Page 1 of 4
AN46.1-5 | Male external genitalia — SDL Guide
The male external genitalia include the testis (with its coverings and descent), the epididymis, the penis, and the scrotum. A thorough understanding of testicular anatomy is essential for diagnosing and treating the two most urgent urological emergencies in young men — testicular torsion and incarcerated inguinal hernia. This module covers each structure with its applied anatomy, covering the most commonly tested conditions in final examinations and clinical practice.
Learning Outcomes
- Describe the coverings, internal structure, side determination, blood supply, nerve supply, lymphatic drainage, and descent of the testis with applied anatomy (AN46.1)
- Describe the parts and function of the epididymis (AN46.2)
- Describe the penis — parts, components, blood supply, and lymphatic drainage (AN46.3)
- Explain the anatomical basis of varicocele (AN46.4)
- Explain the anatomical basis of phimosis and circumcision (AN46.5)
PREREQUISITES
Review the inguinal canal and spermatic cord from the Anterior Abdominal Wall module. Understanding the coverings of the testis requires knowledge of the layers of the anterior abdominal wall.
References
- Gray's Anatomy for Students — Male Reproductive System (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 2 — Male Genitalia (Textbook)
- Clinically Oriented Anatomy (Moore) — Perineum chapter (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy | ~40 min
CLINICAL SCENARIO
A 19-year-old student in Vellore is woken at 3 AM by sudden, severe right scrotal pain. The testis is riding high and has a transverse lie. The cremasteric reflex is absent on the right side.
The emergency resident recognises testicular torsion and calls for emergency surgery. The testis is salvaged because it reaches theatre within 4 hours of onset.
Why does an absent cremasteric reflex point to torsion? Why does the testis ride high? Why is lymphatic drainage to the para-aortic nodes — not the inguinal nodes — clinically important in testicular cancer?
Every doctor who sees a young man with acute scrotal pain must be able to answer these questions instantly — the 4–6 hour window for testicular salvage is an anatomical story.
WHY THIS MATTERS
Male genital anatomy is clinically tested at every level of medical training:
- Testicular torsion (~1 in 4,000 males under 25) — a 4–6 hour window for salvage; missed diagnoses cost young men a testis
- Hydrocele is the most common cause of painless scrotal swelling in India — the anatomy of tunica vaginalis explains why it is translucent
- Varicocele affects 15% of all men and 40% of men attending infertility clinics — the anatomical asymmetry explains why it is almost always left-sided
- Testicular cancer — lymph drainage to para-aortic nodes (not inguinal) determines where metastases go and where to look on imaging
- Circumcision is performed on religious, cultural, and medical grounds — the anatomy determines the complications
- Erectile dysfunction — the vascular anatomy of the penis is the basis of modern ED management
RECALL
Before we proceed:
From the Anterior Abdominal Wall module: The inguinal canal contains the spermatic cord. The cord's coverings are derived from the layers of the abdominal wall (internal spermatic fascia from transversalis fascia, cremasteric from internal oblique, external spermatic fascia from external oblique aponeurosis).
From Embryology (if covered): The testis develops retroperitoneally in the posterior abdominal wall near the kidney. It descends through the inguinal canal into the scrotum guided by the gubernaculum. This descent explains why testicular vessels come from the abdominal aorta (not iliac vessels).
From NCERT Biology: The testis produces sperm (spermatogenesis at 35°C — slightly below body temperature, hence scrotal location) and testosterone.
This descent story is the key to understanding every scrotal swelling and the lymphatic drainage of the testis.
Part 1: The Testis — Coverings, Descent, and Applied Anatomy (AN46.1)
Structure of the testis:
The testis is a paired, oval organ (~5×3×3 cm) enclosed in fibrous and fascial coverings.

Figure: Part 1: The Testis — Coverings, Descent, and Applied Anatomy (AN46.1)
Internal structure:
- Tunica albuginea — dense fibrous capsule. Sends inward partitions (septa testis) dividing the testis into ~250 lobules, each containing 1–4 seminiferous tubules (where spermatogenesis occurs, at 35°C).
- Each lobule's seminiferous tubules converge → rete testis (in the mediastinum testis, a thickening of the posterior tunica albuginea) → efferent ductules → epididymis.
- Leydig (interstitial) cells between the tubules produce testosterone.
Coverings (from inside out, corresponding to abdominal wall layers):
1. Visceral layer of tunica vaginalis — reflected serous layer (peritoneum) directly on the testis
2. Parietal layer of tunica vaginalis — forms a sac; the cavity between visceral and parietal layers = potential space for hydrocele fluid
3. Internal spermatic fascia (from transversalis fascia)
4. Cremasteric muscle and fascia (from internal oblique; function: temperature regulation by raising/lowering testis)
5. External spermatic fascia (from external oblique aponeurosis)
6. Dartos muscle (smooth muscle in scrotal skin; reflex contraction in cold)
7. Scrotal skin (rugose, thin, with sebaceous glands)
Side determination (how to tell left from right testis in a cadaveric specimen):
- The epididymis is always posterior (posteromedial surface)
- The testicular artery approaches on the lateral side above
- The vas deferens ascends on the posteromedial surface → into the tail of epididymis
Testicular descent:
- Testis develops retroperitoneally near L1–L2 level (below the kidney)
- Descends from ~7th week of gestation, guided by the gubernaculum testis (a mesenchymal cord from testis to scrotum)
- Passes through the inguinal canal during the 7th–9th months of gestation (dragging its coverings)
- Normally reaches the scrotum by birth (or shortly after in premature infants)
Undescended testis (cryptorchidism): Failure to descend — most commonly arrested in the inguinal canal. If not corrected by 2 years of age → failure of spermatogenesis (higher temperature of inguinal position destroys sperm-producing cells) + 15× increased risk of testicular malignancy.
Blood supply:
- Testicular artery — directly from the abdominal aorta at L2 (because the testis developed in the abdomen). This is the embryological reason testicular vessels do NOT come from the iliac vessels.
- Venous drainage: pampiniform plexus → testicular vein → right to IVC; left to left renal vein (at a right angle, creating higher venous pressure on the left — explains left-sided varicocele predominance).
Nerve supply: Testicular plexus (T10) — visceral afferents travel with the testicular artery → pain referred to periumbilical region (T10 dermatome) in orchitis, torsion, and trauma.
Lymphatic drainage: Para-aortic (lumbar) lymph nodes at L2 level — NOT the inguinal nodes. This reflects the testis's abdominal origin. Testicular cancer metastases appear in para-aortic nodes on CT/MRI — NOT the inguinal nodes. Scrotal skin does drain to inguinal nodes — so a testicular tumour that has eroded through scrotal skin CAN eventually reach inguinal nodes.*
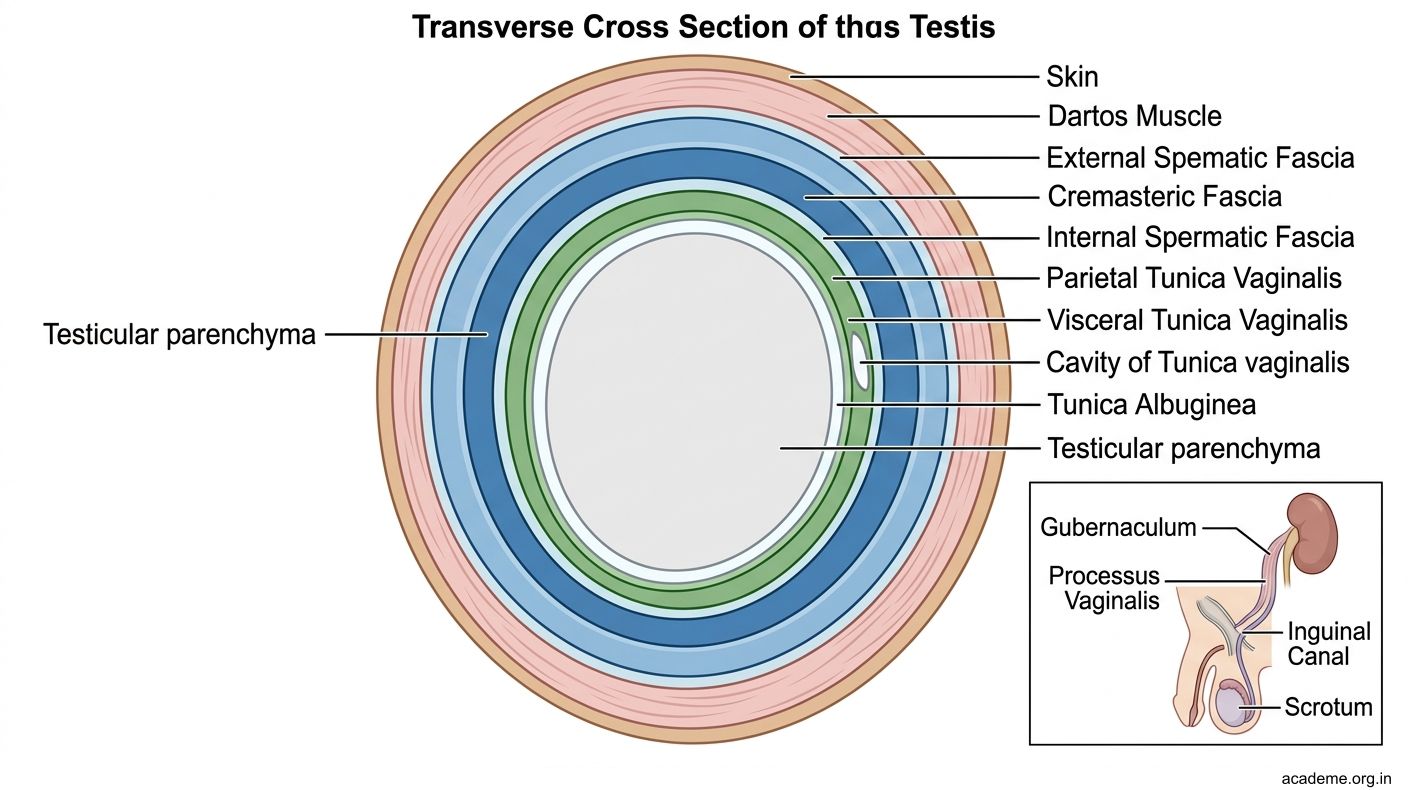
Figure: Part 1: The Testis — Coverings, Descent, and Applied Anatomy (AN46.1)
CLINICAL PEARL
Medical students consistently confuse testicular lymphatic drainage with that of the scrotum. The rule is:
- Testis → para-aortic (lumbar) nodes at L2 — because the testis developed near L2 in the fetus and dragged its lymphatics during descent
- Scrotal skin → superficial inguinal nodes
The clinical consequence: a patient with testicular cancer and no groin nodes can still have massive para-aortic lymphadenopathy. Staging CT must look at the retroperitoneum at L2 level — not the groin.
Conversely, an inguinal node metastasis from a scrotal (skin) lesion is very different from a testicular (gonadal) malignancy — different staging, different surgery, different chemotherapy.
This single anatomical fact saves patients from being understaged and undertreated.
Part 2: The Epididymis — Structure and Function (AN46.2)
The epididymis is a coiled comma-shaped structure (~7 m of coiled duct) lying along the posterolateral surface of the testis. It is the site of sperm maturation and storage.

Figure: Part 2: The Epididymis — Structure and Function (AN46.2)
Parts (head to tail):
1. Head (caput) epididymis — receives the efferent ductules from the rete testis; located at the upper pole of the testis; most prominent palpable part
2. Body (corpus) epididymis — middle portion along the posterior surface
3. Tail (cauda) epididymis — at the lower pole; becomes the vas deferens (ductus deferens)
Functions:
- Sperm maturation: Spermatozoa leaving the testis are immotile. Transit through the epididymis (~12 days) achieves full motility and fertilisation capacity.
- Storage: Mature spermatozoa stored in the tail of the epididymis await ejaculation.
- Fluid reabsorption: Reabsorbs most of the fluid from the rete testis.
Applied anatomy:
- Epididymo-orchitis: Infection of the epididymis (most common bacterial: Chlamydia trachomatis in young men, E. coli in older men). Presents as painful swelling of the epididymis/testis. The cremaster reflex is preserved (unlike torsion) — crucial differentiating sign.
- Appendix epididymis: A small vestigial structure at the head that can undergo torsion → localised head-of-epididymis tenderness; not an emergency.
- Vasectomy is performed on the vas deferens (not the epididymis) — the vas is palpable through the scrotal skin at its lower pole.
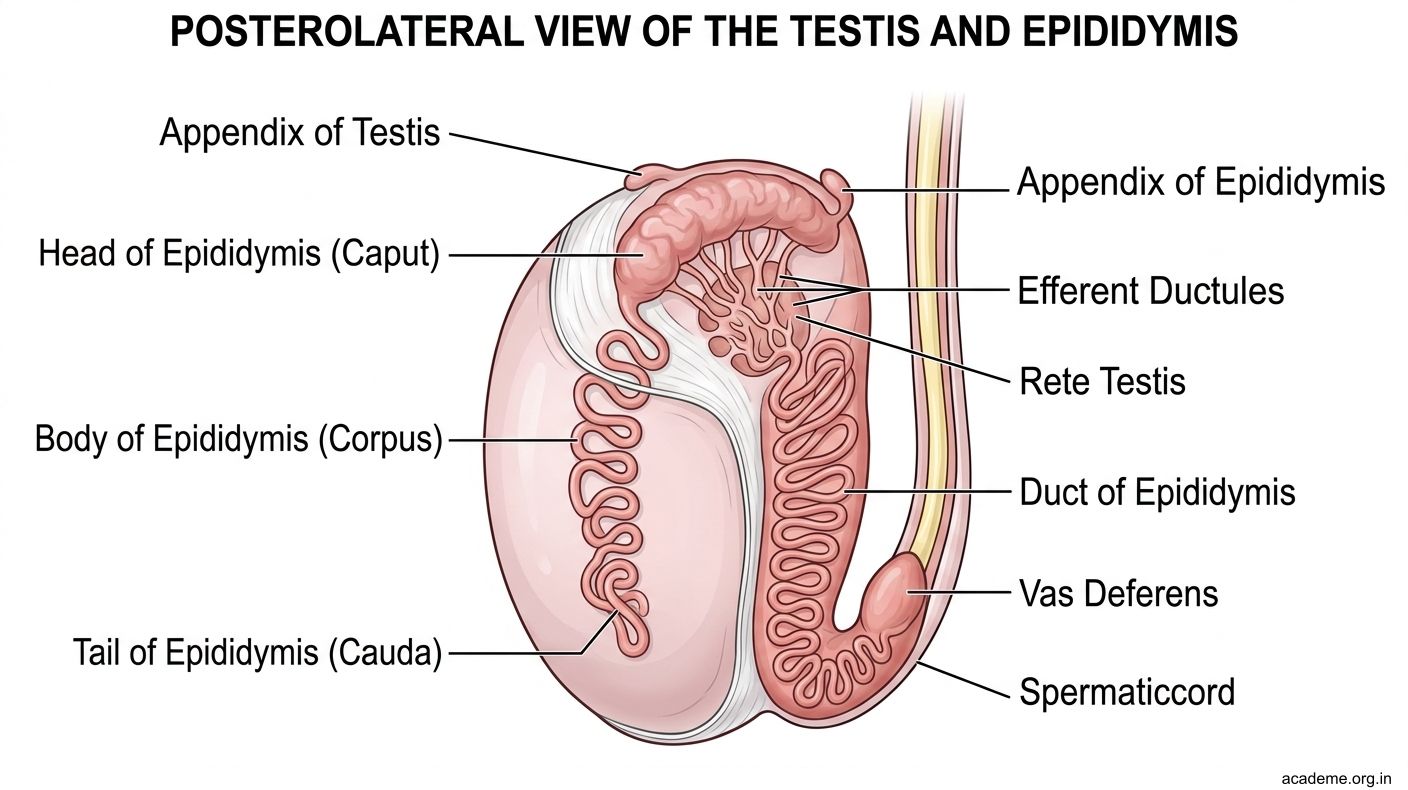
Figure: Part 2: The Epididymis — Structure and Function (AN46.2)
Part 3: The Penis — Parts, Components, and Blood Supply (AN46.3)
The penis has three cylindrical bodies of erectile tissue:

Figure: Part 3: The Penis — Parts, Components, and Blood Supply (AN46.3)
Three erectile bodies:
1. Two corpora cavernosa — paired, lie side by side dorsally; each surrounded by a tough fibrous tunica albuginea; joined by an incomplete median septum. End blindly at the glans.
2. One corpus spongiosum — single, ventral; surrounds the penile urethra; expands distally to form the glans penis (covered by the prepuce/foreskin); expands proximally as the bulb of the penis (fixed to the perineal membrane).
Parts of the penis:
- Root (fixed part): Two crura (singular: crus) attached to the ischiopubic rami + bulb attached to the perineal membrane + ischiocavernosus (over crura) + bulbospongiosus (over bulb) muscles.
- Body (shaft): Free cylindrical part; skin + subcutaneous tissue (no fat in penile skin) + Buck's (deep penile) fascia + dartos fascia + 3 erectile bodies.
- Glans penis: Expanded distal end of corpus spongiosum; bears the external urethral meatus.
Blood supply:
- Dorsal artery of the penis (branch of internal pudendal artery) — supplies glans and skin
- Deep artery of the penis (branch of internal pudendal) — enters the corpus cavernosum → helicine arteries open into cavernous spaces during erection
- Artery to the bulb — supplies the bulb (corpus spongiosum proximally) and the bulbourethral glands
Erection mechanism: Parasympathetic (S2,3,4 via pelvic splanchnic nerves / nervi erigentes) → relaxation of smooth muscle of helicine arteries → blood fills cavernous spaces → compresses emissary veins against tunica albuginea → veno-occlusion → erection maintained.
Lymphatic drainage:
- Prepuce, scrotal skin, shaft skin → superficial inguinal nodes
- Glans penis → deep inguinal nodes → external iliac nodes
- Carcinoma of the glans presents with inguinal lymphadenopathy.
Dorsal nerve of the penis (S2,3) — sensory to the glans; the nerve blocked in penile nerve block for circumcision.
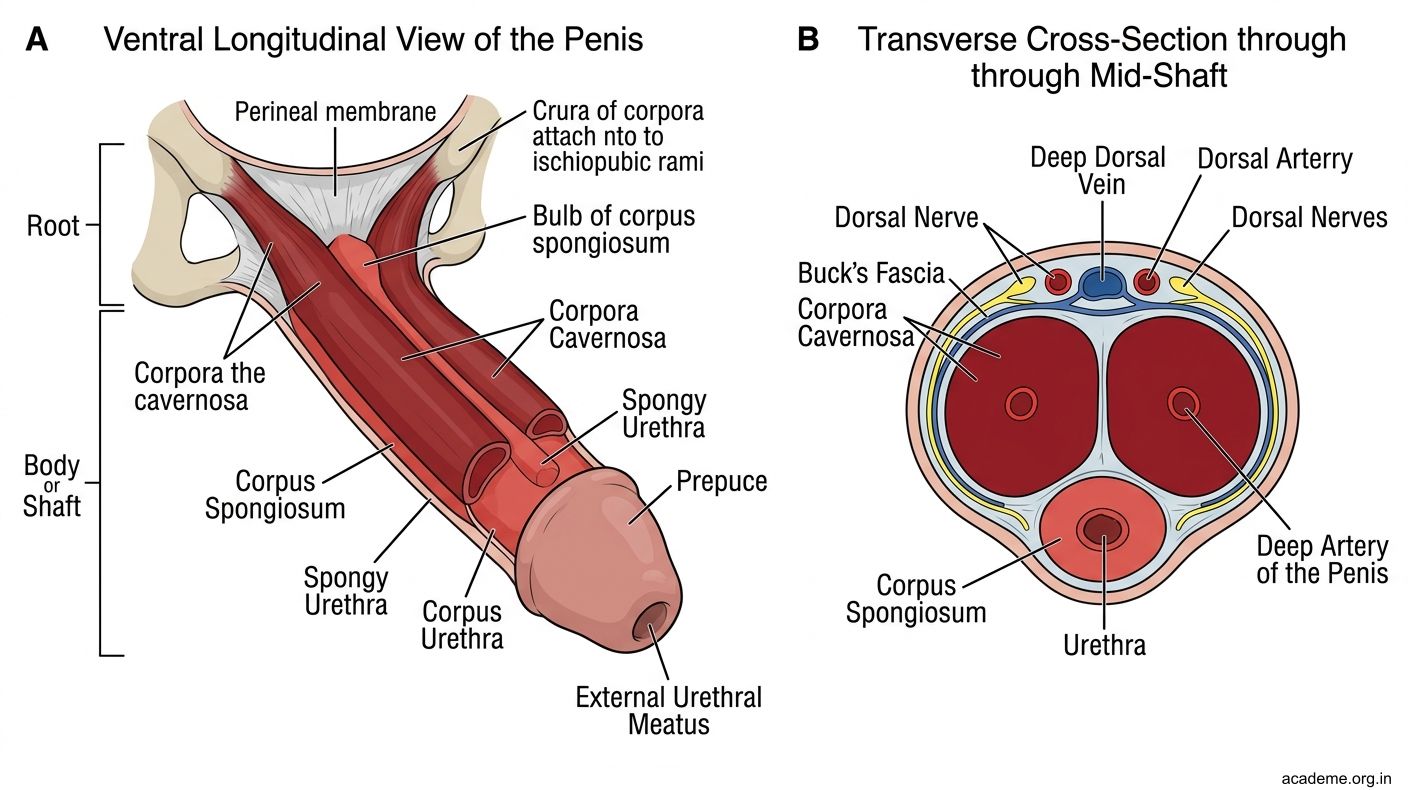
Figure: Part 3: The Penis — Parts, Components, and Blood Supply (AN46.3)
Part 4: Varicocele and Phimosis — Anatomical Basis (AN46.4, AN46.5)
Varicocele (AN46.4):
A varicocele is an abnormal dilatation of the pampiniform plexus of veins within the spermatic cord — like varicose veins of the scrotum.
Anatomical basis of left-sided predominance (90% of varicoceles are on the left):
- Left testicular vein → left renal vein (joins at a right angle, creating high hydrostatic resistance; column of blood to the renal vein is ~10 cm longer than the right)
- Right testicular vein → IVC directly (at an oblique angle, lower resistance)
The left testicular vein effectively has a higher venous pressure → valves in the left testicular vein fail → retrograde venous flow → dilatation of pampiniform plexus.
Why clinically important:
- Raised scrotal temperature (venous pooling) → impaired spermatogenesis → male factor infertility (found in 40% of infertile men)
- Sudden onset left varicocele in a middle-aged man → rule out a left renal vein tumour thrombus (from renal cell carcinoma) obstructing the left renal vein
- Right-sided varicocele is uncommon and should raise suspicion of a retroperitoneal mass
Examination: "Bag of worms" feel in the left scrotum, more prominent on standing and Valsalva manoeuvre.
Phimosis and Circumcision (AN46.5):
Phimosis: The prepuce (foreskin) cannot be retracted over the glans because the preputial opening is too tight.
- Physiological phimosis: In boys under 2–3 years, the foreskin is normally non-retractile (preputial adhesions separate naturally with erections). This is NOT pathological and does NOT require treatment.
- Pathological phimosis: Acquired narrowing in older boys/men from scarring (recurrent balanitis, balanitis xerotica obliterans). Causes difficulty with urination, pain during intercourse, and inability to clean under the foreskin → recurrent infections.
Paraphimosis: Retracted foreskin that CANNOT be pulled back forward → constrictive ring cuts off venous/lymphatic return → oedema of glans and prepuce → urological emergency (manual reduction or emergency dorsal slit).
Circumcision: Surgical removal of the prepuce.
- Anatomical basis: The prepuce is a double fold of skin (inner mucosal layer + outer cutaneous layer) covering the glans. Circumcision removes this fold to the level of the corona, exposing the glans permanently.
- Nerve supply of the foreskin: Branches of the dorsal nerve of the penis (S2,3) — blocked with a penile ring block (local anaesthetic infiltrated at the base of the penis, bilaterally, dorsal and ventral) for painless circumcision.
- Complications: Haemorrhage (dorsal artery/vein of the penis), injury to the glans or urethra (rare but serious), meatal stenosis (post-circumcision scarring).

Figure: Part 4: Varicocele and Phimosis — Anatomical Basis (AN46.4, AN46.5)

Figure: Phimosis and Circumcision (AN46.5):

Figure: Module Summary — Male External Genitalia
SELF-CHECK
A 22-year-old man with a sudden right scrotal pain has a high-riding right testis and absent cremasteric reflex. What is the most likely diagnosis?
A. Epididymo-orchitis
B. Right testicular torsion
C. Hydrocele
D. Inguinal hernia
Reveal Answer
Answer: B. Right testicular torsion
Where do lymphatics from the testis drain?
A. Superficial inguinal nodes
B. Deep inguinal nodes
C. Para-aortic (lumbar) nodes at L2
D. Internal iliac nodes
Reveal Answer
Answer: C. Para-aortic (lumbar) nodes at L2
Why is varicocele predominantly left-sided?
A. The left testis is more commonly undescended
B. The left testicular vein drains into the left renal vein at a right angle, creating higher venous resistance
C. The left epididymis has fewer venous valves
D. The left spermatic cord is longer than the right
Reveal Answer
Answer: B. The left testicular vein drains into the left renal vein at a right angle, creating higher venous resistance
REFLECT
Three patients are referred to a urology outpatient clinic in Chennai:
- A 17-year-old student with sudden right scrotal pain for 3 hours, high-riding testis, and absent cremasteric reflex.
- A 35-year-old man with painless "bag of worms" sensation in the left scrotum, subfertility for 2 years.
- A 55-year-old man who develops a sudden left varicocele with no prior history.
For each patient:
- What is the anatomical basis of the condition?
- What is the urgency of management?
- For patient 3 — why does a new varicocele at this age require additional investigation?
Discuss with peers before your urology tutorial.
KEY TAKEAWAYS
Module Summary — Male External Genitalia
- Testis coverings (outside-in): Skin → dartos → EsF (EO) → cremasteric (IO) → ISF (transversalis) → parietal tunica vaginalis → visceral tunica vaginalis → tunica albuginea.
- Blood supply: Testicular artery from abdominal aorta at L2 (abdominal origin). Venous: pampiniform plexus → left renal vein (right-angle, high resistance = left varicocele) vs IVC (right side).
- Lymphatics: Para-aortic at L2 (not inguinal nodes). Scrotal skin → inguinal.
- Nerve supply: Testicular plexus (T10) — referred pain to periumbilical.
- Descent: L1–L2 level → inguinal canal → scrotum; guided by gubernaculum.
- Epididymis: Head (efferent ductules) → body → tail (becomes vas deferens). Function: maturation and storage of sperm.
- Penis: Two corpora cavernosa + one corpus spongiosum (with urethra). Blood: internal pudendal → dorsal + deep arteries. Lymph: glans → deep inguinal. Erection: parasympathetic (S2,3,4), helicine arteries, veno-occlusion.
- Varicocele: 90% left-sided; left testicular vein drains to left renal vein at right angle. New left varicocele in older man → exclude renal cell carcinoma.
- Phimosis: Non-retractile foreskin. Physiological (<3 years) vs pathological. Paraphimosis = emergency.