Page 1 of 4
AN53.1-4 | Osteology — SDL Guide
Learning Objectives
- Identify a bone in anatomical position and describe its salient features, articulations, and muscle attachments (AN53.1)
- Demonstrate the anatomical position of the bony pelvis and identify boundaries of pelvic inlet, cavity, and outlet (AN53.2)
- Define and demonstrate true vs false pelvis and sex determination from the bony pelvis (AN53.3)
- Explain clinical importance of sacralisation, lumbarisation, pelvic types, and coccyx variations (AN53.4)
INSTRUCTIONS
Study this module alongside an actual bone specimen or a detailed bone atlas. The practical component requires you to hold a bone in anatomical position and demonstrate attachments. For the pelvis, use the bisected model in the anatomy museum.
References
- BD Chaurasia's Human Anatomy, Vol. 2 — Abdomen and Pelvis (Textbook)
- Gray's Anatomy for Students — Pelvis and Perineum (Textbook)
- Cunningham's Manual of Practical Anatomy, Vol. 2 (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 28-year-old primigravida from Puducherry is admitted at 38 weeks of gestation with failure to progress in the first stage of labour. A clinical pelvic assessment is performed by the obstetrician. The findings are: diagonal conjugate = 10.5 cm, subpubic angle = 70°, ischial spines prominent, sacrum straight (not curved).
The obstetrician diagnoses "android (male-type) pelvis" and proceeds to emergency caesarean section.
What are the four types of bony pelvis? How does sex determination from the bony pelvis work? Why does an android pelvis cause obstructed labour?
This module systematically covers the osteology of the abdominopelvic bones — from bone identification in anatomical position to the obstetric relevance of pelvic shape.
WHY THIS MATTERS
The osteology of the abdominopelvic region is clinically relevant in India because:
- Obstetric emergencies — cephalopelvic disproportion (CPD) due to pelvic shape variations is a major cause of obstructed labour and emergency caesarean section in India
- Forensic medicine — sex determination from skeletal remains relies primarily on pelvic bones; age estimation from epiphyseal fusion is legally required in medicolegal cases
- Radiological diagnosis — sacralization and lumbarisation are common incidental findings on lumbar spine X-rays in Indian patients presenting with low back pain
- Pelvic fractures — road traffic accidents in India cause pelvic ring fractures; understanding the anatomy guides emergency management
- Anatomy practicals — NMC mandates demonstration of bones in anatomical position and identification of muscle attachments (AN53.1)
RECALL
Before we begin, recall:
- The hip bone (os coxae) is formed by three bones that fuse at the acetabulum: ilium (superior), ischium (posteroinferior), pubis (anteroinferior). They fuse at the acetabulum by age 15–16 years.
- The bony pelvis consists of: 2 hip bones + sacrum + coccyx, joined by symphysis pubis (anteriorly) and two sacroiliac joints (posteriorly)
- The pelvic brim separates the greater (false) pelvis above from the lesser (true) pelvis below
- Anatomical position of a bone: the position the bone occupies in a living human standing erect with arms at sides and palms forward
Part 1: Bone Identification in Anatomical Position (AN53.1)
Holding a Bone in Anatomical Position — General Principles

Figure: Part 1: Bone Identification in Anatomical Position (AN53.1)
For any bone, orient it by identifying:
1. Landmarks — specific named prominences, depressions, or processes unique to that bone
2. Articular surfaces — smooth, cartilage-covered surfaces; face toward the bone they articulate with
3. Nutrient foramen — the oblique hole for the nutrient artery; its opening faces AWAY from the growing end
4. Side identification — convex vs concave surfaces, specific landmarks
Lumbar Vertebra (e.g., L3) — Practical Identification:
| Feature | Detail |
|---|---|
| Vertebral body | Large, kidney-shaped, widest transversely |
| Pedicle | Short, stout |
| Lamina | Broad |
| Spinous process | Short, horizontal (hatchet-shaped), points directly backward |
| Transverse processes | Slender, no costal facets |
| Articular facets | Vertical orientation; superior articular facets face medially (sagittal plane) → locks lumbar vertebrae, allows flexion/extension, prevents rotation |
| Mammillary process | Small tubercle on superior articular process |
Sacrum in Anatomical Position:
The sacrum is held with its concave pelvic surface facing anteriorly and inferiorly; the apex (tip) points inferiorly.
| Feature | Side |
|---|---|
| Pelvic (anterior) surface | Concave, smooth, 4 anterior sacral foramina (S1–S4) |
| Dorsal (posterior) surface | Convex, rough, 4 posterior sacral foramina |
| Lateral surface | Ear-shaped (auricular) surface for sacroiliac joint |
| Base (S1) | Superior; the sacral promontory projects anteriorly from the upper margin of S1 body |
| Apex (S5) | Inferior; articulates with coccyx |
Coccyx in Anatomical Position:
Held with the concave pelvic surface facing anteriorly; apex points downward. Usually 4 coccygeal vertebrae (can be 3 or 5). The base articulates with the sacral apex.
Muscle Attachments on the Sacrum and Coccyx:
• Gluteus maximus — posterior surface of sacrum and coccyx
• Piriformis — anterior surface of sacrum (S2–S4), exits greater sciatic foramen
• Coccygeus — tip and lateral border of coccyx → ischial spine
• Levator ani — inner surface of ilium (anterior) and coccyx
• Iliacus — iliac fossa on the medial surface of ilium
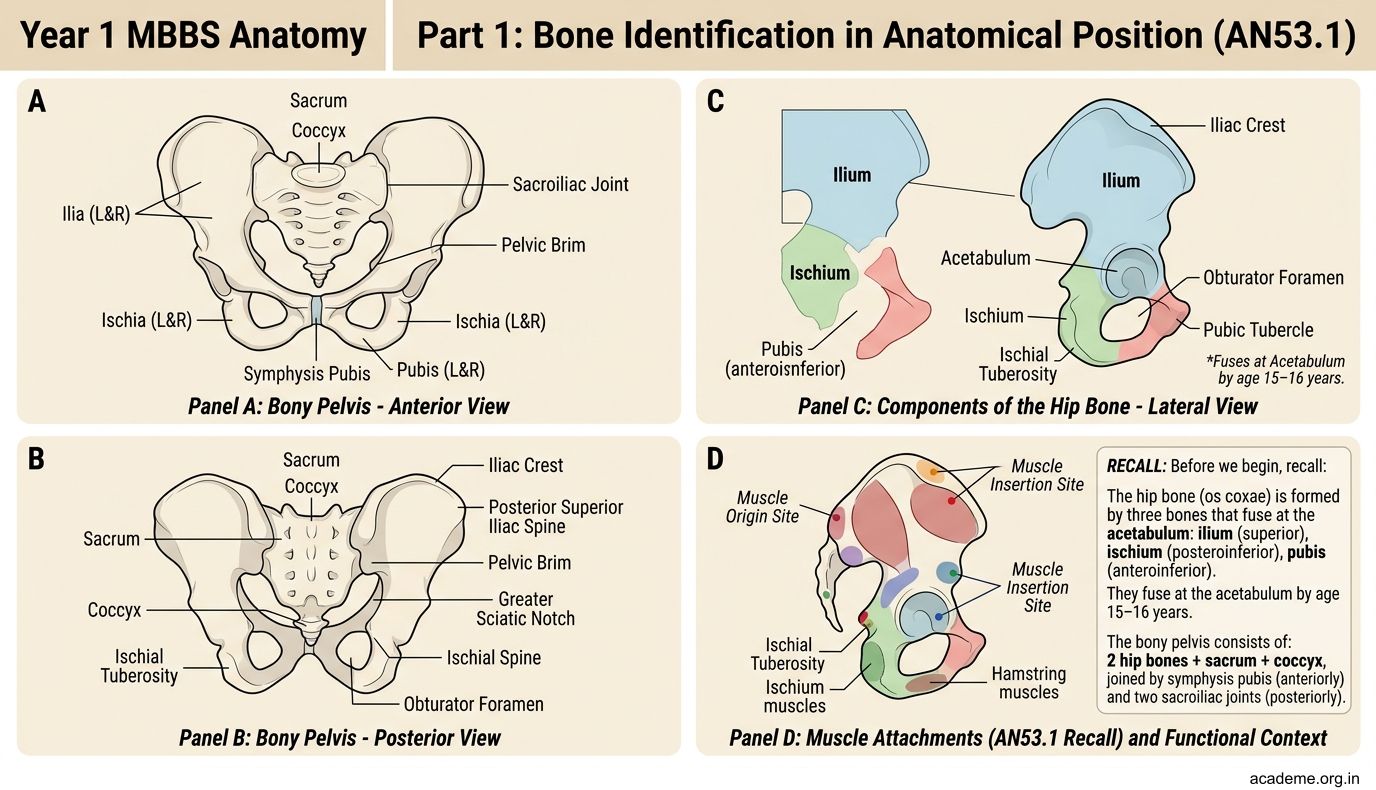
Figure: Part 1: Bone Identification in Anatomical Position (AN53.1)

Figure: Lumbar Vertebra (e.g., L3) — Practical Identification:
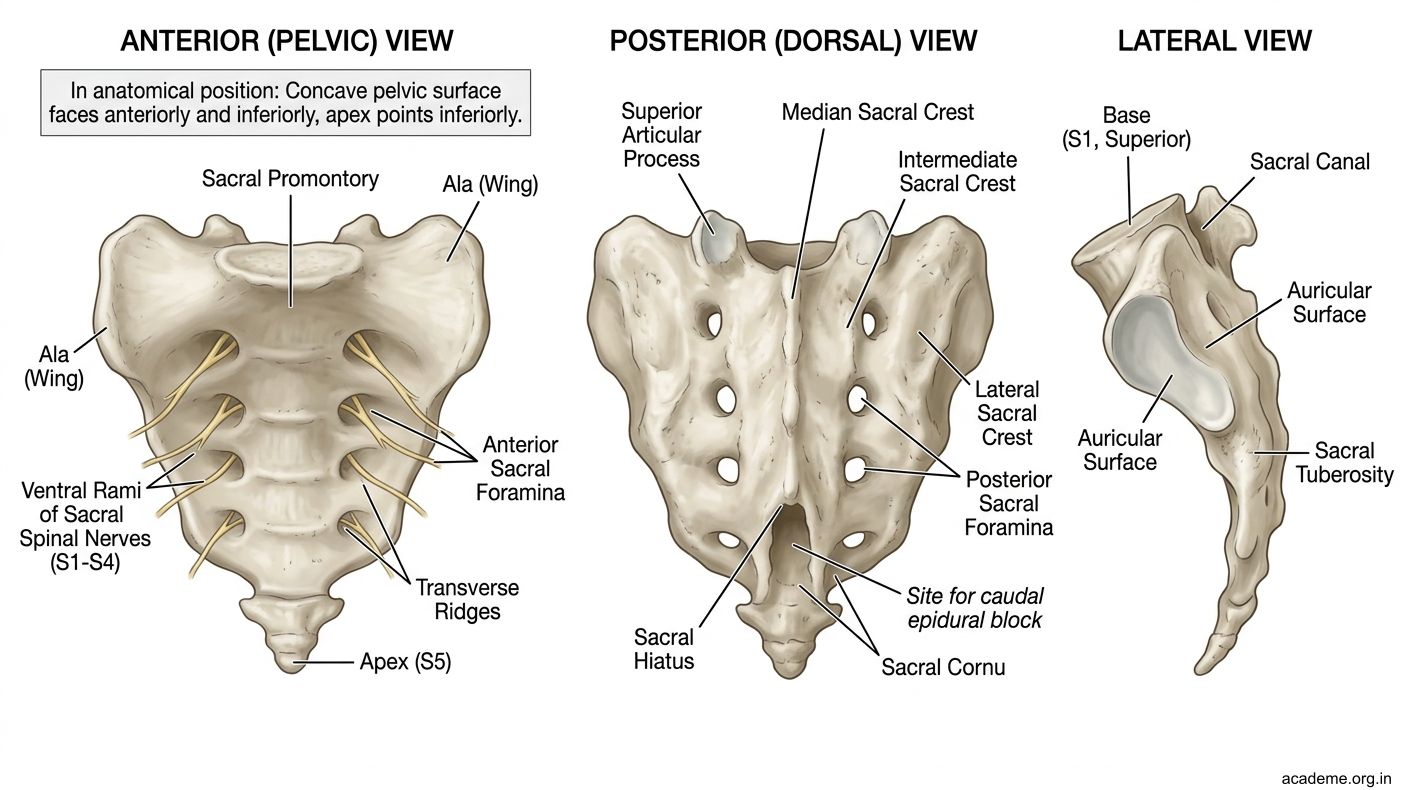
Figure: Lumbar Vertebra (e.g., L3) — Practical Identification:
Part 2: Bony Pelvis — Anatomical Position, Inlet, Cavity, Outlet (AN53.2)
Bony Pelvis in Anatomical Position

Figure: Pelvic Inlet (Brim)

Figure: Part 2: Bony Pelvis — Anatomical Position, Inlet, Cavity, Outlet (AN53.2)
In anatomical position (standing erect), the pelvis is tilted so that:
• The anterior superior iliac spine (ASIS) and the upper edge of the pubic symphysis lie in the SAME vertical plane (coronal plane)
• The pelvic brim faces anterosuperiorly, making approximately 60° with the horizontal
• The coccyx tip is at the level of the upper border of the pubic symphysis
Pelvic Inlet (Brim)
The pelvic inlet is bounded by (tracing anteriorly → posteriorly):
• Anteriorly: Upper border of pubic symphysis and pubic crest
• Laterally: Pectineal line (pecten pubis) → arcuate line of ilium
• Posteriorly: Sacral promontory (anterior upper border of S1)
Pelvic inlet diameters:
| Diameter | Measurement | Obstetric significance |
|---|---|---|
| Anteroposterior (true conjugate) | 11 cm (promontory → inner surface of pubic symphysis) | Cannot be measured clinically |
| Diagonal conjugate | 12.5 cm (promontory → lower border of pubic symphysis) | Clinically measured per vaginum |
| Obstetric conjugate | 10.5 cm (promontory → internal pubic symphysis projection) | The smallest AP diameter; estimated: diagonal conjugate − 1.5 cm |
| Transverse | 13 cm (widest across pelvic brim) | Widest diameter of inlet |
Pelvic Cavity
The space between the inlet above and the outlet below; bounded by:
• Anteriorly: Body of pubis
• Posteriorly: Hollow of sacrum and coccyx
• Laterally: Body of ischium, obturator internus fascia
Pelvic Outlet
Bounded by:
• Anteriorly: Lower border of pubic symphysis and pubic arch
• Laterally: Ischial tuberosities + sacrotuberous ligaments
• Posteriorly: Tip of coccyx
Pelvic outlet diameters:
| Diameter | Measurement |
|---|---|
| AP (subpubic to coccyx tip) | 13 cm (coccyx can move back in labour to 15 cm) |
| Transverse (inter-ischial) | 11 cm |
| Anterior sagittal | 6 cm |
| Posterior sagittal | 9 cm |
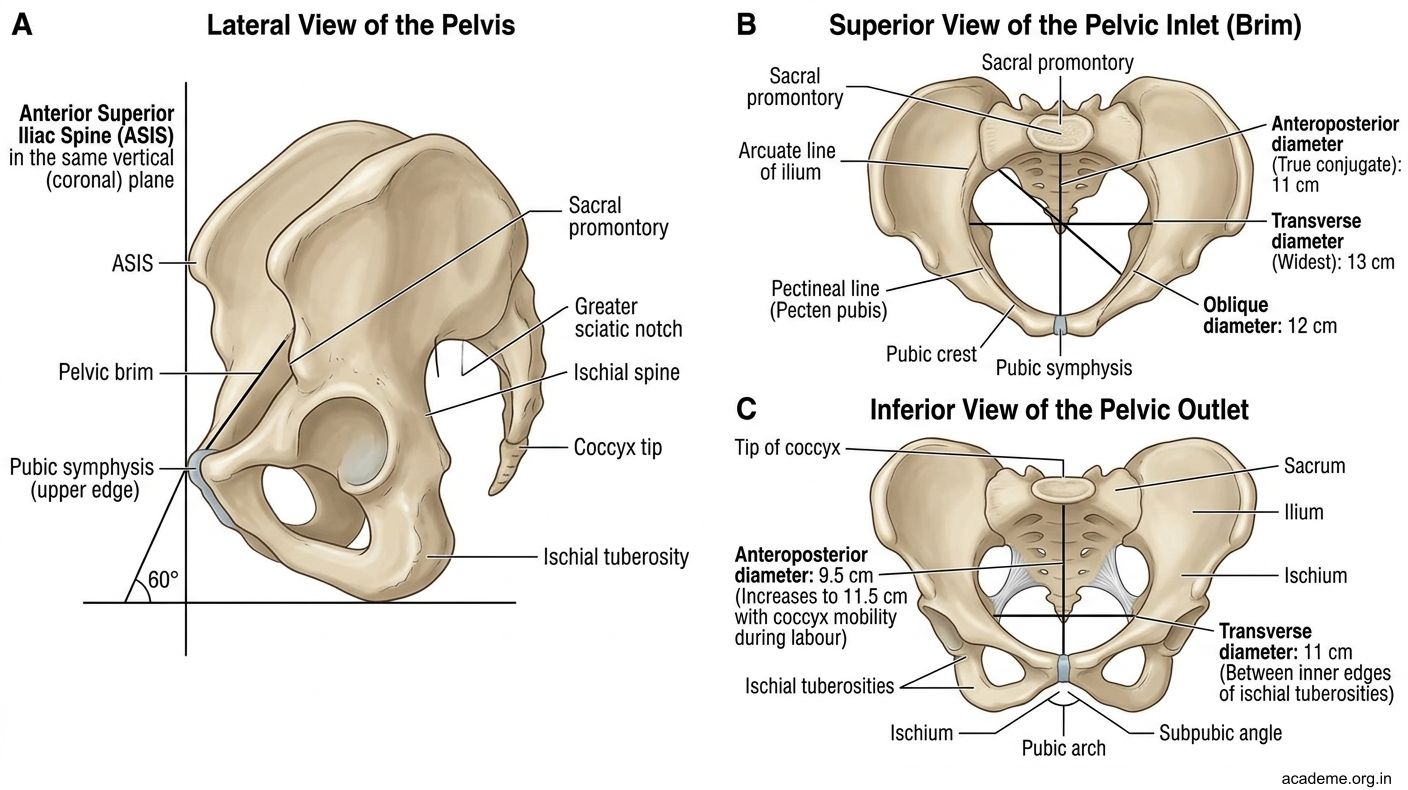
Figure: Part 2: Bony Pelvis — Anatomical Position, Inlet, Cavity, Outlet (AN53.2)
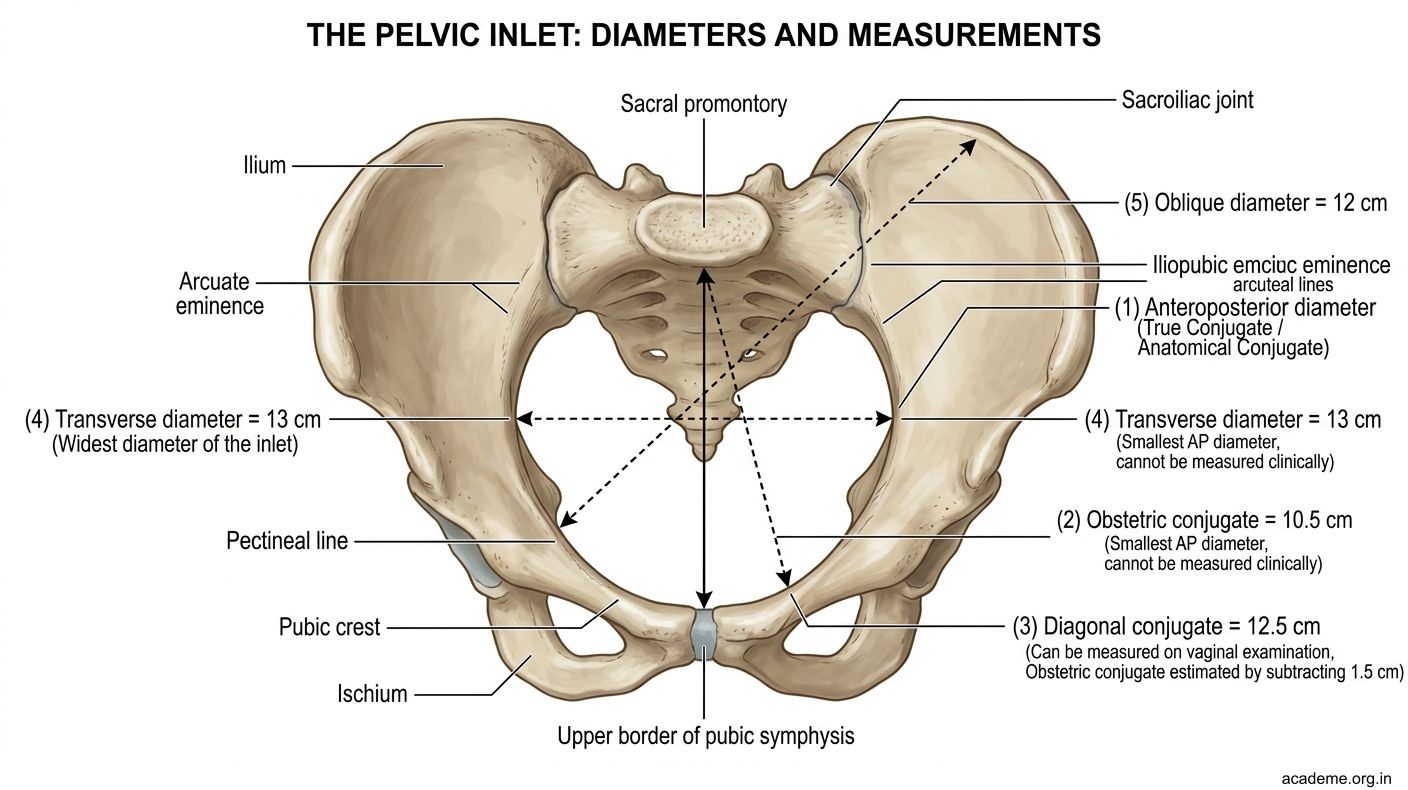
Figure: Pelvic Inlet (Brim)

Figure: Pelvic inlet diameters:
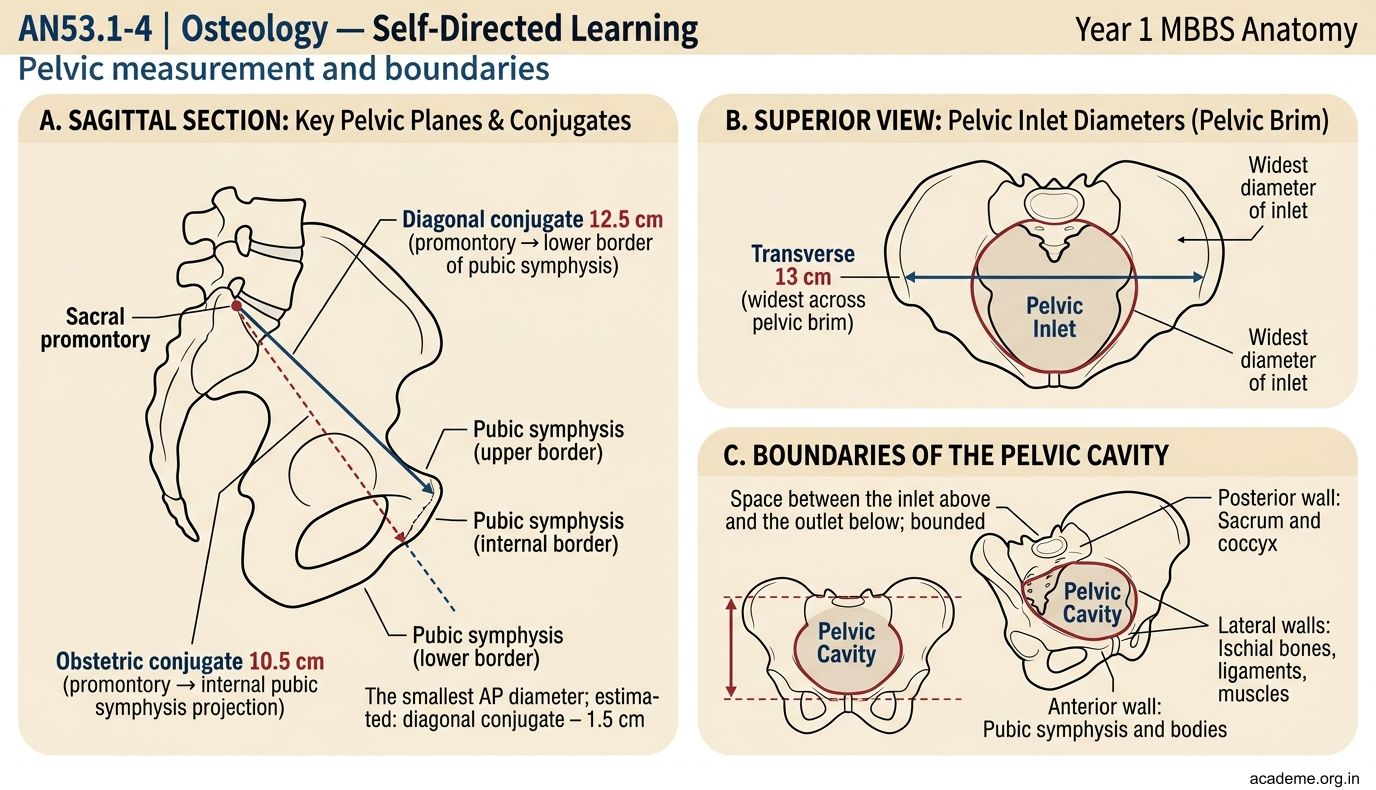
Figure: Pelvic inlet diameters:
Part 3: True vs False Pelvis and Sex Determination (AN53.3)
True (Lesser) Pelvis vs False (Greater) Pelvis

Figure: Sex Determination from the Bony Pelvis
| Feature | False (Greater) Pelvis | True (Lesser) Pelvis |
|---|---|---|
| Location | Above the pelvic brim | Below the pelvic brim |
| Boundaries | Iliac fossae + posterior abdominal wall above | Sacrum + ilium + ischium + pubis below |
| Contents | Iliac vessels, pelvic colon, small bowel, appendix (right) | Bladder, rectum, uterus/prostate, ovaries, vagina |
| Clinical | Referred pain from abdominal organs | Obstetric canal, pelvic surgery |
Sex Determination from the Bony Pelvis
The pelvis is the most reliable bone for sex determination (90% accuracy):
| Feature | Female Pelvis | Male Pelvis |
|---|---|---|
| Subpubic angle | >90° (obtuse) | <90° (acute) |
| Pelvic inlet shape | Oval/round | Heart-shaped (narrower A-P) |
| Sciatic notch | Wide (>90°) | Narrow (<60°) |
| Acetabulum | Small, faces anterolaterally | Large, faces more laterally |
| Obturator foramen | Triangular | Oval |
| Sacrum | Wide, short, more concave | Narrow, long, less concave |
| Ischial spines | Not prominent | Prominent (may project into pelvic cavity) |
| Overall shape | Gynaecoid — wide, shallow, circular inlet | Android — narrow, deep, heart-shaped inlet |
Practical mnemonic for sex determination: "Female pelvis is WIDE for BIRTH" — wider angle, wider notch, wider inlet, wider sciatic notch

Figure: Pelvic outlet diameters:

Figure: Part 3: True vs False Pelvis and Sex Determination (AN53.3)
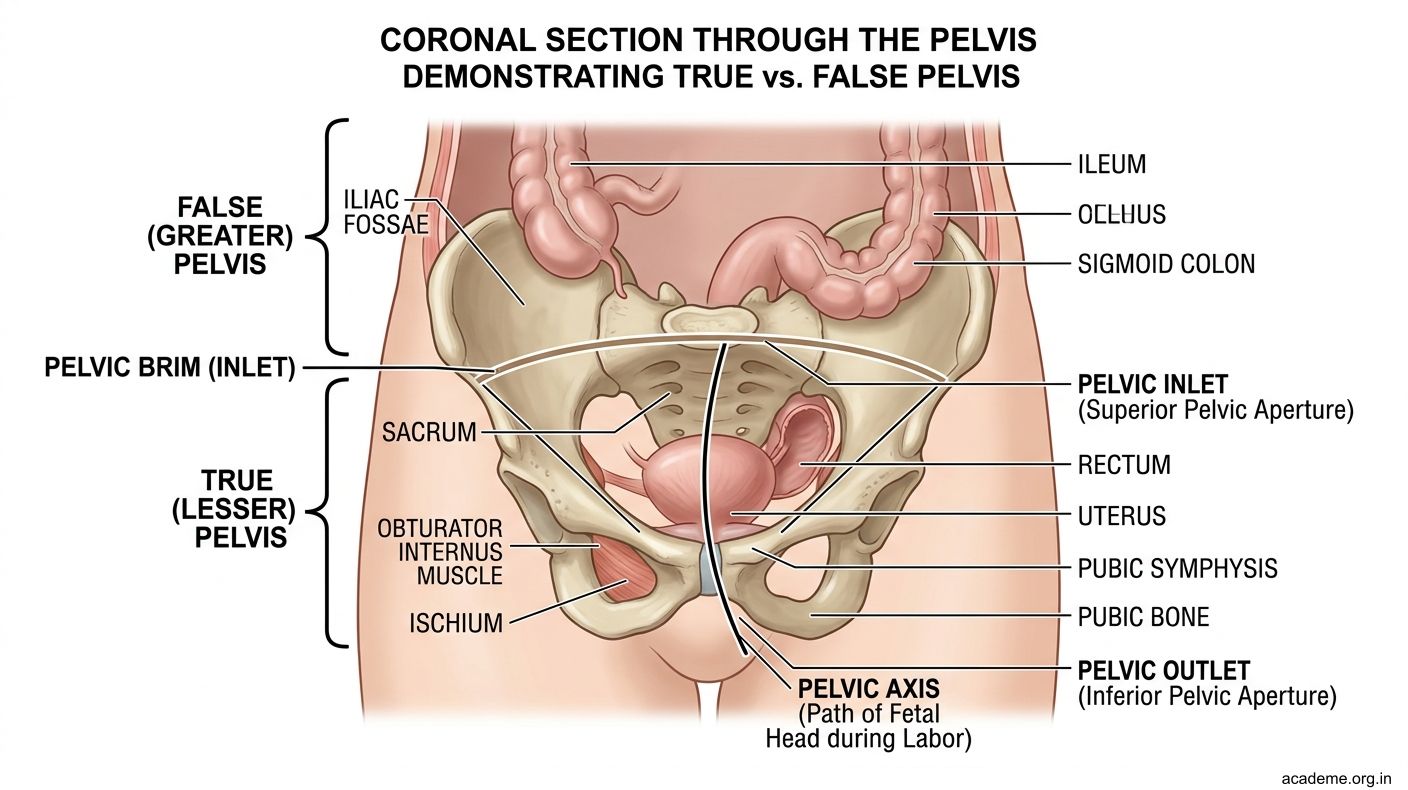
Figure: Pelvic outlet diameters:
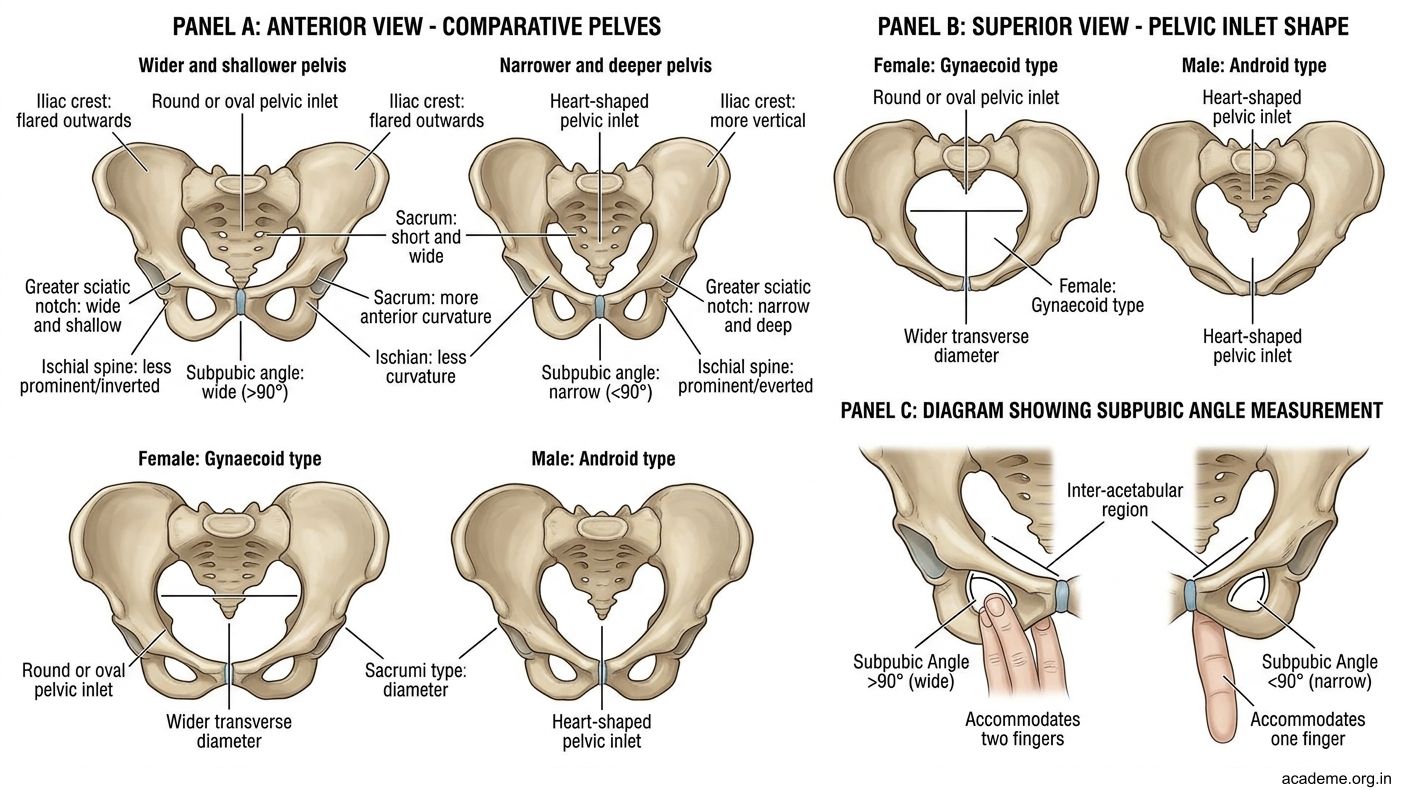
Figure: Part 3: True vs False Pelvis and Sex Determination (AN53.3)
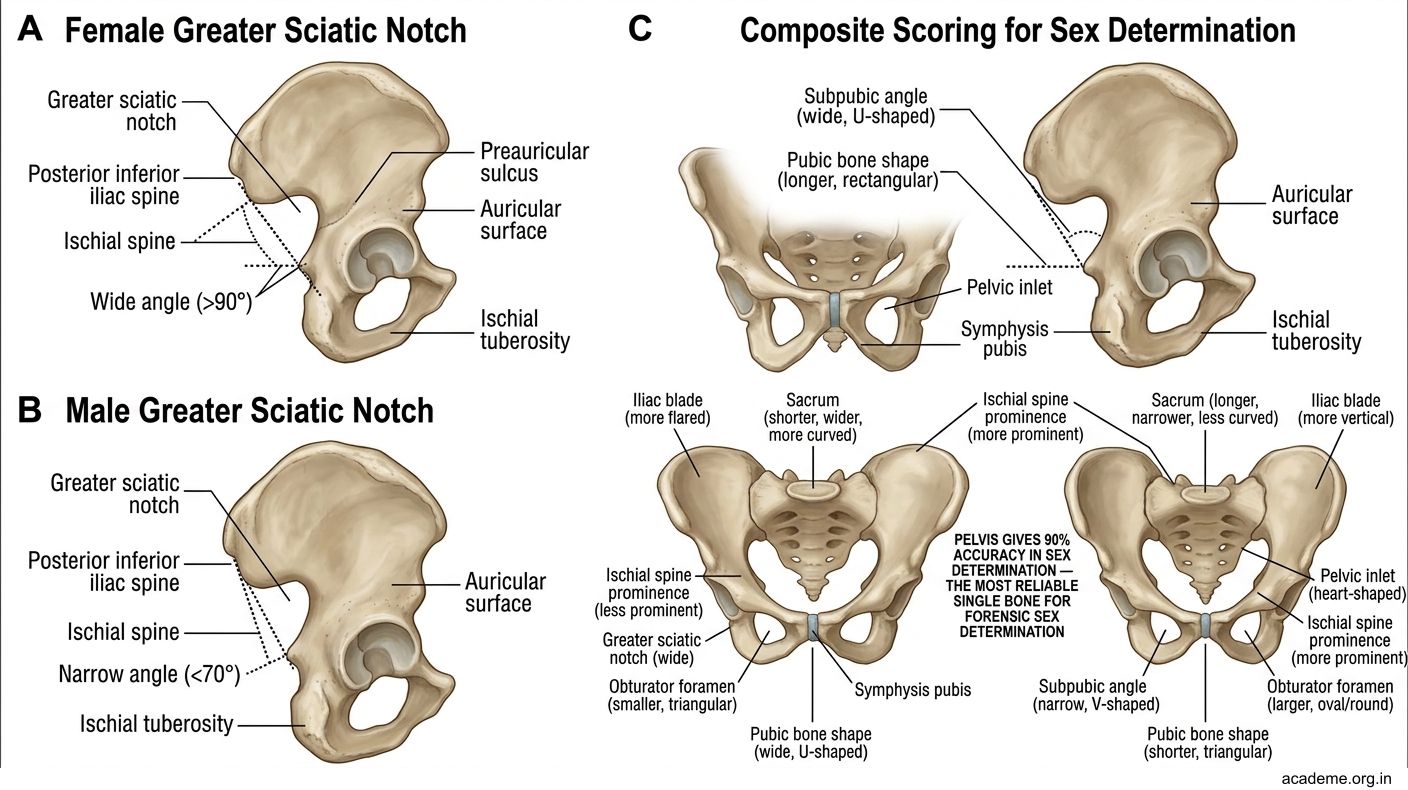
Figure: Sex Determination from the Bony Pelvis
SELF-CHECK — : Pelvis Anatomy
The obstetric conjugate is the smallest antero-posterior diameter of the pelvic inlet. It is measured from the sacral promontory to:
A. The lower border of the pubic symphysis
B. The upper border of the pubic symphysis
C. The most projecting inner surface of the pubic symphysis (posterior surface)
D. The midpoint of the pubic symphysis
Reveal Answer
Answer: C. The most projecting inner surface of the pubic symphysis (posterior surface)
A forensic pathologist examining pelvic bones notes: subpubic angle 75°, narrow greater sciatic notch, prominent ischial spines, and heart-shaped pelvic inlet. This skeleton most likely belongs to:
A. A female, gynaecoid pelvis
B. A male
C. A female, android pelvis
D. A female, platypelloid pelvis
Reveal Answer
Answer: B. A male
Part 4: Clinical Importance — Sacralisation, Lumbarisation, Pelvic Types, Coccyx (AN53.4)
Four Types of Bony Pelvis (Caldwell-Moloy Classification)

Figure: Obstructed Labour — How the Android Pelvis Causes Problems
| Type | Inlet Shape | Frequency in Indian Women | Obstetric Prognosis |
|---|---|---|---|
| Gynaecoid | Round/oval | ~50% | Excellent — widest in all dimensions |
| Android | Heart-shaped (narrow anterior) | ~25% | Poor — arrested labour, OP position |
| Anthropoid | Long oval (narrow transverse) | ~20% | Fair — deep transverse arrest possible |
| Platypelloid | Flat oval (narrow AP) | ~5% | Poor — flat inlet, transverse arrest |
Sacralization of the Lumbar Vertebra
Sacralization = the lowest lumbar vertebra (L5) fuses partially or completely with the sacrum, making it appear as part of the sacrum.
• Incidence: ~10% of the Indian population
• On X-ray: L5 appears fused; only 4 mobile lumbar vertebrae visible above
• Clinical: May cause low back pain due to altered biomechanics; can cause confusion during counting vertebral levels for epidural anaesthesia
• Types: Unilateral (more symptomatic) or bilateral (often asymptomatic)
Lumbarisation of the 1st Sacral Vertebra
Lumbarisation = the first sacral segment separates from the sacrum and functions as an additional lumbar vertebra, giving 6 mobile lumbar vertebrae.
• Less common than sacralization (~5%)
• On X-ray: 6 mobile lumbar vertebrae; sacrum has only 4 segments
• Clinical: Can cause low back pain and confuses vertebral level counting
Clinical importance of the Coccyx
• Coccydynia — pain at the tip of the coccyx; common after a fall onto the buttocks or after childbirth; treated conservatively (donut cushion) or rarely coccygectomy
• Coccyx in childbirth — the sacrococcygeal joint allows the coccyx to pivot backward by up to 2 cm during childbirth, increasing the AP diameter of the outlet
• Anomalies: Calcification of sacrococcygeal joint in older patients; bifid coccyx
Forensic Age Estimation from Pelvic Bones
• The iliac crest secondary ossification centre appears at puberty (13–14 years) and fuses by 16–17 years → complete fusion = adult
• Sacroiliac joint: In young adults, articular surface is smooth; with aging, the joint becomes irregular, develops osteophytes, and partial fusion in old age
• Pubic symphysis: At 18–20 years, ridged and irregular surface; by 35–40, surface smoothed; by 50+, erosive and pitted → forensic age estimation from pubic symphysis morphology

Figure: Part 4: Clinical Importance — Sacralisation, Lumbarisation, Pelvic Types, Coccyx (AN53.4)
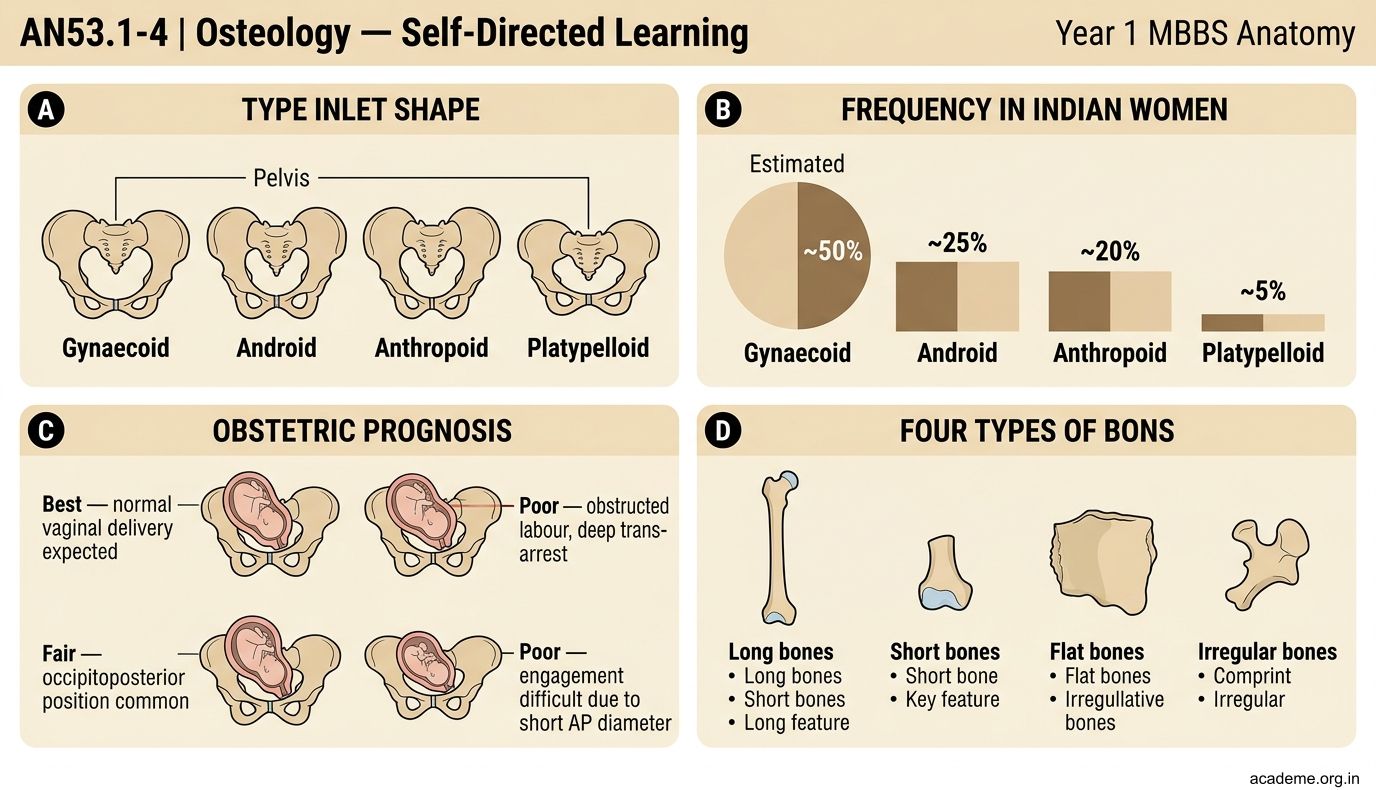
Figure: Part 4: Clinical Importance — Sacralisation, Lumbarisation, Pelvic Types, Coccyx (AN53.4)
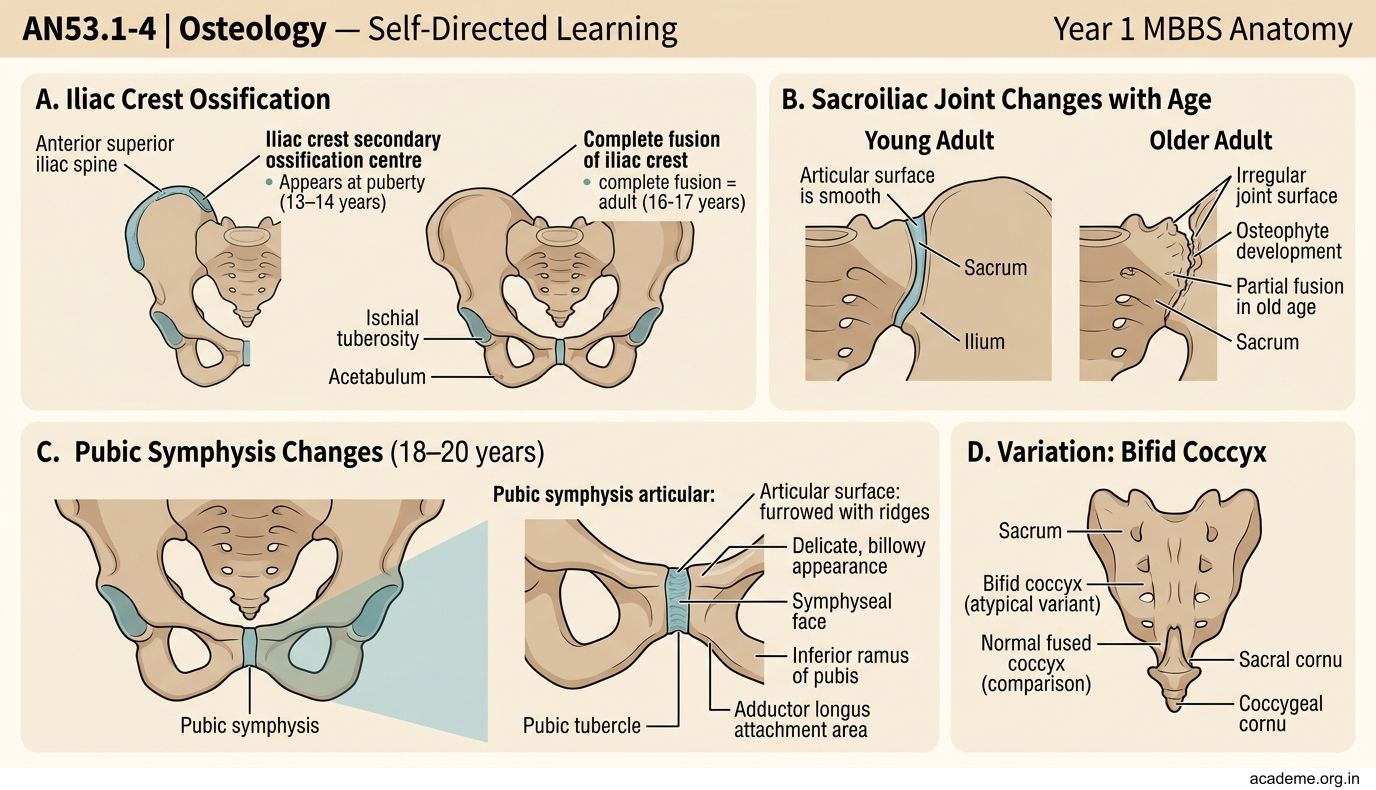
Figure: Obstructed Labour — How the Android Pelvis Causes Problems
CLINICAL PEARL
Obstructed Labour — How the Android Pelvis Causes Problems
In the android pelvis, the inlet is heart-shaped with a narrowed anterior segment. This has three consequences for labour:
- Engagement difficulty: The fetal head, which is ovoid (wider in the transverse dimension), cannot enter a heart-shaped inlet where the anterior segment is narrowed — it tends to engage in the transverse or posterior position.
- Deep transverse arrest: Even if the head engages, rotation to the occiput anterior (OA) position in the mid-pelvis is impeded by prominent ischial spines — the head gets stuck in the transverse position.
- Outlet obstruction: The subpubic angle of <90° means the pubic arch is too narrow for the head to extend out at delivery.
Clinical management:
• Diagonal conjugate measurement on first antenatal visit (per vaginum)
• If diagonal conjugate <11.5 cm → plan caesarean section before labour
• If deep transverse arrest occurs in labour → ventouse or forceps rotation, or emergency LSCS
In India, cephalopelvic disproportion (CPD) from android and platypelloid pelvic types accounts for a significant proportion of emergency caesarean sections — particularly in primigravidas from regions where nutritional stunting during childhood affected pelvic development.
REFLECT
Return to the hook case — the primigravida with android pelvis and obstructed labour:
- The diagonal conjugate measured 10.5 cm. What is the obstetric conjugate, and is it adequate for vaginal delivery?
- The subpubic angle of 70° is less than normal. What does this tell you about the pelvic outlet, and which muscles attach to the pubic arch?
- Prominent ischial spines are noted on examination. What is the significance of prominent ischial spines in the mid-pelvis during labour?
- The obstetrician notes the sacrum is straight (not curved). How does a straight, flat sacrum affect the pelvic cavity dimensions?
Discussion: Obstetric conjugate = diagonal conjugate − 1.5 cm = 10.5 − 1.5 = 9 cm → below the minimum adequate 10 cm → CPD. Subpubic angle of 70° = narrow pubic arch; compressor urethrae and urogenital diaphragm muscles attach to the pubic arch; the narrow angle reduces the outlet AP dimension. Prominent ischial spines reduce the inter-spinous diameter (normal 10.5 cm) → can cause deep transverse arrest. A straight (flat) sacrum reduces the posterior pelvic space, further decreasing the cavity dimensions.
KEY TAKEAWAYS
Key Takeaways — Osteology (AN53.1–53.4)
Bone Identification:
• Anatomical position = position in the living erect human
• Lumbar vertebra: large kidney-shaped body, horizontal hatchet spinous process, medially-facing superior articular facets
• Sacrum: concave pelvic surface anteriorly, promontory on S1 superiorly, auricular surface laterally
Bony Pelvis (AN53.2):
• Inlet: bounded by sacral promontory (posterior) → arcuate line → pectineal line → pubic symphysis (anterior)
• Obstetric conjugate (10.5 cm) = smallest AP inlet diameter; estimated from diagonal conjugate (12.5 cm) minus 1.5 cm
• Pelvis tilted 60° in anatomical position; ASIS and pubic symphysis in same coronal plane
Sex Determination (AN53.3):
• Female: subpubic angle >90°, wide sciatic notch, round inlet, non-prominent ischial spines
• Male: subpubic angle <90°, narrow sciatic notch, heart-shaped inlet, prominent ischial spines
Clinical Importance (AN53.4):
• 4 pelvic types: Gynaecoid (best for birth), Android (worst), Anthropoid, Platypelloid
• Sacralisation (L5 → sacrum): 10%, causes low back pain, confuses epidural counting
• Lumbarisation (S1 → 6th lumbar): 5%, similar problems
• Coccydynia: treated conservatively; coccyx moves back 2 cm in delivery