Page 1 of 4
AN56.1-2 | Meninges & CSF — SDL Guide
Learning Objectives
- Describe and identify the layers of meninges, their extent, and dural modifications including folds, sinuses, and reflections (AN56.1)
- Describe the formation, circulation, and absorption of CSF with applied anatomy including hydrocephalus and lumbar puncture (AN56.2)
INSTRUCTIONS
Study meninges in conjunction with the base of skull and dural venous sinuses. The CSF circulation pathway must be traced step by step — it is a high-yield topic in university examinations.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Gray's Anatomy for Students — Meninges and CSF (Textbook)
- Inderbir Singh's Human Neuroanatomy, Chapter on Meninges (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 5-year-old child from Vellore is brought to the paediatric casualty with fever for 3 days, severe headache, neck stiffness (nuchal rigidity), and photophobia. A petechial rash is noted on the trunk. CSF examination after urgent lumbar puncture reveals: turbid fluid, pressure 300 mm H₂O (raised), protein 180 mg/dL (raised), glucose 20 mg/dL (low), neutrophilic pleocytosis.
Diagnosis: Bacterial meningitis (Neisseria meningitidis).
Why does inflammation of the meninges cause headache and neck stiffness? Why is lumbar puncture performed at L3–L4 and not higher? How does meningitis affect CSF pressure?
Understanding meningeal anatomy answers all these questions.
WHY THIS MATTERS
Meninges and CSF knowledge is essential for clinical practice in India:
- Bacterial meningitis — a medical emergency; TBM (tuberculous meningitis) is the most important cause in India, especially in children
- Lumbar puncture — performed daily in Indian hospitals for CSF analysis; safe anatomy at L3–L4 (below spinal cord end)
- Hydrocephalus — congenital hydrocephalus from aqueduct stenosis is the most common indication for VP shunting in Indian paediatric neurosurgery
- Subdural vs extradural haematoma — the meningeal layers determine the space in which blood collects; affects prognosis and surgical urgency
- Epidural anaesthesia — the epidural (extradural) space is entered for obstetric and surgical pain relief in Indian hospitals daily
RECALL
Before we begin, recall:
- The brain and spinal cord are contained within the cranium and vertebral canal respectively
- Meninges = three protective membranes surrounding the CNS
- CSF is a clear, colourless fluid produced primarily in the choroid plexus
- Hydrocephalus = excess CSF accumulation causing raised intracranial pressure
Part 1: Layers of the Meninges (AN56.1)
Three Meningeal Layers (outer to inner)

Figure: Part 1: Layers of the Meninges (AN56.1)
1. Dura Mater ("tough mother")
• Outermost; thick, tough, fibrous
• In the cranium: two layers — periosteal layer (adheres to skull) + meningeal layer (forms dural folds)
• In the spine: single layer (periosteal layer is separate periosteum of vertebral canal)
• Dural folds (septa):
- Falx cerebri — sickle-shaped vertical fold separating the two cerebral hemispheres in the midline sagittal plane; attaches from crista galli (anteriorly) to internal occipital protuberance (posteriorly)
- Tentorium cerebelli — tent-shaped horizontal fold separating cerebrum (above) from cerebellum (below); has a gap — tentorial notch (incisura) — for the midbrain; the free edge of the tentorium forms the tentorial notch
- Falx cerebelli — smaller vertical fold between the two cerebellar hemispheres
- Diaphragma sellae — horizontal fold over the pituitary fossa (sella turcica); has a central opening for the pituitary stalk
• Clinical — Transtentorial herniation (uncal herniation): In raised ICP, the medial temporal lobe (uncus) herniates through the tentorial notch, compressing the ipsilateral CN III (dilated pupil, "blown pupil") and midbrain → coning
Dural Venous Sinuses (within dural folds):
| Sinus | Location |
|---|---|
| Superior sagittal sinus | Upper border of falx cerebri |
| Inferior sagittal sinus | Lower border of falx cerebri |
| Straight sinus | Junction of falx cerebri + tentorium cerebelli |
| Transverse sinuses | Posterior margin of tentorium |
| Sigmoid sinuses | S-shaped; continue from transverse → internal jugular vein |
| Cavernous sinus | Either side of the sella; contains CN III, IV, V1, V2, VI + ICA |
| Confluence of sinuses | Where straight + superior sagittal + occipital sinuses meet |
2. Arachnoid Mater ("spider web")
• Middle layer; thin, delicate, avascular
• Subarachnoid space = between arachnoid and pia mater; contains CSF, blood vessels, and cranial nerve roots
• Arachnoid granulations (Pacchionian bodies) — tufted projections of arachnoid into the superior sagittal sinus → site of CSF absorption
• Cisterns = enlarged subarachnoid spaces:
- Cisterna magna (cerebellomedullary cistern) — between cerebellum and medulla
- Pontine cistern — anterior to pons
- Interpeduncular cistern — between cerebral peduncles
- Cistern of the lateral fossa — over the Sylvian fissure
3. Pia Mater ("tender mother")
• Innermost; thin, vascular; closely covers the brain surface and dips into every sulcus
• Spinal pia: forms the denticulate ligaments (lateral projections that anchor the spinal cord to the dura, preventing excessive movement) and the filum terminale (condensed pia from conus medullaris to coccyx)
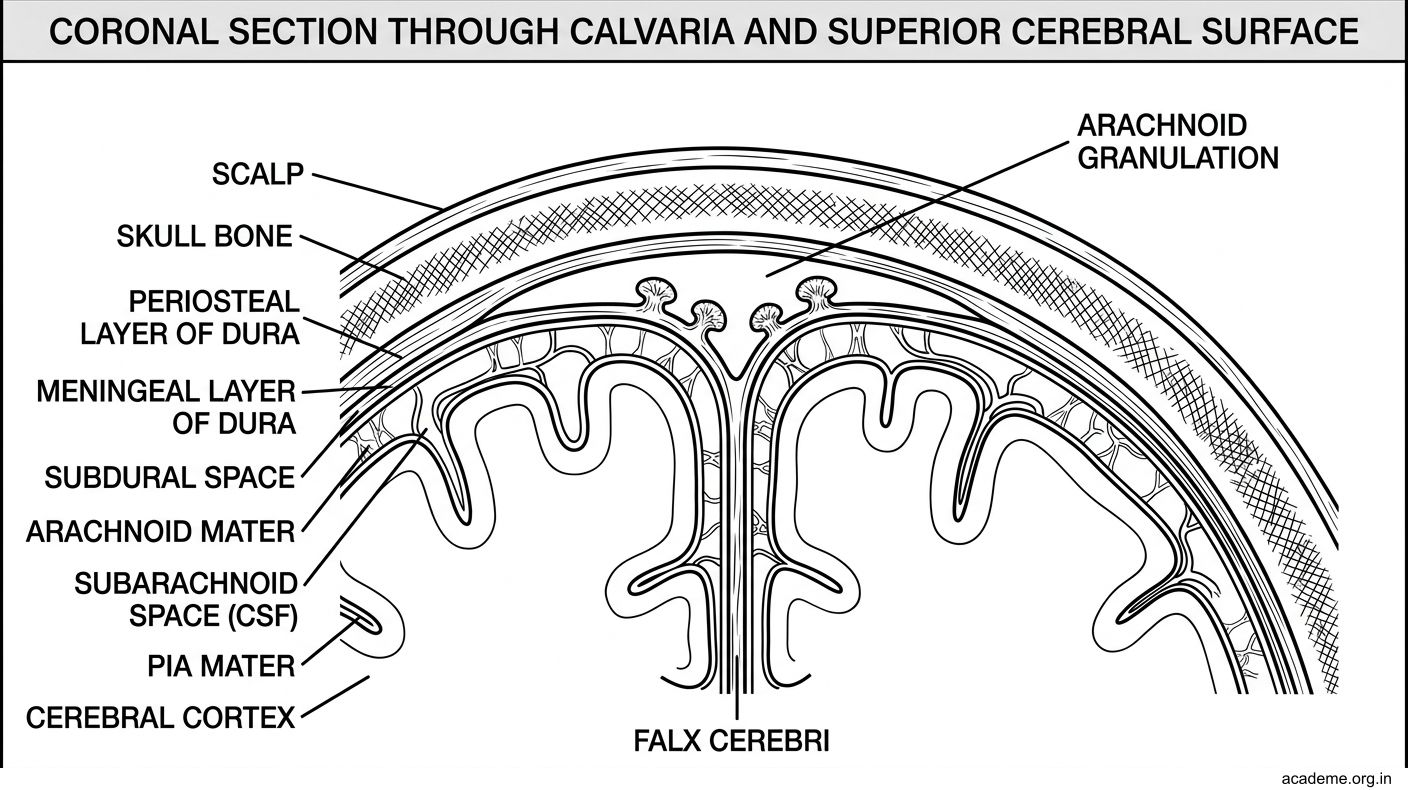
Figure: Part 1: Layers of the Meninges (AN56.1)

Figure: Dural Venous Sinuses (within dural folds):
Part 2: CSF — Formation, Circulation, Absorption (AN56.2)
Formation of CSF
• Produced mainly by the choroid plexus (specialised ependymal cells + capillary tufts) in the lateral ventricles (most), 3rd ventricle, and 4th ventricle
• Rate: ~500 mL/day; total volume at any time: 125–150 mL
• Composition: clear, colourless; glucose 2/3 of plasma; protein low (15–45 mg/dL); no RBCs; few lymphocytes

Figure: Part 2: CSF — Formation, Circulation, Absorption (AN56.2)
Circulation of CSF — Step by Step:
1. Lateral ventricles (most CSF produced here)
2. → Through interventricular foramina of Monro → 3rd ventricle
3. → Through cerebral aqueduct of Sylvius (in midbrain) → 4th ventricle
4. → Through foramina of Magendie (median) and foramina of Luschka (lateral, ×2) → subarachnoid space
5. → Circulates around the brain and spinal cord in the subarachnoid space
6. → Absorbed at arachnoid granulations into the superior sagittal sinus
Normal CSF pressure: 70–180 mm H₂O (measured at LP in lateral decubitus position)
Absorption: Arachnoid granulations act as one-way valves — CSF absorbed into venous blood when CSF pressure exceeds venous pressure.
Hydrocephalus — Types and Causes:
| Type | Mechanism | Cause |
|---|---|---|
| Obstructive (non-communicating) | Blockage within CSF pathway | Aqueduct stenosis (congenital), tumour at 4th ventricle (medulloblastoma) |
| Communicating | Impaired absorption at arachnoid granulations | Post-meningitis (scarring), subarachnoid haemorrhage, choroid plexus papilloma (overproduction) |
| Normal pressure hydrocephalus (NPH) | Impaired absorption, normal pressure at LP | Triad: Wet (incontinence) + Wobbly (gait ataxia) + Wacky (dementia) — in elderly |
Lumbar Puncture — Anatomical Basis:
• The spinal cord ends at L1–L2 in adults (L3 in neonates)
• LP is done at L3–L4 or L4–L5 interspace → needle enters the lumbar cistern (subarachnoid space of the cauda equina)
• Safe because there is no spinal cord at this level — only the cauda equina nerve roots, which float aside
• Layers pierced (posterior → anterior): skin → fascia → supraspinous ligament → interspinous ligament → ligamentum flavum → epidural space (fat + veins) → dura → arachnoid → subarachnoid space (CSF)
• Complications: Post-LP headache (CSF leak through dural hole), infection, epidural haematoma
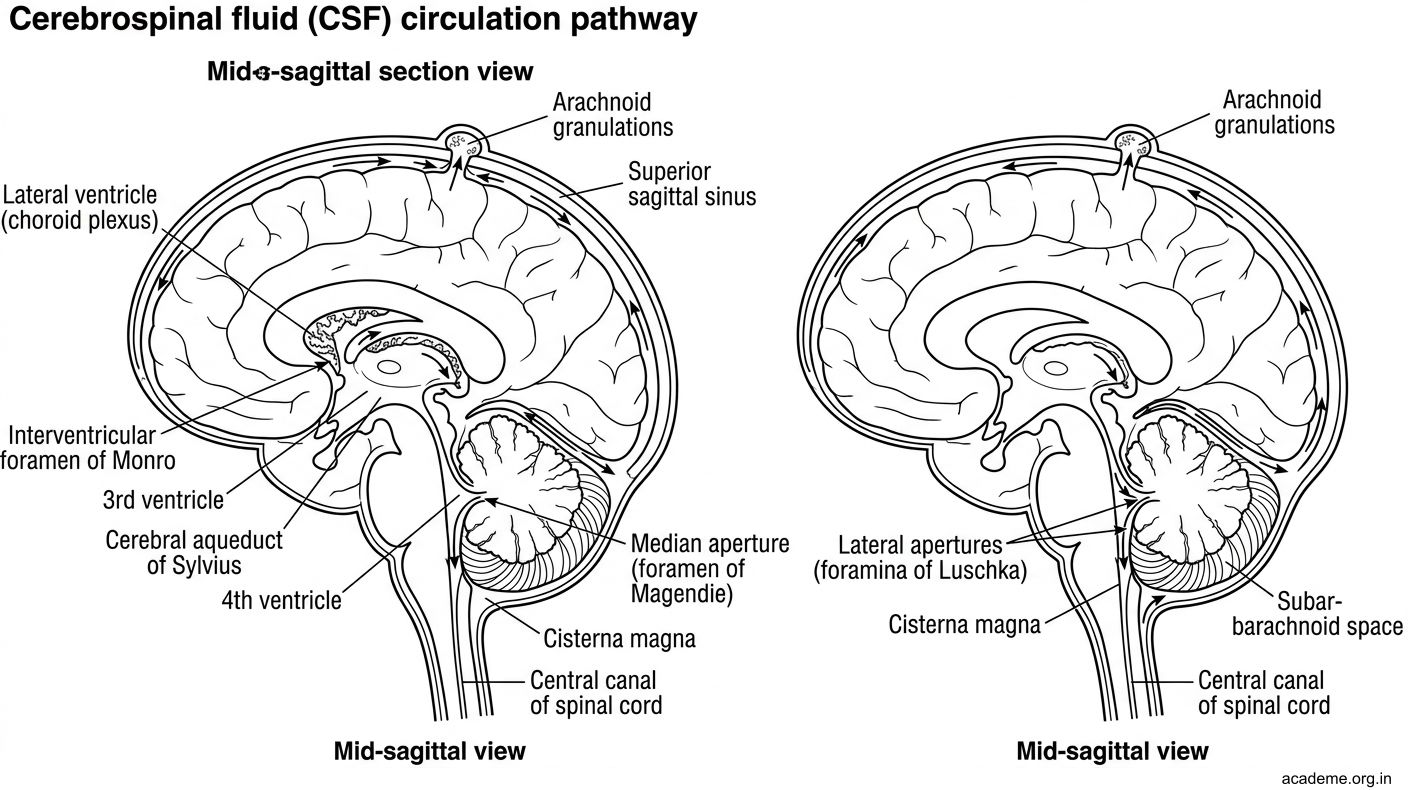
Figure: Part 2: CSF — Formation, Circulation, Absorption (AN56.2)

Figure: Hydrocephalus — Types and Causes:

Figure: CSF Analysis in Indian Clinical Practice
SELF-CHECK — : Meninges & CSF
The foramen of Magendie connects which two CSF spaces?
A. Lateral ventricle → 3rd ventricle
B. 3rd ventricle → 4th ventricle via aqueduct
C. 4th ventricle → subarachnoid space (cisterna magna)
D. Subarachnoid space → superior sagittal sinus
Reveal Answer
Answer: C. 4th ventricle → subarachnoid space (cisterna magna)
Which structure is NOT contained within the cavernous sinus?
A. CN VI (abducens)
B. Internal carotid artery
C. CN III (oculomotor)
D. CN XII (hypoglossal)
Reveal Answer
Answer: D. CN XII (hypoglossal)
In obstructive (non-communicating) hydrocephalus due to aqueduct stenosis, which ventricle(s) dilate?
A. 4th ventricle only
B. Lateral and 3rd ventricles (upstream of the block)
C. All four ventricles equally
D. 4th ventricle and subarachnoid space
Reveal Answer
Answer: B. Lateral and 3rd ventricles (upstream of the block)
CLINICAL PEARL
CSF Analysis in Indian Clinical Practice
| Parameter | Normal | Bacterial Meningitis | Viral Meningitis | TBM |
|---|---|---|---|---|
| Appearance | Clear | Turbid | Clear | Turbid/viscous |
| Pressure | 70–180 mmH₂O | Raised | Normal/raised | Raised |
| Cells | 0–5 lymphocytes | 100–50,000 neutrophils | 10–1000 lymphocytes | 100–500 lymphocytes |
| Protein | 15–45 mg/dL | Raised (>100) | Normal/slightly raised | Raised |
| Glucose (CSF:serum ratio) | 0.6 | Low (<0.3) | Normal | Very low |
| Other | — | Culture positive | PCR viral | AFB smear/culture; fibrin web |
India-specific: TBM is the most important cause of chronic meningitis in India. Classic findings: lymphocytic pleocytosis + very high protein + very low glucose + cobweb clot in CSF. ADA (adenosine deaminase) levels are elevated. Start anti-TB treatment without waiting for culture confirmation.
REFLECT
Return to the hook case — the 5-year-old with bacterial meningitis:
- Which layer of meninges is inflamed in meningitis? Why does this cause headache (which sensory nerve innervates the meninges)?
- Why is LP done at L3–L4 and not L1–L2 in this child?
- The CSF pressure is 300 mm H₂O. Through which structure is CSF normally absorbed, and why does infection impair this?
- If the child later develops hydrocephalus, trace the CSF pathway and identify where the block would be in communicating post-meningitic hydrocephalus.
Discussion: Meningeal pain is transmitted by the trigeminal nerve (supratentorial dura) and upper cervical nerves (posterior fossa + spinal dura) — hence headache and neck stiffness. LP at L3–L4 is safe because the spinal cord ends at L1–L2 (even lower at L3 in neonates). Post-meningitic communicating hydrocephalus: arachnoid granulations become scarred → impaired CSF absorption → all CSF spaces dilate.
KEY TAKEAWAYS
Key Takeaways — Meninges & CSF
- Layers: Dura (outer, tough) → Arachnoid (middle, avascular) → Pia (inner, vascular, on brain surface)
- Dural folds: Falx cerebri (L/R hemispheres), Tentorium cerebelli (cerebrum/cerebellum), Diaphragma sellae (pituitary)
- Dangerous spaces: Extradural (between skull/dura — extradural haematoma, middle meningeal artery), Subdural (between dura/arachnoid — bridging veins), Subarachnoid (CSF — SAH)
- CSF path: Choroid plexus (lateral ventricles) → Foramen of Monro → 3rd ventricle → Aqueduct of Sylvius → 4th ventricle → Magendie (median) + Luschka (lateral) → subarachnoid space → arachnoid granulations → superior sagittal sinus
- LP level: L3–L4 or L4–L5 (spinal cord ends L1–L2)
- Hydrocephalus: Obstructive (aqueduct stenosis) vs Communicating (post-meningitis, post-SAH)