Page 1 of 4
AN45.1-3 | Posterior abdominal wall — SDL Guide
The posterior abdominal wall forms the back of the abdominal cavity and is bounded posteriorly by the lumbar vertebrae and intervertebral discs. It houses major vessels (aorta, IVC), the retroperitoneal organs (kidneys, ureters, adrenals), and gives origin to the lumbar plexus that supplies the lower limb. In this module you will master the thoracolumbar fascia and its clinical relevance, the back muscles and their nerve supply, and the lumbar plexus with its branches and clinical significance.
Learning Outcomes
- Describe the layers, attachments, and clinical significance of the thoracolumbar fascia (AN45.1)
- Describe the lumbar plexus — root values, formation, branches, and clinical anatomy of injury (AN45.2)
- Describe the back muscles (erector spinae group), their nerve supply, and actions (AN45.3)
PREREQUISITES
Knowledge of lumbar vertebra anatomy and the general plan of a spinal nerve is essential. Review the dermatomes of the lower limb before studying the lumbar plexus.
References
- Gray's Anatomy for Students — Posterior Abdominal Wall (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 2 — Back muscles and lumbar plexus (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy | ~35 min
CLINICAL SCENARIO
A 42-year-old software engineer in Bengaluru presents to the outpatient with low back pain for 6 months. Recently he developed shooting pain down the left leg to the big toe, and weakness of left great toe extension. An MRI shows a left L4–L5 posterolateral disc prolapse.
Which nerve root is compressed? What muscles are weak? Where exactly does the pain radiate? Why do the symptoms go to the big toe specifically?
Understanding the lumbar plexus and the back muscles is not just anatomy — it is the foundation of the neurological examination of the lower limb, one of the most common clinical assessments in medicine.
WHY THIS MATTERS
The posterior abdominal wall structures are clinically ubiquitous:
- Low back pain affects 60–80% of Indians at some point in their lives — the most common cause of work disability after headache. The thoracolumbar fascia and erector spinae are central to this.
- Lumbar disc prolapse causes L4, L5, or S1 radiculopathy in millions of Indians — you need lumbar plexus anatomy to localise the level clinically.
- Femoral nerve injury from retroperitoneal haematoma (after cardiac catheterisation via femoral artery) causes quadriceps weakness — a common iatrogenic complication you must recognise.
- Meralgia paraesthetica (lateral femoral cutaneous nerve compression) is extraordinarily common in overweight individuals and pregnant women in India.
- Psoas abscess (TB of lumbar vertebrae — Pott's disease) tracks along the psoas sheath to the femoral triangle — understanding the anatomy predicts the presentation.
RECALL
Before we begin, anchor the new content:
From Osteology: The lumbar vertebrae (L1–L5) have large vertebral bodies, no costal facets, and transverse processes that are actually modified ribs (costal elements). The intervertebral foramina transmit the spinal nerve roots.
From General Anatomy: A typical spinal nerve has a dorsal root (sensory) + ventral root (motor). The anterior primary rami of L1–L4 form the lumbar plexus. You know that the femoral nerve supplies the anterior thigh and the obturator nerve supplies the medial thigh.
From Clinical context: You have heard of "slipped disc" and "sciatica." The lumbar plexus anatomy explains these precisely.
Part 1: Thoracolumbar Fascia (AN45.1)
The thoracolumbar fascia (TLF) is a complex multilayered fascial envelope enclosing the extensor muscles of the back. It extends from the thoracic region to the sacrum and is especially well-developed (and clinically important) in the lumbar region, where it has three distinct layers:

Figure: Part 1: Thoracolumbar Fascia (AN45.1)
Three layers in the lumbar region:
1. Posterior layer — behind the erector spinae; attached medially to the spinous processes and supraspinous ligaments. Laterally, it fuses with the middle layer to form the lateral raphe (at the lateral margin of erector spinae), where the internal oblique and transversus abdominis aponeuroses attach.
2. Middle layer — between erector spinae (posterior) and quadratus lumborum (anterior); attached medially to the transverse processes of lumbar vertebrae and the intertransverse ligaments.
3. Anterior layer — anterior to quadratus lumborum; attached to the anterior surfaces of lumbar transverse processes.
In the thoracic region, only the posterior layer is distinct (covering the erector spinae); the other layers are thin.
Clinical significance:
1. Muscle compartment: The posterior and middle layers form a closed osteofascial compartment for the erector spinae. Swelling within this compartment (haematoma, abscess) compresses the muscles.
2. Attachment for abdominal muscles: The TLF is the origin of transversus abdominis, internal oblique, and latissimus dorsi — it is the structural link between the posterior wall and the anterolateral wall.
3. Tensegrity of the spine: The TLF, under tension from the attached muscles (especially TA), provides "hydraulic amplification" of spinal loading — an important concept in core stability rehabilitation.
4. TB/Psoas abscess: Pott's disease (TB of lower thoracic/lumbar vertebrae) causes a cold abscess that tracks along the psoas fascia (an extension of the anterior TLF) down to the femoral triangle, presenting as a fluctuant groin swelling.
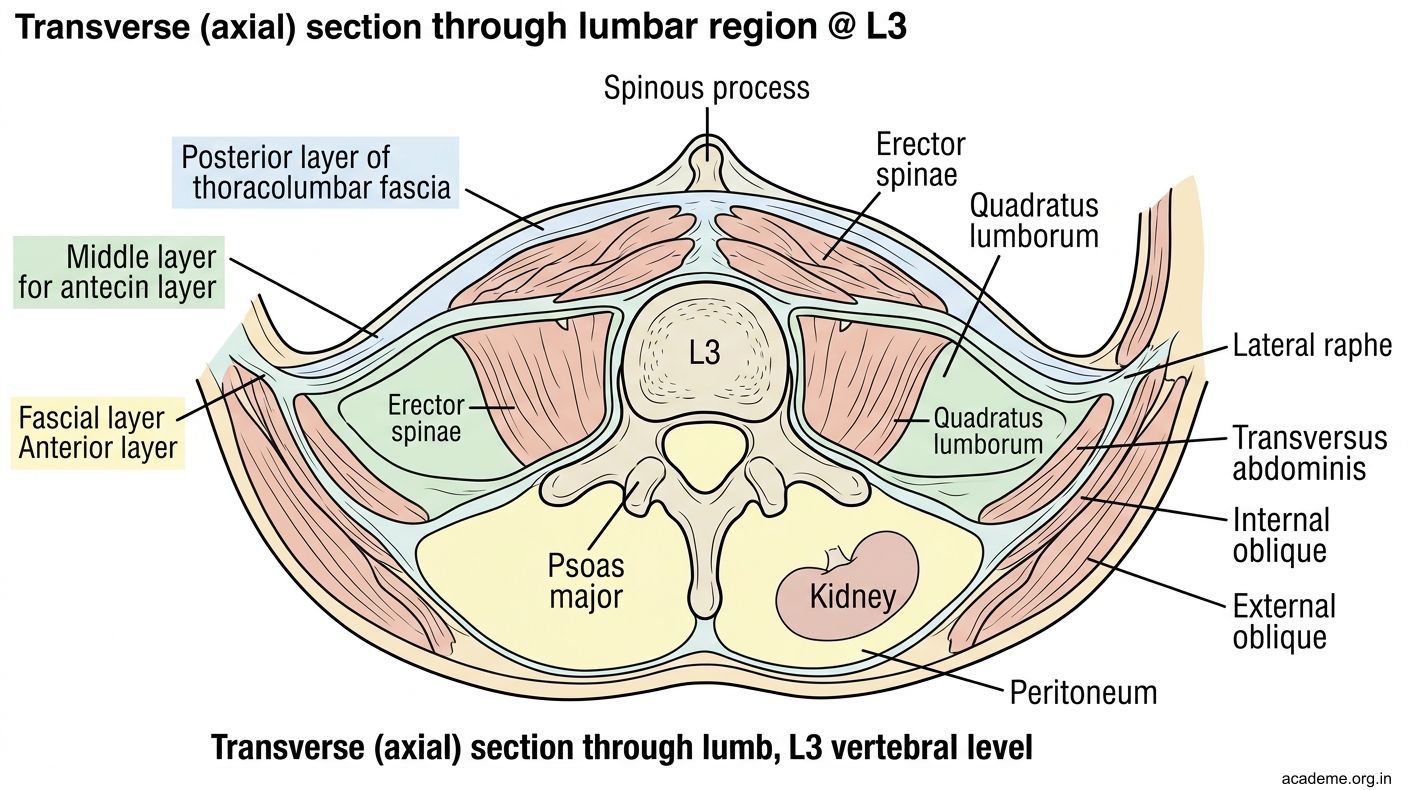
Figure: Part 1: Thoracolumbar Fascia (AN45.1)
Part 2: Back Muscles — Erector Spinae and Deep Back Muscles (AN45.3)
The back muscles responsible for extending and stabilising the vertebral column are enclosed in the osteofascial compartment of the thoracolumbar fascia.
Erector spinae (sacrospinalis) — the main extensor column:
A large muscular mass arising from the sacrum, iliac crest, and lumbar spinous processes. It divides in the lumbar region into three columns (medial to lateral):
| Column | Name | Attachments |
|---|---|---|
| Medial | Spinalis | Spinous processes to spinous processes |
| Middle | Longissimus | Transverse processes + ribs (largest, most powerful) |
| Lateral | Iliocostalis | Ribs to ribs (most lateral) |
Mnemonic: "I Love Sitting" — Iliocostalis, Longissimus, Spinalis (lateral to medial).
Nerve supply: All erector spinae muscles are supplied by the dorsal (posterior) primary rami of spinal nerves at each segmental level. This segmental supply means the muscle cannot be paralysed by a single nerve injury — complete paralysis requires multiple root lesions.
Actions of erector spinae:
- Bilateral contraction: extension of the vertebral column; antigravity posture
- Unilateral contraction: lateral flexion to the same side
Deep (intrinsic) back muscles — the Transversospinalis group:
Deep to erector spinae; fibres run obliquely upward and medially from transverse to spinous processes:
- Semispinalis — spans 4–6 segments; well-developed in the thoracic region
- Multifidus — spans 2–4 segments; most developed in the lumbar region. Critical in core stability; atrophies selectively ipsilateral to a painful disc lesion — hence physiotherapy targets multifidus rehabilitation.
- Rotatores — span 1–2 segments; richest in proprioceptive nerve endings (joint position sense for the spine)
Suboccipital muscles (upper cervical):
Four small muscles deep to the trapezius/semispinalis at the occiput-C1-C2 level (rectus capitis posterior major/minor, obliquus capitis superior/inferior). Supply: suboccipital nerve (dorsal ramus C1). Function: fine movements and proprioception of the head.

Figure: Part 2: Back Muscles — Erector Spinae and Deep Back Muscles (AN45.3)
Part 3: Lumbar Plexus — Formation, Branches, and Clinical Anatomy (AN45.2)
The lumbar plexus is formed by the anterior primary rami of L1, L2, L3, and most of L4 within the substance of the psoas major muscle (between its anterior and posterior slips). It supplies the anterior and medial compartments of the thigh.
Formation:
- L1 → iliohypogastric + ilioinguinal nerves (emerge from lateral border of psoas)
- L1 + L2 → genitofemoral nerve (emerges through anterior surface of psoas at L3–L4)
- L2 + L3 → lateral femoral cutaneous nerve (LFCN — emerges lateral border of psoas, crosses iliacus, exits under the inguinal ligament medial to ASIS)
- L2, L3, L4 (posterior divisions) → femoral nerve (largest branch; emerges lateral border of psoas, passes through muscular lacuna under inguinal ligament)
- L2, L3, L4 (anterior divisions) → obturator nerve (emerges medial border of psoas at pelvic brim, passes through obturator foramen)
- L4 + L5 → lumbosacral trunk (joins sacral plexus; forms the sciatic nerve with S1–S3)
Key branches and clinical anatomy:
| Nerve | Root | Motor | Sensory | Clinical significance |
|---|---|---|---|---|
| Femoral | L2,3,4 | Quadriceps femoris, sartorius, iliacus | Anterior + medial thigh, medial leg (saphenous nerve) | Femoral nerve palsy: foot lifts off the ground but cannot extend knee; absent knee jerk. Causes: retroperitoneal haematoma, femoral artery catheterisation, psoas abscess |
| Obturator | L2,3,4 | Adductors of thigh | Medial thigh | Obturator nerve palsy: weakness of adduction; pain spreading down medial thigh. Obturator hernia may compress it → pain radiating to medial thigh (Howship-Romberg sign). |
| Lateral femoral cutaneous | L2,3 | None (purely sensory) | Lateral thigh | Meralgia paraesthetica: compression under inguinal ligament near ASIS → burning/tingling lateral thigh. Commonest in pregnant women and obese patients in India. |
| Genitofemoral | L1,2 | Cremaster muscle (genital branch) | Upper anterior thigh (femoral branch), scrotum/labia majora (genital branch) | Cremasteric reflex is mediated by genitofemoral nerve; absent in testicular torsion and upper motor neuron lesions. |
| Ilioinguinal | L1 | None in adults | Scrotum/labia majora, upper medial thigh | Can be damaged during hernia repair → numbness of scrotum/upper thigh. |
Psoas major as a landmark:
- The lumbar plexus forms within the psoas and its nerves emerge at predictable borders
- The femoral nerve lies in the groove between psoas and iliacus (iliacus compartment)
- A psoas abscess (TB Pott's disease) directly compresses lumbar plexus roots

Figure: Part 3: Lumbar Plexus — Formation, Branches, and Clinical Anatomy (AN45.2)

Figure: Key branches and clinical anatomy:

Figure: Module Summary — Posterior Abdominal Wall
CLINICAL PEARL
Meralgia paraesthetica (from Greek meros = thigh, algos = pain) is compression of the lateral femoral cutaneous nerve (L2,3) as it passes under the inguinal ligament approximately 1 cm medial to the ASIS.
In Indian clinical practice, the three most common presentations are:
1. Pregnant women — fetal weight increases lumbar lordosis, stretching the nerve at the inguinal ligament
2. Obese patients — abdominal pannus drags on the inguinal ligament
3. Tight dhotis or trousers — external compression at the ASIS
The patient complains of burning, tingling, or numbness over the lateral thigh (L2,3 territory). Crucially, there is no motor deficit (LFCN is purely sensory) and no weakness of knee extension (femoral nerve not involved). This distinguishes it from an L2–L3 root lesion, which would affect both sensation and power.
Treatment in mild cases: weight loss, physiotherapy, avoiding tight clothing. Nerve blocks with local anaesthetic at the ASIS can provide relief. This is a condition you will diagnose in outpatient practice every week.
SELF-CHECK
Which layer of the thoracolumbar fascia attaches to the spinous processes and supraspinous ligaments?
A. Anterior layer
B. Middle layer
C. Posterior layer
D. All three layers
Reveal Answer
Answer: C. Posterior layer
A patient has burning pain and numbness over the lateral thigh with NO weakness of knee extension. Which nerve is most likely compressed?
A. Femoral nerve (L2,3,4)
B. Lateral femoral cutaneous nerve (L2,3)
C. Obturator nerve (L2,3,4)
D. Genitofemoral nerve (L1,2)
Reveal Answer
Answer: B. Lateral femoral cutaneous nerve (L2,3)
The lumbar plexus is formed within which muscle?
A. Iliacus
B. Quadratus lumborum
C. Psoas major
D. Erector spinae
Reveal Answer
Answer: C. Psoas major
REFLECT
A 35-year-old male construction worker in rural Andhra Pradesh presents with a 4-month history of low back pain that has now been joined by pain and numbness along the lateral aspect of his left thigh. He has also noticed left knee weakness when climbing stairs. MRI (done at a city hospital) shows an L2–L3 disc prolapse on the left side compressing the L3 nerve root.
- Which muscle action is primarily weakened in an L3 root compression?
- What dermatomal territory corresponds to L3?
- Would meralgia paraesthetica be in the differential? How would you clinically differentiate it from L3 root compression?
Discuss with a peer before your next tutorial.
KEY TAKEAWAYS
Module Summary — Posterior Abdominal Wall
- Thoracolumbar fascia: Three layers (posterior/middle/anterior) in lumbar region. Posterior layer → spinous processes. Middle layer → transverse processes. Anterior layer → anterior transverse processes. Abdominal muscles (TA, IO) and latissimus dorsi originate from TLF. Psoas abscess tracks in its fascial plane.
- Back muscles: Erector spinae = Spinalis (medial) + Longissimus (middle) + Iliocostalis (lateral). Nerve supply: dorsal primary rami (segmental). Deep: multifidus (core stability), semispinalis, rotatores (proprioception).
- Lumbar plexus: Forms within psoas from L1–L4. Key branches: femoral (L2,3,4 — knee extension, anterior thigh sensation), obturator (L2,3,4 — adduction, medial thigh), LFCN (L2,3 — lateral thigh, purely sensory), genitofemoral (L1,2 — cremasteric reflex), ilioinguinal (L1 — scrotum). Meralgia paraesthetica = LFCN entrapment at ASIS.