Page 1 of 4
AN49.1-5 | Perineum — SDL Guide
Learning Objectives
- Describe and demonstrate the superficial and deep perineal pouches — boundaries and contents (AN49.1)
- Describe and identify the perineal body (AN49.2)
- Describe and demonstrate the perineal membrane in male and female (AN49.3)
- Describe and demonstrate the boundaries, contents, and applied anatomy of the ischiorectal (ischioanal) fossa (AN49.4)
- Explain the anatomical basis of perineal tear, episiotomy, perianal abscess, and anal fissure (AN49.5)
INSTRUCTIONS
Read each section carefully. The perineum is a clinically important region with direct relevance to obstetrics, urology, proctology, and surgery. Focus on the pouches, fasciae, and the ischiorectal fossa — common exam topics with important surgical implications.
References
- BD Chaurasia's Human Anatomy Vol. 2 — Perineum chapter (Textbook)
- Gray's Anatomy for Students — Perineum chapter (Textbook)
- OpenStax Anatomy and Physiology 2e — Pelvic floor and Perineum (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 26-year-old woman is in active labour in a district hospital in Puducherry. As the fetal head crowns, the obstetrician notes that the perineum is tightly stretched and about to tear. A decision is made to perform a mediolateral episiotomy.
Why is a mediolateral episiotomy preferred over a midline episiotomy in Indian obstetric practice? Which muscles does the incision cut? What structures must be protected? What is the perineal body and why is its repair critical to long-term pelvic floor function?
The perineum is the diamond-shaped region at the pelvic outlet. Despite its small size, injuries here have lifelong consequences — incontinence, prolapse, and chronic pelvic pain. A solid grasp of perineal anatomy is essential for every medical graduate in India.
WHY THIS MATTERS
Perineal anatomy is directly relevant to:
- Obstetrics: episiotomy and perineal tear repair — every obstetrician in India performs these; perineal body repair is essential for preventing prolapse and incontinence
- Colorectal surgery: perianal abscess, anal fissure, fistula-in-ano — extremely common in Indian surgical practice (up to 10% of general surgical outpatients); all require understanding of the ischiorectal fossa and anal sphincters
- Urological surgery: bulbar urethroplasty for urethral strictures — a very common operation in Indian males (high prevalence of gonococcal urethral stricture)
- Forensic medicine: examination of the perineum in cases of sexual assault — MBBS curriculum requirement
- Gynaecology: Bartholin's cyst/abscess — common; drainage is in the superficial perineal pouch region
RECALL
Before we begin, recall:
- The perineum is the diamond-shaped region at the pelvic outlet, bounded by the pubic symphysis anteriorly, coccyx posteriorly, and ischiopubic rami + sacrotuberous ligaments laterally
- A line between the two ischial tuberosities divides the perineum into the anterior urogenital triangle and posterior anal triangle
- The pelvic diaphragm (levator ani + coccygeus) forms the floor of the pelvis and the roof of the ischioanal fossa
- The pudendal nerve (S2–S4) and internal pudendal vessels supply most of the perineum — they pass through Alcock's canal in the lateral wall of the ischiorectal fossa
Perineal Membrane and Pouches (AN49.1, AN49.3)
Perineal membrane (formerly "inferior fascia of urogenital diaphragm"):
- A strong, triangular fibromuscular sheet spanning the anterior part of the pelvic outlet (attached to ischiopubic rami bilaterally)
- Present only in the urogenital triangle (not the anal triangle)
- Forms the floor of the deep perineal pouch and the roof of the superficial perineal pouch
- In males: urethra pierces it at the bulbomembranous junction; in females: urethra and vagina both pierce it
Superficial perineal pouch (between perineal membrane above and Colles' fascia/superficial perineal fascia below):
| Structure | Male | Female |
|---|---|---|
| Muscles | Superficial transverse perinei, bulbospongiosus (= bulbocavernosus), ischiocavernosus | Superficial transverse perinei, bulbospongiosus, ischiocavernosus |
| Erectile tissue | Corpus spongiosum (bulb of penis), crura of penis | Bulb of vestibule, crura of clitoris |
| Glands | — | Bartholin's (greater vestibular) glands |
| Urethra | Penile urethra (from bulb) | Terminal urethra |
Deep perineal pouch (between perineal membrane below and pelvic diaphragm above):
| Structure | Male | Female |
|---|---|---|
| Muscles | Deep transverse perinei, external urethral sphincter (EUS) | Deep transverse perinei, EUS |
| Glands | Bulbourethral (Cowper's) glands | Greater vestibular glands (variable — some sources place in superficial) |
| Vessels/nerves | Internal pudendal vessels, pudendal nerve, dorsal nerve of penis | Pudendal nerve, dorsal nerve of clitoris |
Clinical relevance — extravasation of urine in urethral rupture:
- Rupture of the urethra within the perineum (bulbar urethra, within the superficial pouch) → urine extravasates into the superficial perineal pouch
- Spreads deep to Colles' fascia into the scrotum (or labia majora) → scrotal oedema; into the anterior abdominal wall deep to Scarpa's fascia (Scarpa's fascia is continuous with Colles' fascia)
- Does NOT spread into the thigh (Colles' fascia fuses with the fascia lata at the inguinal ligament)
- Does NOT spread posteriorly (Colles' fascia fuses with perineal body and posterior edge of perineal membrane)

Figure: Perineal Membrane and Pouches (AN49.1, AN49.3)
Perineal Body (AN49.2)
Definition: The perineal body (central perineal tendon) is a fibromuscular node at the junction of the anal canal and the urogenital triangle — positioned in the midline between the anal canal and the vagina (or the bulb of the penis in males).

Figure: Perineal Body (AN49.2)
Muscles converging on it:
1. Superficial and deep transverse perinei (bilateral)
2. Bulbospongiosus
3. External anal sphincter
4. Levator ani (puborectalis, pubococcygeus)
5. Some fibres of the rectovaginal septum
Clinical importance:
- Acts as the keystone of the pelvic floor — maintains the integrity of all perineal muscles and the support of the pelvic viscera
- Perineal tear: during vaginal delivery, the perineum may tear anteroposteriorly through the perineal body
- 1st degree: skin only
- 2nd degree: skin + perineal muscles (but not anal sphincter)
- 3rd degree: extends into external anal sphincter
- 4th degree: through the anal sphincter into the anal mucosa
- Episiotomy repair: the perineal body must be reconstructed correctly to prevent long-term pelvic floor dysfunction, incontinence, and prolapse
- Rectovaginal fistula: injury to the perineal body with communication between rectum and vagina — can result from 4th-degree tear or obstetric injury
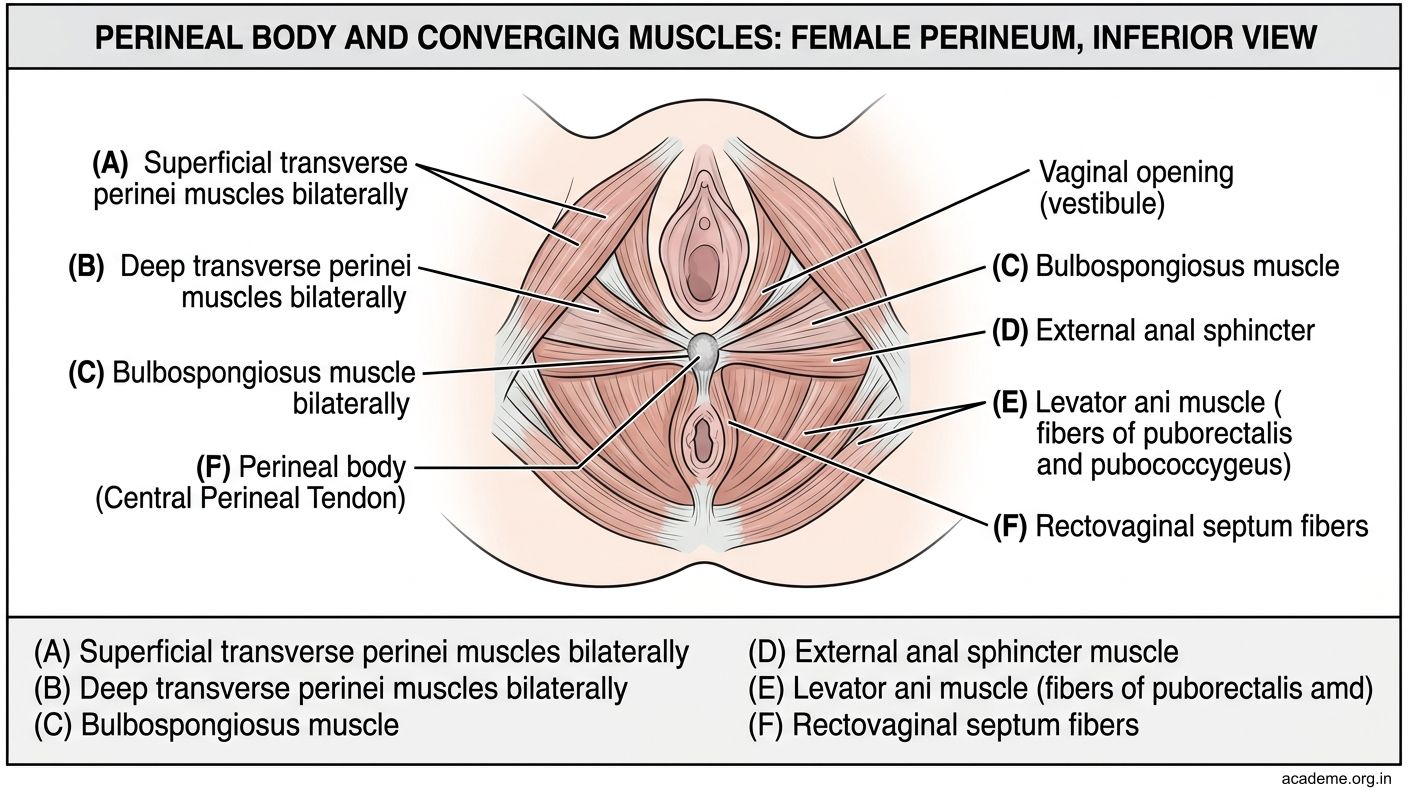
Figure: Perineal Body (AN49.2)
Ischiorectal (Ischioanal) Fossa (AN49.4)
Location: Wedge-shaped fat-filled space on either side of the anal canal, below the pelvic diaphragm.

Figure: Ischiorectal (Ischioanal) Fossa (AN49.4)
Boundaries:
| Wall | Structure |
|---|---|
| Medial | External anal sphincter + levator ani (above) |
| Lateral | Obturator internus muscle covered by its fascia (lower part); ischium and sacrotuberous ligament (below) |
| Roof | Levator ani (pelvic diaphragm — sloping) |
| Floor | Skin of perineum |
| Anterior | Posterior edge of perineal membrane (urogenital triangle) |
| Posterior | Sacrotuberous ligament; gluteus maximus |
Contents:
- Abundant fat (acts as a cushion during defaecation)
- Inferior rectal (anal) vessels and nerve (branch of internal pudendal nerve + vessels) — cross the fossa to reach the anal canal
- Pudendal nerve and internal pudendal vessels in Alcock's canal (a tunnel in the obturator fascia on the lateral wall) — the pudendal nerve supplies nearly all of the perineum
Communication: The two ischiorectal fossae communicate posteriorly via the deep postanal space (posterior to the anal canal, deep to the anococcygeal ligament). This is important because a horseshoe abscess can spread from one fossa to the other through this space.
Applied anatomy:
- Perianal abscess: most common anorectal abscess; originates in anal glands at the dentate line → tracks into the ischiorectal fossa → presents as a warm, fluctuant, exquisitely tender perianal swelling. Treatment: incision and drainage (wide saucerisation)
- Ischiorectal (ischioanal) abscess: larger; spreads laterally into the ischioanal fossa; may be bilateral (horseshoe) if infection crosses the deep postanal space
- Pudendal nerve block: anaesthetic injected into Alcock's canal (approached transvaginally or transperineally) → blocks the entire perineal region — used for episiotomy repair, forceps delivery, anal procedures
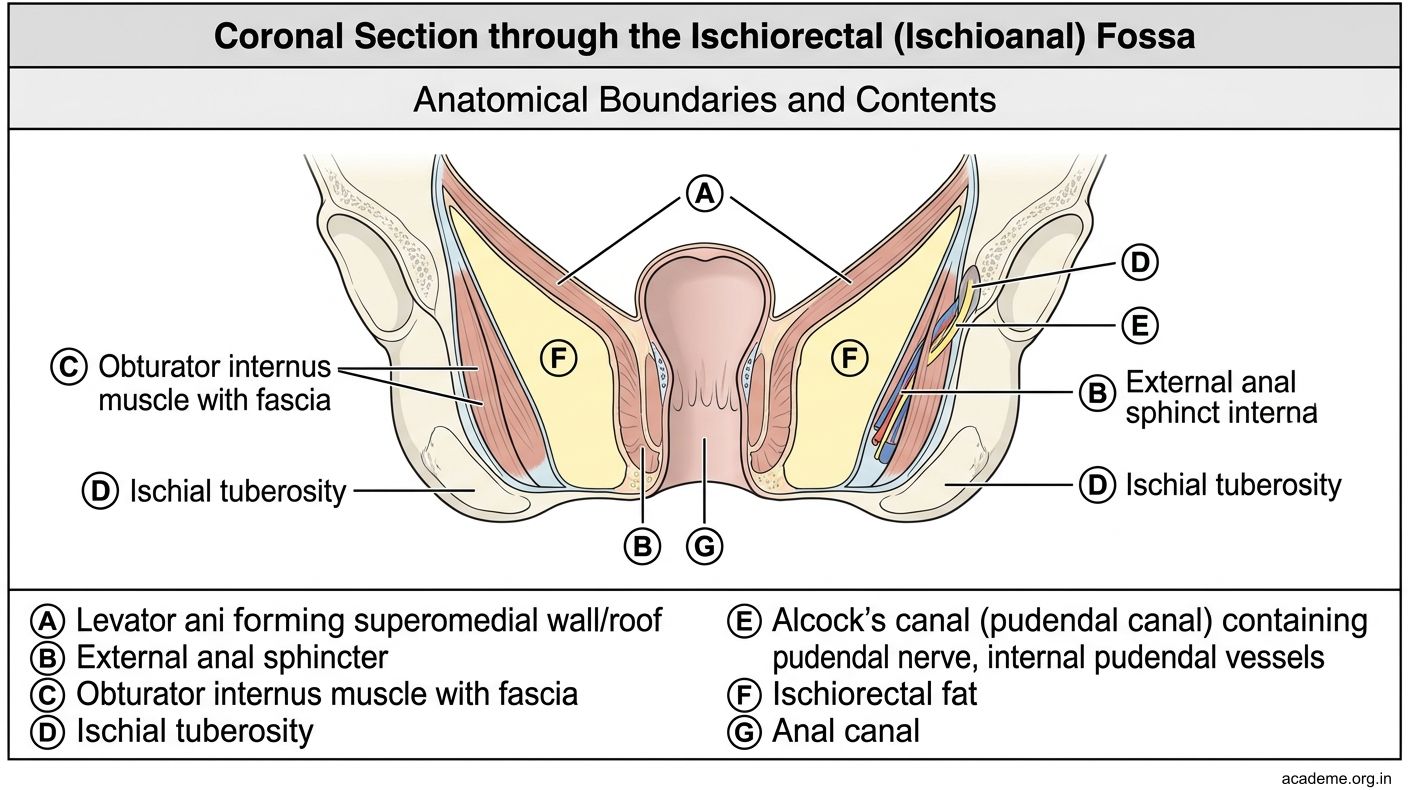
Figure: Ischiorectal (Ischioanal) Fossa (AN49.4)
Anal Fissure and Fistula-in-Ano (AN49.5)
Anal fissure:
- A longitudinal tear in the anal mucosa/skin distal to the dentate line
- Site: 90% in the posterior midline (6 o'clock position) — due to poor blood supply at the posterior commissure and tight external anal sphincter
- Symptoms: Severe pain on defaecation, bright red blood on stool/paper, sentinel pile (skin tag) at the external end
- Acute: heals with topical GTN or diltiazem (relax internal sphincter)
- Chronic: fibrosis; treated with lateral internal sphincterotomy (cuts the lower half of the internal anal sphincter → reduces spasm)
- Anatomical basis: 6 o'clock position has relatively ischaemic mucosa and highest resting sphincter pressure
Fistula-in-ano:
- An abnormal epithelialised track between the anal canal (internal opening, usually at the dentate line) and the perianal skin (external opening)
- Goodsall's rule:
- External opening anterior to the transverse anal line → track runs straight to the dentate line (direct radial track)
- External opening posterior to the line → track curves to open in the posterior midline (horseshoe track)
- Parks' classification (by relation to external anal sphincter):
- Intersphincteric (most common, ~70%): track between internal and external sphincters
- Transsphincteric: track crosses the external sphincter
- Suprasphincteric: track goes above the puborectalis
- Extrasphincteric: bypasses sphincters entirely (rare, usually due to Crohn's disease)
- Treatment: fistulotomy (open track) — risk of incontinence if large amount of sphincter involved; seton suture for high fistulae

Figure: Anal Fissure and Fistula-in-Ano (AN49.5)
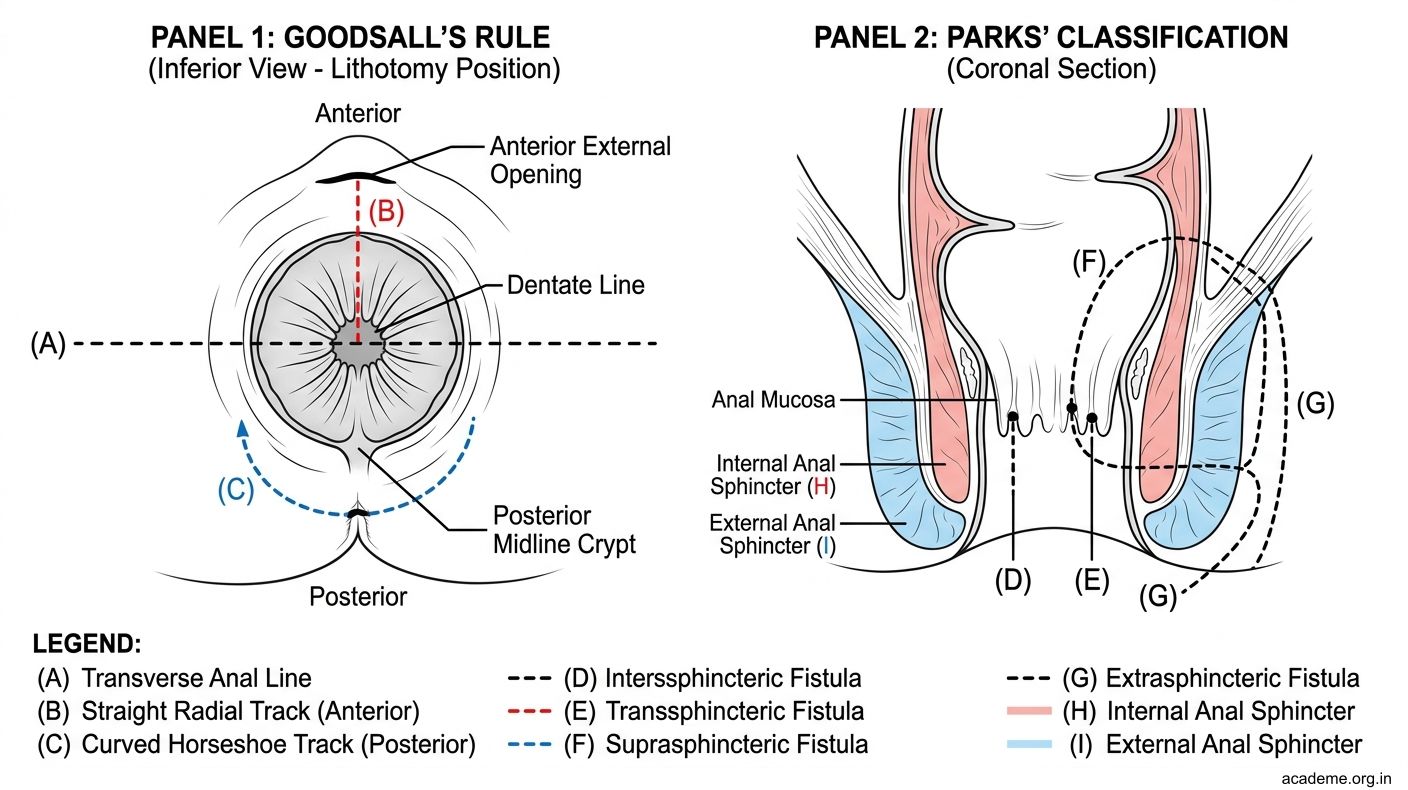
Figure: Anal Fissure and Fistula-in-Ano (AN49.5)

Figure: Episiotomy — mediolateral vs midline:

Figure: Perineum — Key Points:
SELF-CHECK
A. Thighs and gluteal region
B. Scrotum, anterior abdominal wall deep to Scarpa's fascia, and perineum (but NOT into the thighs or posterior to the ischial tuberosities)
C. Ischiorectal fossae bilaterally
D. Retroperitoneum via the deep inguinal ring
Reveal Answer
Answer: see explanation below
When the urethra ruptures within the superficial perineal pouch, urine extravasates deep to Colles' fascia. This fascia is continuous with Scarpa's fascia of the anterior abdominal wall. However, Colles' fascia is attached laterally to the fascia lata at the inguinal ligament (preventing spread to the thigh), and posteriorly to the perineal body and posterior edge of perineal membrane (preventing spread into the ischiorectal fossa or posterior). Urine can therefore track into the scrotum/labia majora and up the anterior abdominal wall.
CLINICAL PEARL
Episiotomy — mediolateral vs midline:
In Indian and UK obstetric practice, the mediolateral episiotomy is standard. It cuts from the posterior fourchette at a 45–60° angle away from the midline (toward the ischial tuberosity) — cutting through the perineal skin, superficial transverse perinei muscle, bulbospongiosus, and often part of levator ani. The purpose is to redirect the line of tearing away from the anal sphincter.
Midline episiotomy (common in the USA) gives a cleaner repair and less postoperative pain, but if it extends further (3rd/4th-degree extension), it directly injures the external anal sphincter → risk of long-term faecal incontinence.
Why is accurate repair of the perineal body critical? If the perineal body is not correctly reconstructed, the structural integrity of the pelvic floor is permanently compromised → uterine prolapse, cystocoele, rectocoele, and incontinence — conditions that disproportionately burden multiparous women in India.
REFLECT
A 45-year-old man from Chennai presents with a 1-week history of severe perianal pain and swelling. On examination, a fluctuant, exquisitely tender swelling is found on the right side of the anus.
What space is this abscess most likely in? What is the relationship of the pudendal nerve to this abscess? If the abscess is not drained and it spreads to the left side of the anus, which anatomical pathway does it take? If you need to perform a pudendal nerve block for the drainage procedure, where would you inject the local anaesthetic and why?
KEY TAKEAWAYS
Perineum — Key Points:
- Perineal membrane: strong triangular sheet in the urogenital triangle; forms floor of deep pouch and roof of superficial pouch
- Superficial perineal pouch: erectile bodies (bulb, crura), bulbospongiosus, ischiocavernosus, superficial transverse perinei, Bartholin's glands (F)
- Deep perineal pouch: deep transverse perinei, external urethral sphincter, pudendal nerve, internal pudendal vessels
- Urethral rupture extravasation: spreads deep to Colles' fascia → scrotum/labia + Scarpa's fascia (abdominal wall) — NOT to thighs or posteriorly
- Perineal body: fibromuscular keystone at the junction of the anal canal and vaginal outlet; must be repaired after perineal tears/episiotomy
- Ischiorectal fossa: fat-filled space lateral to anal canal; contains inferior rectal nerve/vessels + pudendal canal (Alcock's); communicates posteriorly via deep postanal space → horseshoe abscess
- Anal fissure: posterior midline (poor blood supply); chronic = lateral internal sphincterotomy
- Fistula-in-ano: Goodsall's rule (anterior = straight; posterior = curved to posterior midline); Parks' classification
- Episiotomy: mediolateral preferred in India; protects anal sphincter from 3rd/4th degree extension