses an incarcerated indirect inguinal hernia and books him for emergency surgery.
Why does a hernia emerge at this precise spot? What anatomical defect allows intestine to escape through the abdominal wall? Why is the right side more commonly affected than the left?
The inguinal canal — a passage designed for the descending testis in the fetus — becomes the Achilles heel of the male anterior abdominal wall. Understanding its anatomy is not optional for any doctor who will ever examine a groin.
WHY THIS MATTERS
The anterior abdominal wall is involved in some of the most common clinical situations you will encounter:
- Inguinal hernia affects ~27% of Indian men at some point in their lives — the most common surgical condition managed in rural hospitals
- Abdominal examination uses regions and quadrants to localise every abdominal complaint — you cannot document or communicate a clinical finding without them
- Abdominal incisions — every abdominal operation begins by cutting through these layers; your knowledge predicts the surgeon's choices and the patient's recovery
- Umbilical and epigastric hernias are common in multiparous Indian women and obese patients
- Laparoscopic port placement — understanding the deep epigastric vessels prevents catastrophic bleeding during port insertion
Cross-reference (Surgery): You will revisit these structures in your Surgery postings. The anatomy here is the foundation for every hernia repair, every laparotomy, every laparoscopic case.
RECALL
Before we proceed, anchor the new content to what you know:
From NCERT Biology (Class 11): The abdomen contains the digestive organs — stomach, small intestine, large intestine, liver, pancreas. The abdominal cavity is enclosed by muscles and the diaphragm above.
From your Osteology sessions: The abdominal wall is bounded above by the costal cartilages and xiphisternum, below by the iliac crests and inguinal ligament, and posteriorly by the lumbar vertebrae.
From General Anatomy: You know that the body is built in layers — skin → subcutaneous tissue → fascia → muscle → deep fascia → peritoneum. The anterior abdominal wall follows exactly this pattern, with three flat muscles arranged in crossing layers (like plywood) for maximum strength.
In this module, we add precise anatomy, clinical correlations, and the surgical implications that make the difference between a competent and an excellent clinician.
Part 1: Planes, Regions, and Quadrants of the Abdomen (AN44.1)
The abdomen is divided into regions and quadrants to localise pain, organise examination, and document findings — every patient encounter with abdominal complaints begins here.

Figure: Part 1: Planes, Regions, and Quadrants of the Abdomen (AN44.1)
Four Quadrants (clinical standard):
Two lines cross at the umbilicus: a vertical midline + a horizontal transumbilical line.
| Quadrant | Abbreviation | Key contents |
|---|---|---|
| Right upper quadrant | RUQ | Liver (right lobe), gallbladder, right kidney, hepatic flexure of colon |
| Left upper quadrant | LUQ | Stomach, spleen, left kidney, splenic flexure of colon, tail of pancreas |
| Right lower quadrant | RLQ | Appendix, caecum, ascending colon, right ureter, right ovary/fallopian tube |
| Left lower quadrant | LLQ | Sigmoid colon, left ureter, left ovary/fallopian tube |
| Central (periumbilical) | — | Small intestine, aorta, umbilical region |
Nine Regions (academic/surgical):
Two vertical lines (lateral, along the lateral edges of rectus abdominis) + two horizontal lines (subcostal plane at L1 and intertubercular/transtubercular plane at L5) divide the abdomen into 3×3 = 9 regions:
| Row | Left | Centre | Right |
|---|---|---|---|
| Upper | Left hypochondrium (spleen) | Epigastrium (stomach, liver) | Right hypochondrium (liver) |
| Middle | Left lumbar (descending colon) | Umbilical (small bowel, aorta) | Right lumbar (ascending colon) |
| Lower | Left iliac fossa (sigmoid colon) | Hypogastrium/pubic (bladder, uterus) | Right iliac fossa (appendix, caecum) |
Key Planes:
- Transpyloric plane (L1): Midway between the suprasternal notch and pubic symphysis. Passes through the pylorus of the stomach, the neck of the pancreas, the origin of the superior mesenteric artery, the hilum of both kidneys, and the fundus of the gallbladder — the most clinically packed single plane in the abdomen.
- Subcostal plane (L3): Below the lowest costal cartilage (10th rib).
- Intertubercular/transtubercular plane (L5): Connects the tubercles of the iliac crests.
- Interiliac plane: Connects the iliac crests (at L4 — used for lumbar puncture landmark).
Midlines:
- Linea alba — fibrous band from xiphisternum to pubic symphysis, formed by the fusion of the aponeuroses of the three flat abdominal muscles. Relatively avascular → preferred midline incision site.
- Linea semilunaris — curved line lateral to the rectus abdominis, marking its lateral edge.
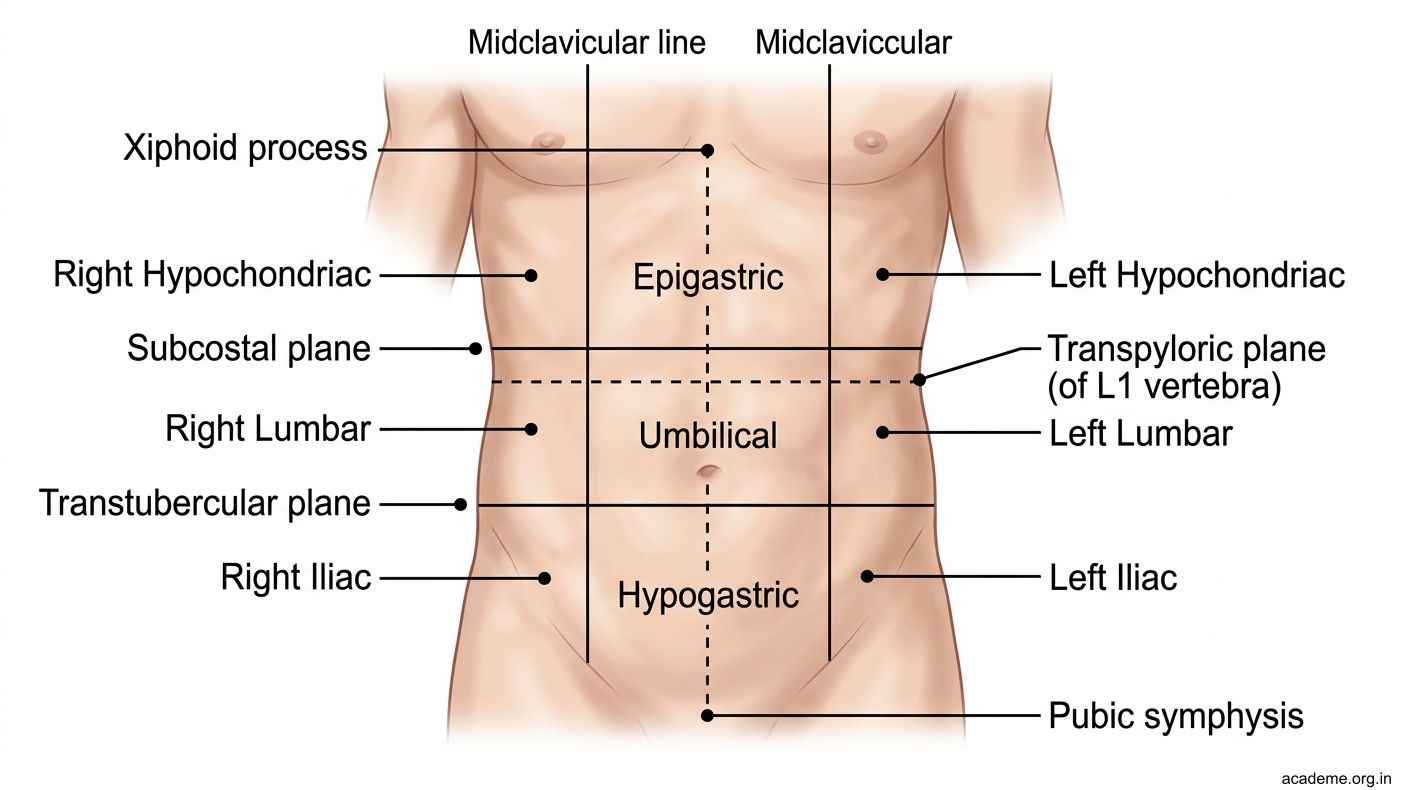
Figure: Part 1: Planes, Regions, and Quadrants of the Abdomen (AN44.1)
Part 2: Muscles and Fascia of the Anterior Abdominal Wall (AN44.6, AN44.2)
The anterior abdominal wall has five muscles — three flat muscles arranged in crossing layers laterally, and two vertical muscles centrally:
Flat muscles (lateral, from superficial to deep):
| Muscle | Origin | Insertion | Fibre direction | Action |
|---|---|---|---|---|
| External oblique | Lower 8 ribs (5–12), outer surface | Linea alba, inguinal ligament, pubic tubercle, anterior iliac crest | Downward and medially (like hands in pockets) | Compresses abdomen; bilateral = trunk flexion; unilateral = ipsilateral side flexion + contralateral rotation |
| Internal oblique | Thoracolumbar fascia, iliac crest, lateral inguinal ligament | Costal margin (ribs 10–12), linea alba, pubic crest | Upward and medially (perpendicular to EO) | Similar to EO but unilateral = ipsilateral rotation |
| Transversus abdominis | Thoracolumbar fascia, iliac crest, lateral inguinal ligament, lower 6 costal cartilages | Linea alba, pubic crest, pubic pecten | Horizontal | Pure abdominal compression — the main muscle of the "Valsalva" (cough, sneeze, defecation, micturition, parturition) |
Vertical muscles (central):
- Rectus abdominis: Two parallel muscles separated by the linea alba. Origin: pubic symphysis and pubic crest. Insertion: xiphisternum, 5th–7th costal cartilages. Action: trunk flexion, expiration. Interrupted by 3–4 tendinous intersections (attached to the anterior rectus sheath only — this is why sit-ups cause a "six pack" appearance). The muscle belly is enclosed in the rectus sheath (described in Part 3).
- Pyramidalis (present in ~80% of people): Small triangular muscle anterior to rectus at its lower end. Origin: pubic body. Insertion: linea alba. Action: tensions the linea alba.
Fascial layers (superficial to deep):
1. Camper's fascia — fatty superficial fascia (continuous with general subcutaneous fat)
2. Scarpa's fascia — membranous deep layer of superficial fascia (fused with fascia lata of thigh below inguinal ligament but continuous over the scrotum/penis as Colles' fascia/dartos fascia). Clinical: Urine extravasation (from urethral injury) is confined by Scarpa's fascia — spreads under Scarpa's fascia into the scrotum, perineum, and up to the umbilical region but not into the thigh.
3. External oblique aponeurosis (investing fascia of the muscle beneath)
4. Transversalis fascia — the innermost layer, lining the transversus abdominis from inside; important in hernia mechanics.
Nerves of the anterior abdominal wall:
- Thoracoabdominal nerves (T7–T11): anterior rami of lower intercostal nerves; supply muscles and skin in bands
- Subcostal nerve (T12)
- Ilioinguinal nerve (L1): passes through the inguinal canal, exits the superficial inguinal ring → supplies skin of the upper scrotum/labia majora and adjacent medial thigh
- Iliohypogastric nerve (L1): pierces the internal oblique → sensory to suprapubic skin
Blood vessels:
- Superior epigastric artery (from internal thoracic) — enters rectus sheath above; anastomoses with inferior epigastric
- Inferior epigastric artery (from external iliac) — enters rectus sheath below; lies medial to the deep inguinal ring; forms the lateral border of Hesselbach's triangle
- Deep circumflex iliac artery (from external iliac) — runs along iliac crest

Figure: Part 2: Muscles and Fascia of the Anterior Abdominal Wall (AN44.6, AN44.2)

Figure: Flat muscles (lateral, from superficial to deep):
CLINICAL PEARL
The three flat muscles of the lateral abdominal wall are arranged so their fibres cross each other — external oblique runs obliquely downward, internal oblique runs obliquely upward, and transversus runs horizontally. This arrangement (like plywood layers) means the wall is mechanically stronger than any single muscle — a stab wound must cut through fibres running in three different directions to penetrate.
In Indian hospitals treating trauma, this anatomy explains why an apparent "deep" lateral stab wound may not have entered the peritoneum — the crossing fibres can deflect a blade. A midline stab wound is more dangerous because it only crosses the avascular linea alba (no muscle), making it a single-layer penetration.
Surgical note: When surgeons close an abdominal wound, they close each layer separately — transversalis fascia first, then muscle, then fascia. Failure to close each layer invites incisional hernia.
SELF-CHECK
Which plane passes through the pylorus of the stomach, the neck of the pancreas, and the hilum of both kidneys?
A. Subcostal plane
B. Transpyloric plane (of Addison)
C. Intertubercular plane
D. Interiliac plane
Reveal Answer
Answer: B. Transpyloric plane (of Addison)
The linea alba is formed by the fusion of the aponeuroses of which muscles?
A. Rectus abdominis (bilateral)
B. External oblique + internal oblique + transversus abdominis
C. Internal oblique + transversus abdominis only
D. External oblique only
Reveal Answer
Answer: B. External oblique + internal oblique + transversus abdominis
Part 3: The Rectus Sheath — An Anatomical Engineering Masterpiece (AN44.3)
The rectus sheath is a fibrous compartment formed by the aponeuroses of the three flat abdominal muscles (external oblique, internal oblique, transversus abdominis). Its formation changes at a critical point — the arcuate line (linea semicircularis) — located approximately one-third of the distance between the umbilicus and the pubic symphysis (roughly 3–4 cm below the umbilicus).

Figure: Part 3: The Rectus Sheath — An Anatomical Engineering Masterpiece (AN44.3)
Above the arcuate line:
- Anterior wall: External oblique aponeurosis + anterior lamella of internal oblique aponeurosis
- Posterior wall: Posterior lamella of internal oblique aponeurosis + transversus abdominis aponeurosis + transversalis fascia
The internal oblique aponeurosis splits at the lateral edge of rectus and reunites on both sides — hence it contributes to both anterior and posterior walls.
Below the arcuate line:
- Anterior wall: ALL three aponeuroses pass anterior to rectus — EO + IO + TA (undivided)
- Posterior wall: Only transversalis fascia (no aponeurosis)
Why? Below the arcuate line, all aponeuroses migrate anteriorly, leaving the posterior rectus unprotected by aponeurosis. This creates a potential weakness at the lower rectus — explains why lower abdominal surgery dehiscence is more common.
Contents of the rectus sheath:
1. Rectus abdominis muscle
2. Pyramidalis (where present)
3. Superior and inferior epigastric vessels (and their anastomosis)
4. Terminal branches of the lower 5 intercostal and subcostal nerves (T7–T12) — enter the sheath laterally
5. Tendinous intersections of rectus (attached to the anterior wall only, not posterior wall — hence rectus is freely mobile posteriorly)
Clinical significance — Rectus sheath haematoma:
The inferior epigastric artery runs posterior to the rectus above the arcuate line and anterior below. Sudden violent contraction (coughing paroxysm in a patient with whooping cough, or anticoagulant therapy) can rupture this vessel → haematoma confined within the sheath → tender pulsatile mass. On ultrasound, it respects the midline (stays within the sheath boundary). Fothergill's sign: a tender abdominal mass that remains palpable when the patient tenses the abdominal muscles (distinguishes rectus sheath haematoma from intraperitoneal mass, which becomes impalpable with muscle contraction).
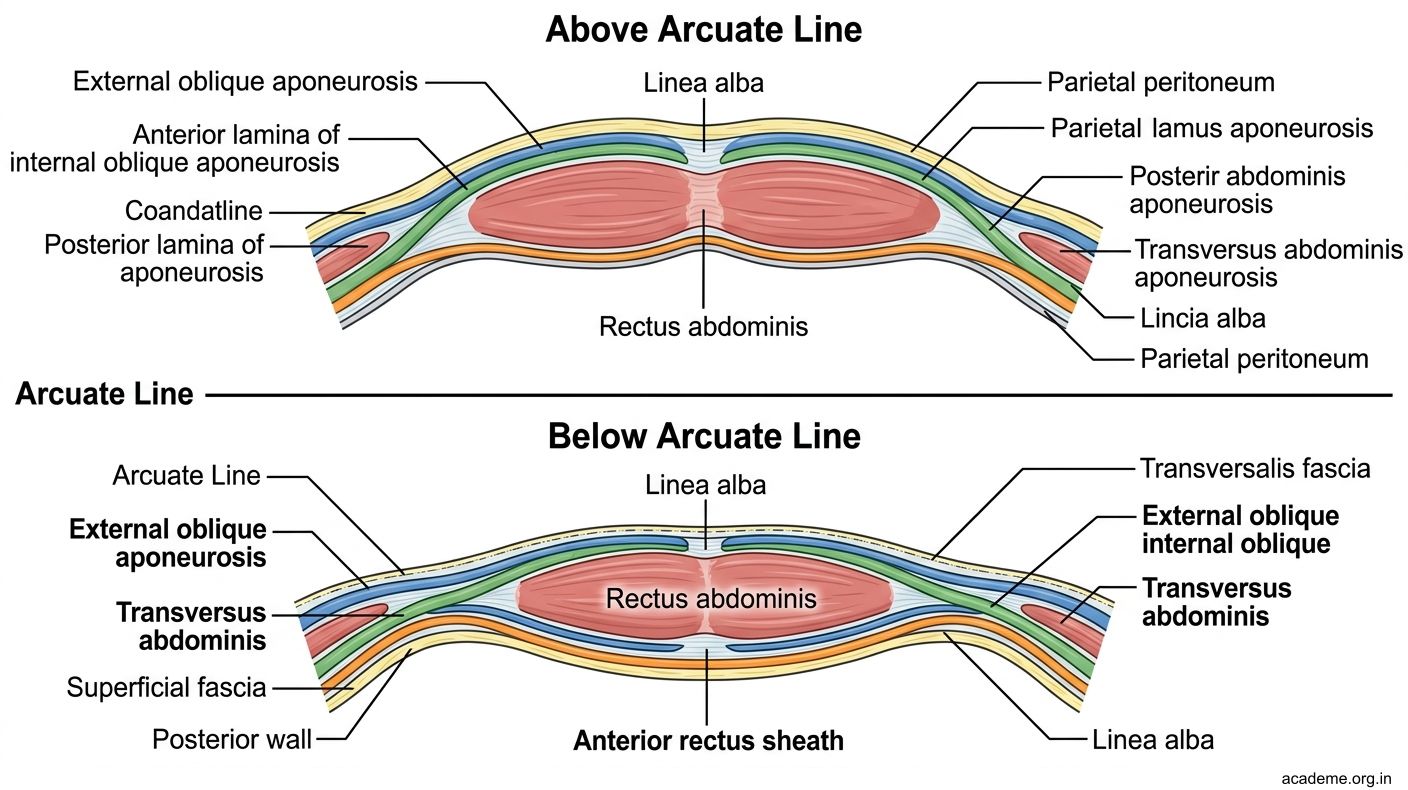
Figure: Part 3: The Rectus Sheath — An Anatomical Engineering Masterpiece (AN44.3)