Page 1 of 4
AN50.1-4 | Vertebral column — SDL Guide
Learning Objectives
- Describe the curvatures of the vertebral column (AN50.1)
- Describe and demonstrate the type, articular ends, ligaments, and movements of intervertebral joints, sacroiliac joints, and pubic symphysis (AN50.2)
- Describe lumbar puncture — site, direction of needle, and structures pierced (AN50.3)
- Explain the anatomical basis of scoliosis, lordosis, prolapsed intervertebral disc, spondylolisthesis, and spina bifida (AN50.4)
INSTRUCTIONS
Read each section carefully. The vertebral column underpins the anatomy of disc prolapse, scoliosis, spondylolisthesis, spina bifida, and lumbar puncture — all common in Indian clinical practice. Build a clear understanding of the curvatures, joints, ligaments, and the intervertebral disc before moving to the applied sections.
References
- BD Chaurasia's Human Anatomy Vol. 3 — Vertebral Column chapter (Textbook)
- Gray's Anatomy for Students — Vertebral Column chapter (Textbook)
- OpenStax Anatomy and Physiology 2e — The Axial Skeleton (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 42-year-old construction worker from Chennai is brought to casualty after lifting a heavy load and experiencing a sudden "pop" in his lower back, followed by excruciating left leg pain radiating from the buttock down to the foot. He cannot straight-leg raise on the left beyond 30°. His left ankle jerk is absent.
Which disc has prolapsed? Which nerve root is being compressed — and why is the pain radiating down to the foot? What is the anatomical relationship between the disc level and the nerve root that is compressed? Why is L4–L5 disc prolapse common in labourers?
Disc prolapse is the most common spinal condition presenting to Indian hospitals. An orthopaedic surgeon, neurosurgeon, or GP in India will diagnose disc prolapse daily — and accurate anatomical reasoning determines whether to operate and on which level.
WHY THIS MATTERS
Vertebral column anatomy has direct clinical relevance in India:
- Disc prolapse (PIVD): enormous burden in India — manual labourers, IT professionals, and road workers; L4–L5 and L5–S1 account for 90% of symptomatic disc prolapses
- Scoliosis: common in adolescent girls presenting to orthopaedic OPDs; early detection prevents respiratory compromise
- TB spine (Pott's disease): most common cause of paraplegia in India; kyphotic deformity, cold abscess, vertebral body destruction
- Spondylolisthesis: common cause of chronic low back pain in young Indian adults; L4 sliding over L5 is the typical pattern
- Spina bifida: included in the national neural tube defect prevention programme (folic acid supplementation)
- Sacroiliac joint disease: ankylosing spondylitis (axial spondyloarthropathy) is common in young Indian males (HLA-B27 associated); morning stiffness + limited lumbar flexion
RECALL
Before we begin, recall:
- The vertebral column has 33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral (fused), 4–5 coccygeal (fused)
- A typical vertebra has: body (weight-bearing), vertebral arch (pedicles + laminae), spinous process, 2 transverse processes, 4 articular processes (2 superior, 2 inferior — zygapophyseal joints)
- Regional differences: cervical — bifid spine, transverse foramina; thoracic — costal facets, heart-shaped body; lumbar — massive body, no transverse foramina, no costal facets, thick rectangular spinous process
- The intervertebral disc occupies ~25% of vertebral column height; absent at C1–C2 and sacrum
Curvatures of the Vertebral Column (AN50.1)
Four curvatures in the sagittal plane:
| Curvature | Direction | Onset | Classification |
|---|---|---|---|
| Cervical lordosis | Convex anteriorly | When infant lifts head (4 months) | Secondary (compensatory) |
| Thoracic kyphosis | Convex posteriorly | Present at birth (primary) | Primary |
| Lumbar lordosis | Convex anteriorly | When infant begins to stand/walk (12–18 months) | Secondary (compensatory) |
| Sacral kyphosis | Convex posteriorly | Present at birth (primary) | Primary |
Primary curvatures (thoracic + sacral): present at birth; reflect the shape of the embryonic C-shaped flexure
Secondary (compensatory) curvatures (cervical + lumbar): develop postnatally with erect posture
Clinical curvature changes:
- Scoliosis: lateral curvature of the spine (see AN50.4)
- Kyphosis: exaggeration of the thoracic kyphosis; causes include Pott's disease (TB), osteoporotic vertebral fractures (common in Indian postmenopausal women), Scheuermann's disease (adolescent)
- Lordosis: exaggeration of lumbar lordosis; causes include pregnancy (transient), obesity, hip flexor contracture, bilateral congenital hip dislocation
- Flat back: loss of lumbar lordosis after spinal fusion or ankylosing spondylitis

Figure: Curvatures of the Vertebral Column (AN50.1)
Intervertebral Joints and Ligaments (AN50.2)
Two types of joints between adjacent vertebrae:

Figure: Intervertebral Joints and Ligaments (AN50.2)
1. Intervertebral (cartilaginous) joints — between vertebral bodies:
- Type: secondary cartilaginous (symphysis)
- Articular surfaces: hyaline cartilage plates on each vertebral body + fibrocartilaginous intervertebral disc between them
- Intervertebral disc structure:
- Nucleus pulposus (centre): gelatinous, high water content (90% in young adults, decreases with age); embryological remnant of the notochord; acts as a hydraulic shock absorber
- Annulus fibrosus (outer ring): concentric lamellae of obliquely oriented fibrocartilage; posterior part is thinner (predisposes to posterolateral disc herniation)
2. Zygapophyseal (facet) joints — between articular processes:
- Type: synovial plane joints
- Orientation varies by region → determines movement: cervical (oblique, allows rotation + flexion), thoracic (coronal, limits flexion), lumbar (sagittal, allows flexion/extension, limits rotation)
Key ligaments of the vertebral column:
| Ligament | Attachment | Function |
|---|---|---|
| Anterior longitudinal ligament (ALL) | Skull → sacrum on anterior vertebral bodies | Prevents hyperextension; reinforces anterior disc |
| Posterior longitudinal ligament (PLL) | Skull → sacrum in vertebral canal on posterior bodies | Prevents hyperflexion; CENTRAL protection of disc (narrow → posterolateral disc bulge can bypass PLL) |
| Ligamentum flavum | Lamina of one vertebra to lamina below | Elastic; maintains upright posture; thick at lumbar level (can cause canal stenosis when hypertrophied) |
| Interspinous ligament | Between adjacent spinous processes | Limits flexion |
| Supraspinous ligament | Tips of spinous processes C7 to sacrum | Limits flexion (becomes ligamentum nuchae in the neck) |
| Intertransverse ligaments | Between transverse processes | Limits lateral flexion |
Sacroiliac joint:
- Type: synovial (upper part) + syndesmosis (lower part); some cartilaginous elements
- Extremely strong anterior and posterior sacroiliac ligaments (strongest ligaments in the body)
- Movement: very limited (slight nutation/counternutation during pregnancy)
- Ankylosing spondylitis affects the sacroiliac joints first → bilateral sacroiliitis → progressive fusion ("bamboo spine")
Pubic symphysis:
- Type: secondary cartilaginous (with fibrocartilaginous disc)
- Held by superior pubic ligament and inferior arcuate ligament
- Slight movement during pregnancy (relaxin → ligament relaxation)
- Osteitis pubis: inflammation of the symphysis → groin pain in footballers and multiparous women
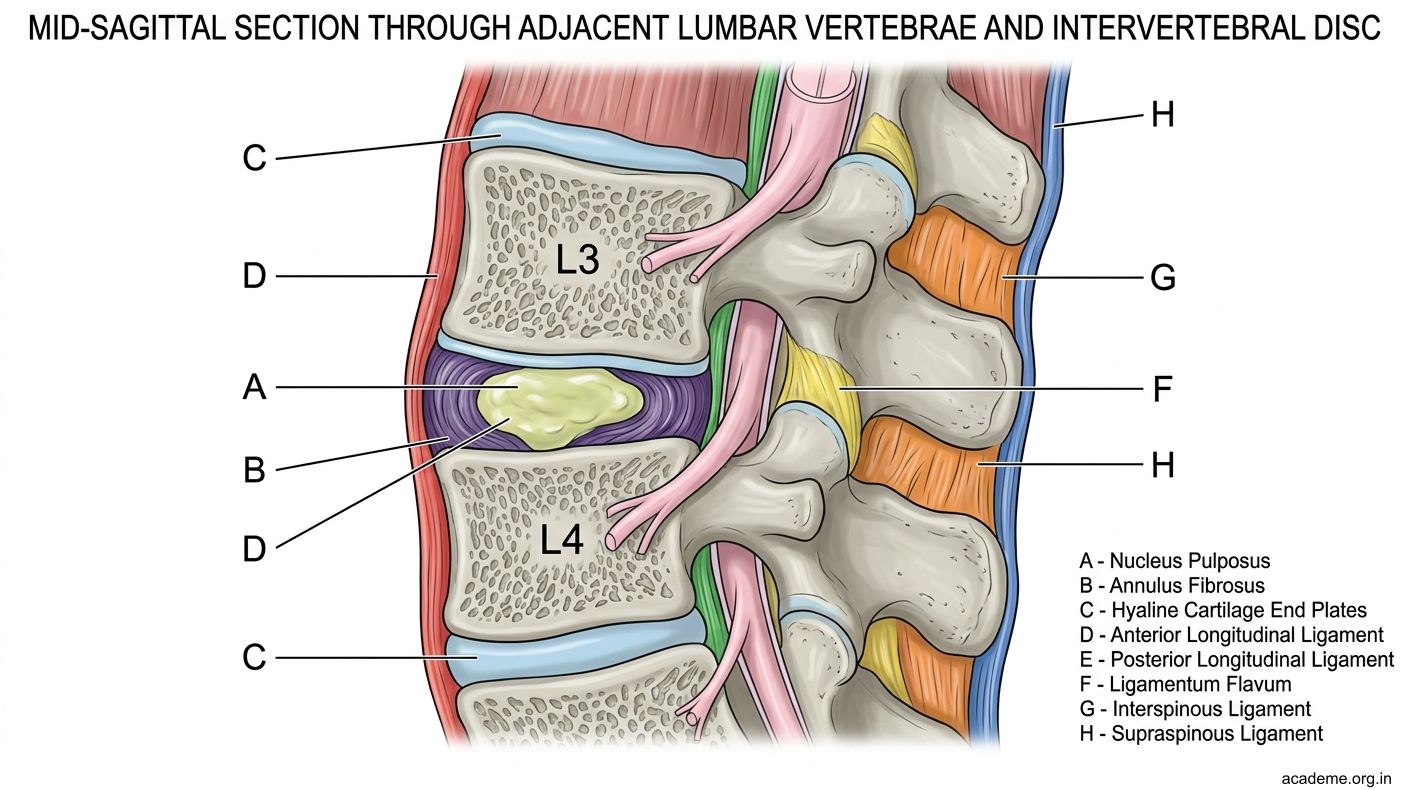
Figure: Intervertebral Joints and Ligaments (AN50.2)

Figure: Key ligaments of the vertebral column:
The Intervertebral Disc — Prolapse Anatomy (AN50.4 excerpt)
Disc prolapse (Prolapsed Intervertebral Disc / PIVD):

Figure: The Intervertebral Disc — Prolapse Anatomy (AN50.4 excerpt)
- Mechanism: The annulus fibrosus tears (usually posterolateral) → nucleus pulposus herniates through the tear → compresses adjacent nerve root
- Why posterolateral? The PLL is broad centrally but tapers laterally → posterolateral annulus is the weakest point; this is where 95% of herniations occur
- Common levels: L4–L5 (most common; compresses L5 root) and L5–S1 (compresses S1 root); together account for ~90%
Nerve root numbering rule:
- At lumbar levels, each nerve root exits BELOW the pedicle of the SAME-numbered vertebra
- The disc between L4 and L5 sits ABOVE the L4–L5 exit foramen; a posterolateral L4–L5 disc herniation compresses the L5 nerve root (which is descending to its exit foramen one level below)
- L4–L5 disc herniation → L5 nerve root compression:
- Pain: down the lateral leg to the dorsum of the foot + big toe (L5 dermatome)
- Weakness: foot dorsiflexion (tibialis anterior, L4–L5)
- Reflexes: usually preserved (ankle jerk = S1)
- Straight leg raise positive (sciatic stretch sign)
- L5–S1 disc herniation → S1 nerve root compression:
- Pain: down posterior thigh, posterior leg, lateral foot, little toe (S1 dermatome)
- Weakness: plantar flexion (gastrocnemius-soleus, S1)
- Reflex: absent ankle jerk (S1)
Cauda equina syndrome (central massive disc prolapse at L4–L5 or L5–S1):
- Bilateral leg weakness/numbness
- Saddle anaesthesia (perineum, inner thighs)
- Urinary retention or incontinence
- Reduced anal sphincter tone
- Surgical emergency — decompress within hours
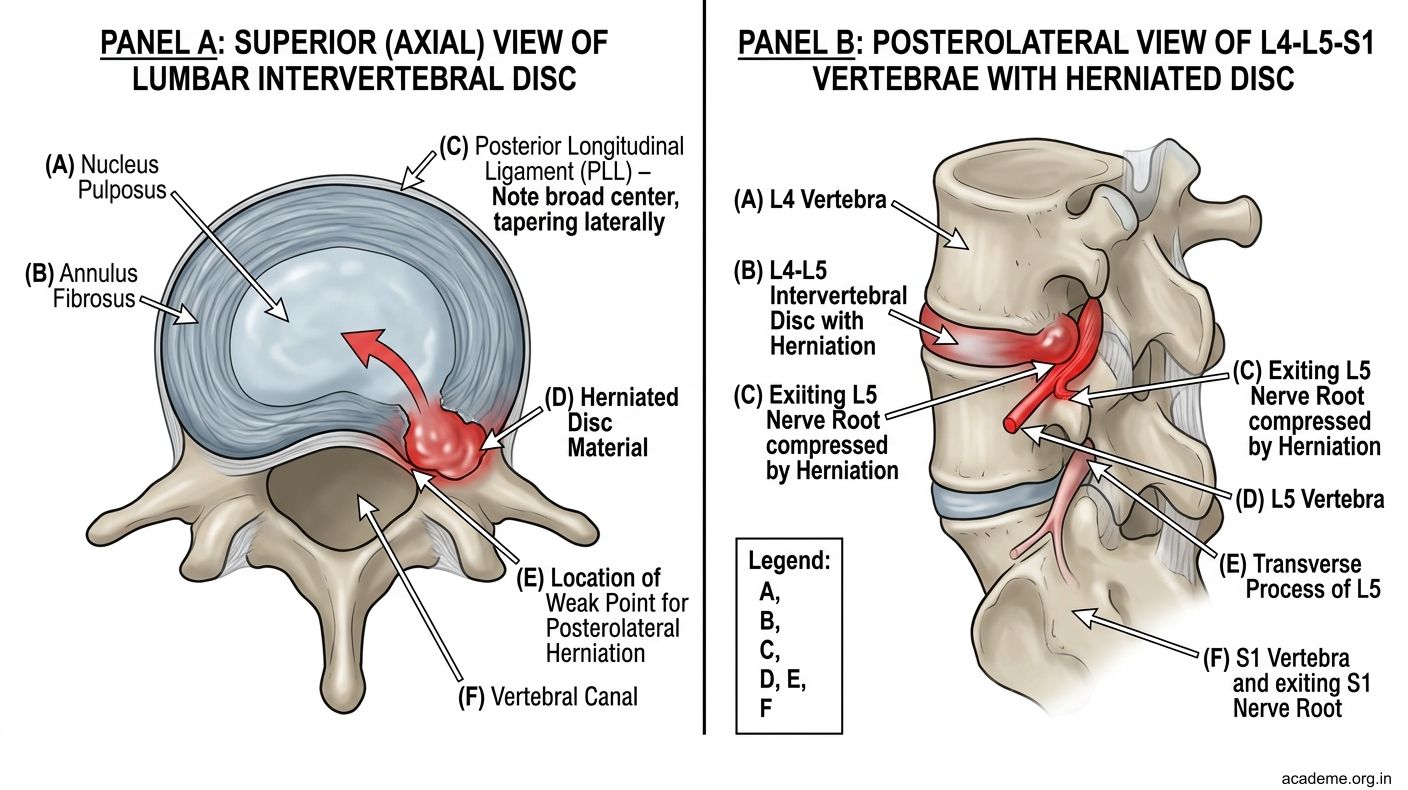
Figure: The Intervertebral Disc — Prolapse Anatomy (AN50.4 excerpt)
Scoliosis, Lordosis, Spondylolisthesis, Spina Bifida (AN50.4)
Scoliosis:
- Lateral curvature of the spine in the coronal plane (often with rotational component)
- Idiopathic scoliosis (80%): most common in adolescent girls; right thoracic curve typical; Cobb angle >10° = scoliosis; >45–50° = surgery
- Secondary scoliosis: leg length discrepancy, hemivertebra, poliomyelitis, NF1, cerebral palsy
- Anatomical consequence: rib hump (rotation of vertebral bodies → ribs rotate posteriorly on convex side → rib prominence on forward bending — Adam's forward bending test)
- Screening: school-based scoliometer screening in India for adolescents
Lordosis:
- Exaggerated lumbar (or cervical) lordosis — convex anteriorly
- Common in pregnancy (shifting centre of gravity), obesity, bilateral hip dislocation
- Flat lumbar lordosis seen in ankylosing spondylitis, muscle spasm from disc prolapse
Spondylolisthesis:
- Forward (anterior) slip of one vertebra on the vertebra below
- Types:
| Type | Mechanism |
|---|---|
| Isthmic (most common) | Stress fracture of the pars interarticularis (= spondylolysis) → vertebra slips forward; usually L4–L5 or L5–S1; gymnasts, fast bowlers |
| Degenerative | Facet joint and disc degeneration in older adults → L4–L5 most common |
| Dysplastic | Congenital defect in the posterior arch |
Spina bifida:
- Failure of fusion of the vertebral arch (posterior neuropore closure failure) — a neural tube defect
- Spina bifida occulta: laminae fail to fuse but meninges and cord intact; often asymptomatic; may have overlying hair tuft/dimple/haemangioma
- Spina bifida cystica:
- Meningocoele: only meninges herniate through the defect; cord intact; good prognosis
- Meningomyelocoele (most common cystic form): cord + nerve roots herniate with meninges → severe neurological deficit below the level of lesion (paralysis, incontinence); associated with Arnold-Chiari malformation + hydrocephalus
- Prevention: folic acid 400 mcg/day (5 mg if previous affected child) periconceptionally → reduces NTD incidence by 70%; key public health message in India

Figure: Scoliosis, Lordosis, Spondylolisthesis, Spina Bifida (AN50.4)

Figure: Vertebral Column — Key Points:
SELF-CHECK
A. L3–L4 (compressing the L4 nerve root)
B. L4–L5 (compressing the L5 nerve root)
C. L5–S1 (compressing the S1 nerve root)
D. L2–L3 (compressing the L3 nerve root)
Reveal Answer
Answer: see explanation below
Absent ankle jerk = S1 nerve root deficit. S1 also supplies the gastrocnemius and soleus (plantar flexion). S1 exits at the L5–S1 foramen. An L5–S1 posterolateral disc prolapse compresses the descending S1 nerve root. L4–L5 disc herniation compresses L5 (foot drop, first dorsal web space sensory loss, ankle jerk preserved). Absent ankle jerk = S1 = L5–S1 disc.
CLINICAL PEARL
Spina bifida and the back dimple: In neonates, a pit or dimple at the lumbosacral junction is a common finding. A small, well-defined midline dimple that is above the intergluteal cleft and close to the base of the sacrum (below L5) is usually benign (benign sacral dimple). However, a dimple above L5, or one with associated tuft of hair, haemangioma, skin tag, or discolouration should be investigated with spinal ultrasound (and MRI if ultrasound shows abnormality) to exclude occult spinal dysraphism (spina bifida occulta, tethered cord, lipomyelomeningocoele). This distinction is tested in MBBS examinations and paediatric ward rounds across India.
REFLECT
A 16-year-old girl from Karaikal is brought by her parents because her school nurse noticed that her right shoulder is higher than her left and her back is asymmetric on bending forward. X-ray shows a 35-degree right thoracic curve.
What is the diagnosis? How do you measure the Cobb angle? What is the significance of the rotational component — and why does it cause the rib hump? At what Cobb angle would you refer her for a surgical opinion? What is the natural history if untreated?
KEY TAKEAWAYS
Vertebral Column — Key Points:
- Curvatures: primary = thoracic + sacral kyphosis (foetal); secondary = cervical + lumbar lordosis (postnatal, erect posture)
- Intervertebral disc: nucleus pulposus (notochord remnant, gelatinous) + annulus fibrosus (fibrocartilage rings); posterior annulus weakest → posterolateral herniation
- Disc prolapse levels: L4–L5 compresses L5 root (foot drop, dorsum foot numbness); L5–S1 compresses S1 root (absent ankle jerk, plantar flexion weakness)
- Ligaments: ALL (prevents hyperextension); PLL (narrow laterally → posterolateral disc herniates past it); ligamentum flavum (elastic, can stenose canal); supraspinous + interspinous (limit flexion)
- Lumbar puncture: L3–L4 or L4–L5; Tuffier's line = L4; structures pierced: supraspinous → interspinous → ligamentum flavum → epidural space → dura → arachnoid → subarachnoid space (CSF)
- Scoliosis: lateral + rotational; adolescent girls; Cobb angle; Adam's forward bend test; surgery if >45°
- Spondylolisthesis: forward slip; isthmic (pars fracture) most common; L5–S1; fast bowlers/gymnasts
- Spina bifida: arch fusion failure; occulta (benign), meningocoele (meninges only), meningomyelocoele (cord + roots; severe deficit); prevent with folic acid
- Sacroiliac joint: synovial + syndesmosis; ankylosing spondylitis → bilateral sacroiliitis → bamboo spine