Page 1 of 4
AN57.1-5 | Spinal Cord — SDL Guide
Learning Objectives
- Identify and describe the external features of the spinal cord (AN57.1)
- Describe the extent of the spinal cord in the child and adult with clinical implications (AN57.2)
- Draw and label transverse sections of the spinal cord at mid-cervical and mid-thoracic levels (AN57.3)
- Enumerate the ascending and descending tracts at the mid-thoracic level (AN57.4)
- Describe the anatomical basis of spinal cord clinical conditions: Brown-Séquard, Poliomyelitis, ALS, Syringomyelia, Subacute Combined Degeneration, Transverse myelitis, Paraplegia (AN57.5)
INSTRUCTIONS
Draw the transverse sections as you study. The tract diagrams must be mastered before studying the clinical syndromes — each syndrome is simply a "lesion map" on the cross-section.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
- Gray's Anatomy for Students — Spinal Cord (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
Three patients admitted to a neurology ward in Chennai:
Patient 1 (28-year-old woman): Road traffic accident. Has loss of pain and temperature on the LEFT side of the body below T6, and weakness + loss of proprioception on the RIGHT side below T6. Right ankle reflex absent.
Patient 2 (45-year-old man): Chronic alcoholic. Has weakness of both legs (spastic paraplegia), brisk knee and ankle jerks, positive Babinski, and loss of vibration sense and proprioception in both legs. Serum B12 = 80 pg/mL (severely low).
Patient 3 (9-year-old boy): Developed fever 2 weeks ago. Now has flaccid paralysis of the right leg with absent knee jerk. No sensory loss.
Each patient has a specific spinal cord syndrome. Can you identify which syndrome each patient has — and which tracts/grey matter regions are involved?
WHY THIS MATTERS
The spinal cord is clinically critical in Indian neurology practice:
- Spinal cord injury from RTAs is a leading cause of permanent disability in India; tracts must be known for prognostication
- Poliomyelitis — India was endemic; AFP (acute flaccid paralysis) surveillance is ongoing for wild poliovirus
- Subacute combined degeneration (SCD) — B12 deficiency (common in Indian vegetarians) destroys posterior and lateral columns
- TB of spine (Pott's disease) — most common cause of paraplegia in young Indians
- Syringomyelia — cape-like loss of pain/temperature; associated with Chiari malformation (neurosurgically correctable)
RECALL
Before we begin, recall:
- Spinal cord is part of the CNS, continuous with the medulla oblongata at the foramen magnum
- It is surrounded by meninges and CSF within the vertebral canal
- Grey matter (cell bodies) is inside; white matter (myelinated axons) surrounds it
- 31 pairs of spinal nerves: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal
Part 1: External Features (AN57.1) & Extent (AN57.2)
External Features of the Spinal Cord
- Cylindrical structure, ~45 cm long, ~1 cm diameter
- Two enlargements (where limb nerves arise):
- Cervical enlargement (C4–T1) — supplies upper limb via brachial plexus
- Lumbar (lumbosacral) enlargement (L1–S3) — supplies lower limb via lumbar and sacral plexuses
- Tapers inferiorly to form the conus medullaris (cone-shaped tip)
- Filum terminale — slender thread of pia mater extending from the conus to the coccyx
- Cauda equina — bundle of lumbar and sacral nerve roots below the conus, resembling a horse's tail
Surface features:
• Anterior median fissure — deep longitudinal groove anteriorly
• Posterior median sulcus — shallow groove posteriorly
• Anterolateral sulcus — where ventral nerve roots emerge
• Posterolateral sulcus — where dorsal nerve roots enter
Extent in Child vs Adult (AN57.2):
| Neonates | Adults | |
|---|---|---|
| Conus medullaris level | L2–L3 | L1–L2 (lower border of L1) |
| Reason for difference | Vertebral column grows faster than spinal cord postnatally | — |
Clinical implication:
• LP in adults = L3–L4 or L4–L5 (safe)
• LP in neonates = L4–L5 (conus is at L2–L3)
• Spinal anaesthesia injected below the conus level avoids cord injury
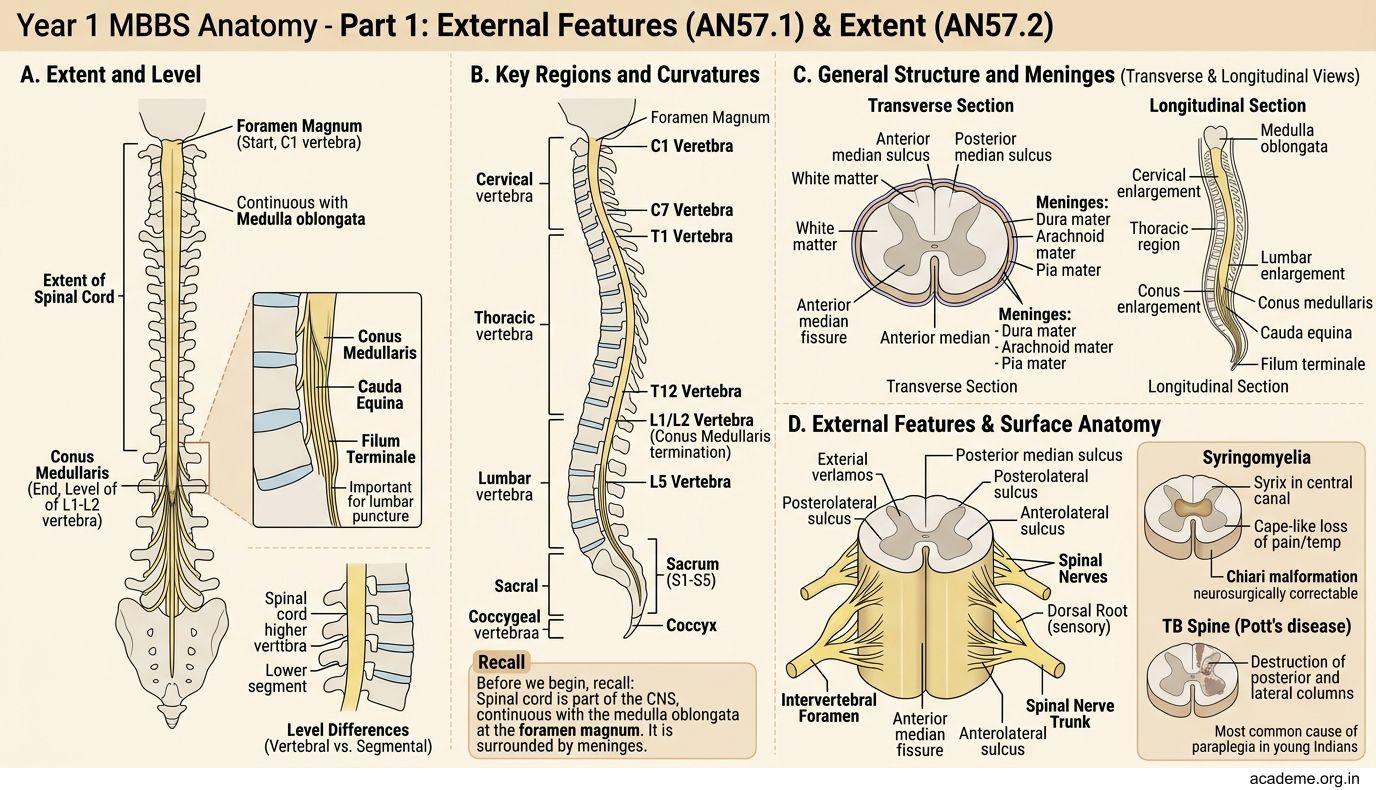
Figure: External Features of the Spinal Cord
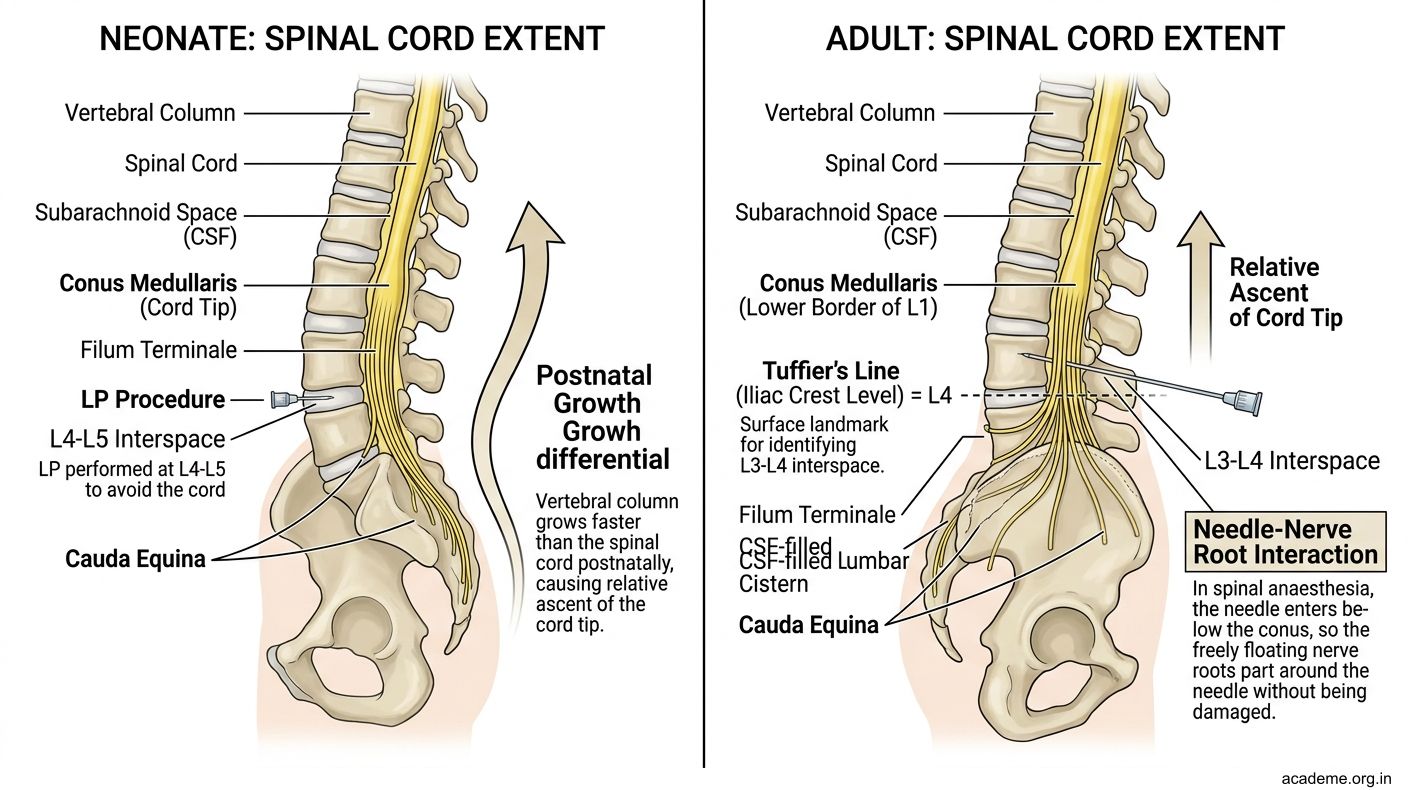
Figure: Extent in Child vs Adult (AN57.2):
Part 2: Transverse Sections (AN57.3) — Mid-Cervical vs Mid-Thoracic
Grey Matter — "H" or "Butterfly" Shape
- Anterior horn (ventral) — motor; contains large multipolar LMNs (alpha motor neurons)
- Large in cervical and lumbar enlargements (more limb muscles)
- Posterior horn (dorsal) — sensory; receives afferent input
- Lateral horn — present ONLY at T1–L2 (sympathetic preganglionic neurons) and S2–S4 (parasympathetic)
- Commissures — grey commissure (connects left and right grey matter, contains central canal)
Rexed Laminae (I–X):
| Laminae | Location | Function |
|---|---|---|
| I–IV | Posterior horn | Somatic sensory input |
| V–VI | Base of posterior horn | Proprioception, pain modulation |
| VII | Intermediate zone | Clarke's nucleus (spinocerebellar), IML (T1–L2) |
| VIII–IX | Anterior horn | Motor output (LMNs in IX) |
| X | Around central canal | Commissural neurons |
Mid-cervical section (e.g., C6):
• Large anterior horns (limb muscles)
• Large posterior horns
• NO lateral horn (sympathetic is only T1–L2)
• White matter is LARGE relative to grey (many ascending/descending fibres traversing)
Mid-thoracic section (e.g., T6):
• Small anterior horns (only trunk muscles)
• Small posterior horns
• Lateral horn present (T1–L2 sympathetic IML)
• White matter is still large (all ascending/descending tracts present)
• Clarke's column (nucleus dorsalis, Lamina VII) present at T1–L2/L3 — origin of posterior spinocerebellar tract
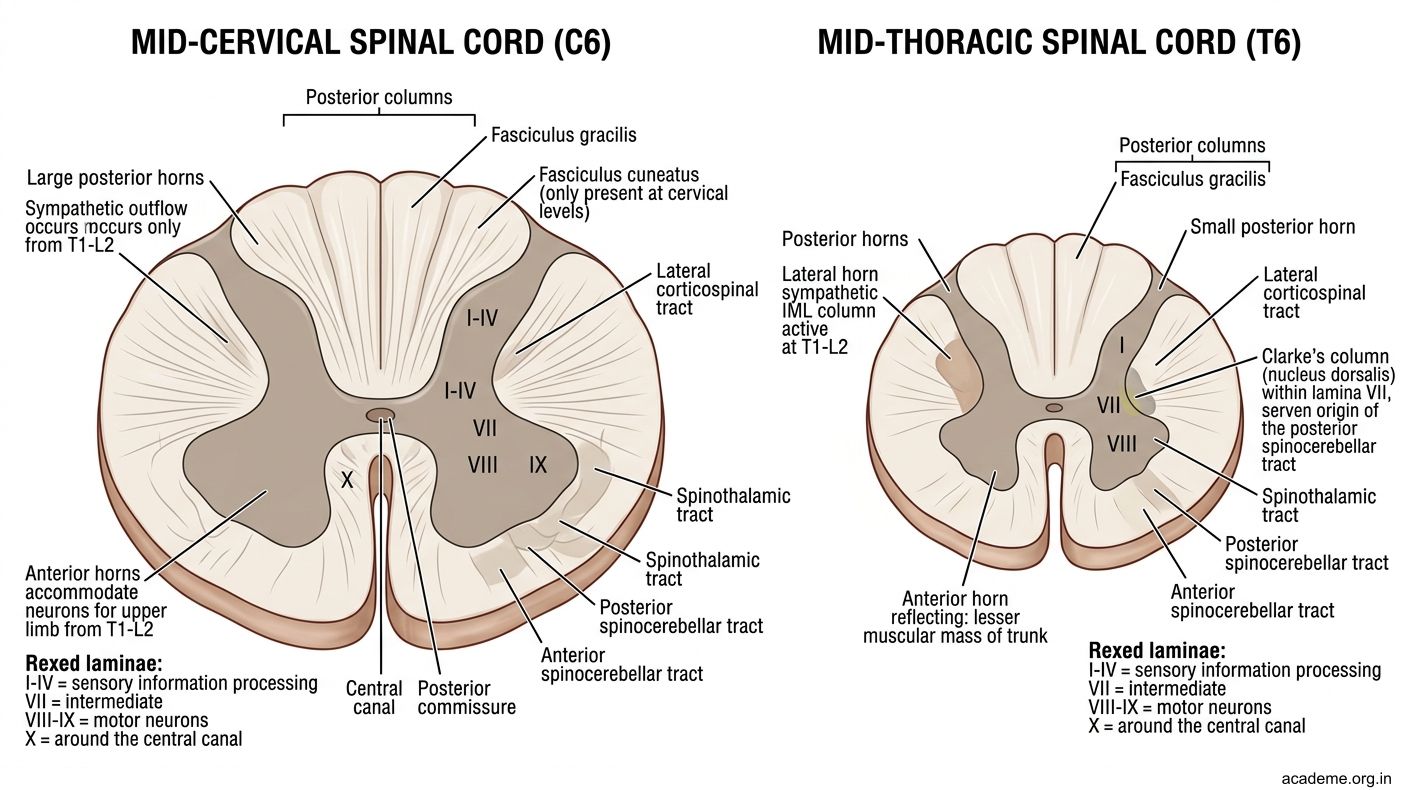
Figure: Part 2: Transverse Sections (AN57.3) — Mid-Cervical vs Mid-Thoracic
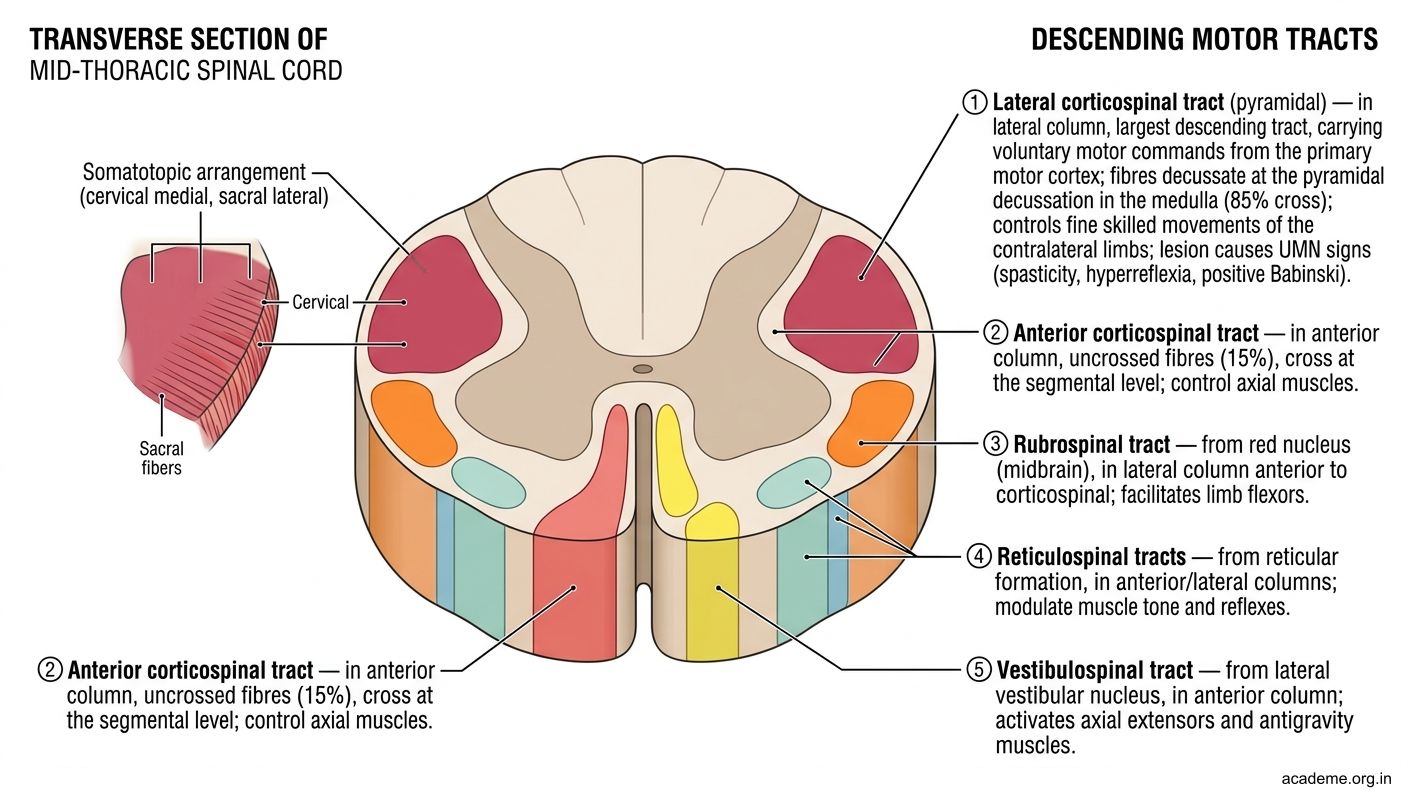
Figure: Rexed Laminae (I–X):
Part 3: Ascending and Descending Tracts at Mid-Thoracic Level (AN57.4)
ASCENDING TRACTS (Sensory — from body to brain)

Figure: Part 3: Ascending and Descending Tracts at Mid-Thoracic Level (AN57.4)
Posterior (Dorsal) White Columns — Medial Lemniscal Pathway
• Fasciculus gracilis (medial) — lower limb and lower trunk (T7 and below); carries fine touch, vibration, proprioception, 2-point discrimination
• Fasciculus cuneatus (lateral) — upper limb and upper trunk (above T7); same modalities
• Neurons: 1st order in DRG → ascend IPSILATERAL in posterior column → synapse in medullary nuclei (nucleus gracilis/cuneatus) → cross in medial lemniscus → thalamus (VPL) → somatosensory cortex
Spinothalamic Tracts — Anterolateral System
• Lateral spinothalamic tract — pain and temperature (sharp pain, temperature)
• Anterior spinothalamic tract — crude touch and pressure
• Neurons: 1st order DRG → enter posterior horn → CROSS in anterior white commissure (within 1–2 spinal segments) → ascend in contralateral anterolateral column → thalamus (VPL) → cortex
Spinocerebellar Tracts (at mid-thoracic level):
• Posterior spinocerebellar tract (lateral white column, posterior part) — proprioception, ipsilateral, via inferior cerebellar peduncle; origin: Clarke's column
• Anterior spinocerebellar tract (lateral white column, anterior part) — proprioception, bilateral; via superior cerebellar peduncle
DESCENDING TRACTS (Motor — from brain to spinal cord)
Corticospinal Tracts (Pyramidal System)
• Lateral corticospinal tract — 85% of pyramidal fibres; crossed (decussate at medulla); in lateral white column; controls fine skilled voluntary movements (especially hand)
• Anterior corticospinal tract — 15%; uncrossed initially; in anterior white column; for trunk muscles (crosses near target)
Extrapyramidal Descending Tracts:
• Rubrospinal tract — from red nucleus (midbrain); in lateral column anterior to corticospinal; facilitates limb flexors
• Reticulospinal tracts — from reticular formation; in anterior/lateral columns; modulate muscle tone, reflexes, ANS
• Vestibulospinal tract — from lateral vestibular nucleus; in anterior column; activates axial extensors, antigravity muscles
• Tectospinal tract — from superior colliculus; head-turning reflexes in response to visual/auditory stimuli
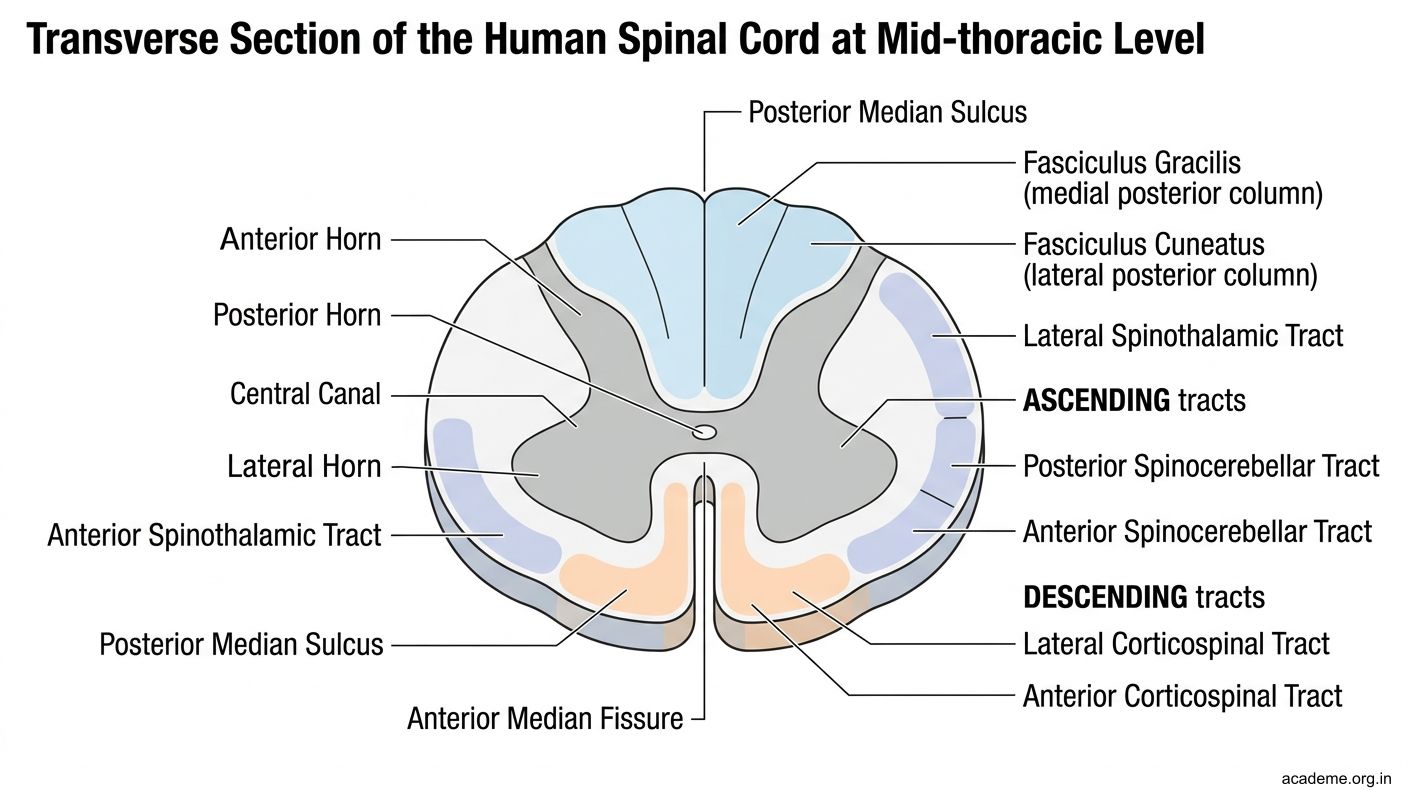
Figure: Part 3: Ascending and Descending Tracts at Mid-Thoracic Level (AN57.4)
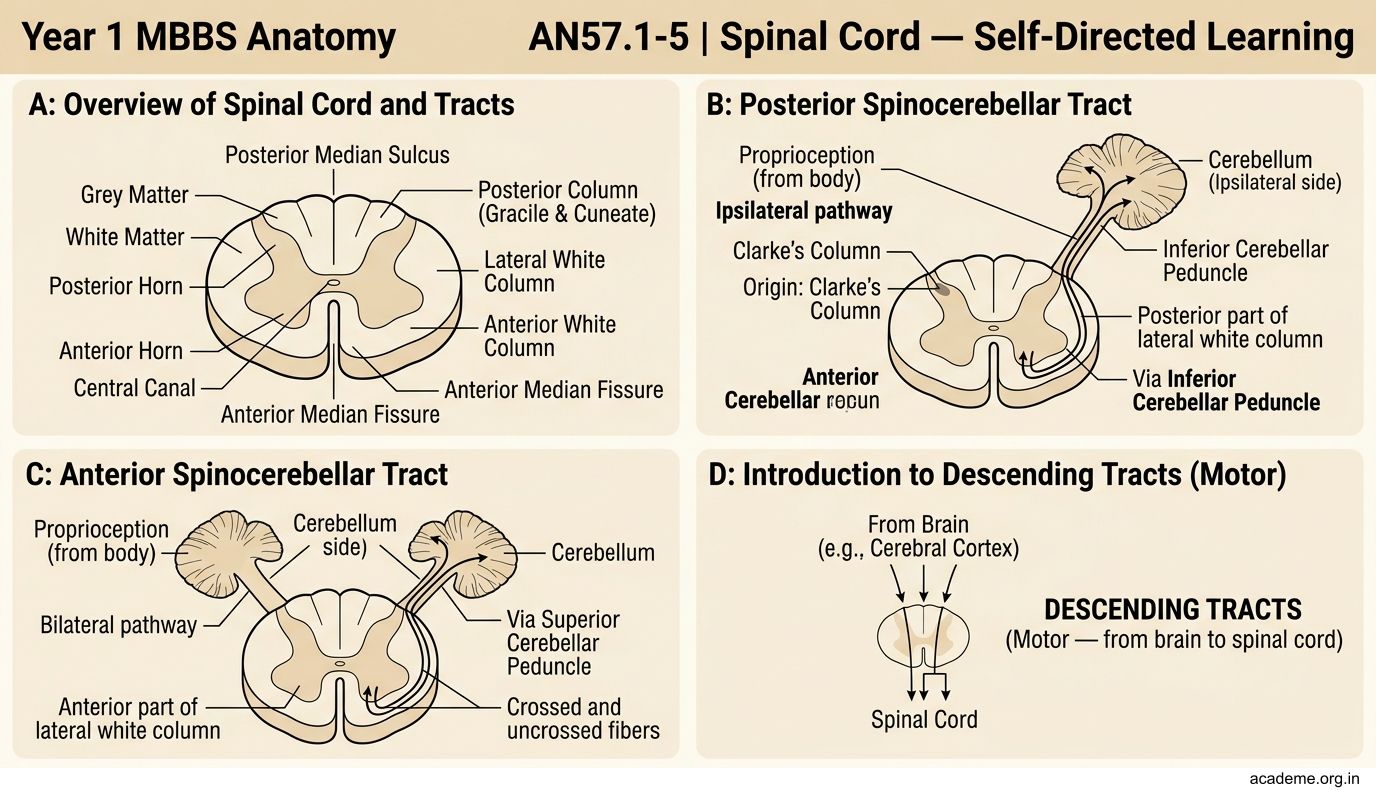
Figure: DESCENDING TRACTS (Motor — from brain to spinal cord)
Part 4: Spinal Cord Syndromes (AN57.5)
1. Brown-Séquard Syndrome (Hemisection of Spinal Cord)
• Cause: stab wound, tumour on one side, MS plaque
• Ipsilateral (same side as lesion): UMN paralysis + loss of proprioception/vibration (posterior column ipsilateral)
• Contralateral (opposite side): loss of pain and temperature (spinothalamic crosses 1–2 segments above entry)
• Patient 1 in the hook: Right hemisection at T6 — right side: LMN (at level) + UMN below; left side: loss of pain/temperature below T6
2. Subacute Combined Degeneration of the Cord (SCD)
• Cause: Vitamin B12 deficiency (commonest in Indian vegetarians) → demyelination of posterior and lateral columns
• Posterior columns: loss of proprioception, vibration, sensory ataxia
• Lateral corticospinal tracts: spastic paraplegia, brisk reflexes, Babinski+
• NOTE: reflexes may be diminished if peripheral neuropathy co-exists
• Patient 2 in the hook: SCD from B12 deficiency
3. Poliomyelitis
• Cause: Poliovirus destroys anterior horn cells (LMNs) selectively
• Features: Flaccid paralysis, absent reflexes, NO sensory loss (sensory neurons spared)
• Patient 3 in the hook: Anterior horn cell destruction at lumbar level
4. Amyotrophic Lateral Sclerosis (ALS / Motor Neuron Disease)
• Cause: Degeneration of both UMN (corticospinal tract) and LMN (anterior horn cells)
• Features: UMN + LMN signs co-existing (spasticity + fasciculations + wasting) — NO sensory loss
5. Syringomyelia
• Cause: Fluid-filled cavity (syrinx) in the centre of the cord, expanding from central canal
• Affects: Anterior white commissure first (pain and temperature fibres as they cross) → "cape distribution" bilateral loss of pain/temperature over shoulders/arms
• Late: anterior horn → LMN weakness in arms; posterior columns may be spared initially
• Association: Chiari malformation (cerebellar tonsils herniate through foramen magnum)
6. Transverse Myelitis
• Cause: Inflammatory/demyelinating lesion (MS, NMO, post-infection) affecting entire cross-section
• Features: Bilateral UMN paralysis + complete sensory loss below the level + bladder/bowel dysfunction
Summary Lesion Map:
| Syndrome | Tract(s) Affected | Sensory Loss | Motor Loss |
|---|---|---|---|
| Brown-Séquard | Ipsi posterior + lateral column; contra spinothalamic | Ipsi: vibrn/prop; Contra: pain/temp | Ipsi: UMN |
| SCD (B12) | Posterior + lateral columns bilat | Bilat: vibrn/prop | Bilat: UMN (spastic) |
| Polio | Anterior horn only | None | LMN (flaccid) |
| ALS | Anterior horn + corticospinal bilat | None | Mixed UMN+LMN |
| Syringomyelia | Anterior commissure | Cape: pain/temp bilat | Late LMN arms |
| Transverse myelitis | All tracts | All modalities below | Bilat UMN |
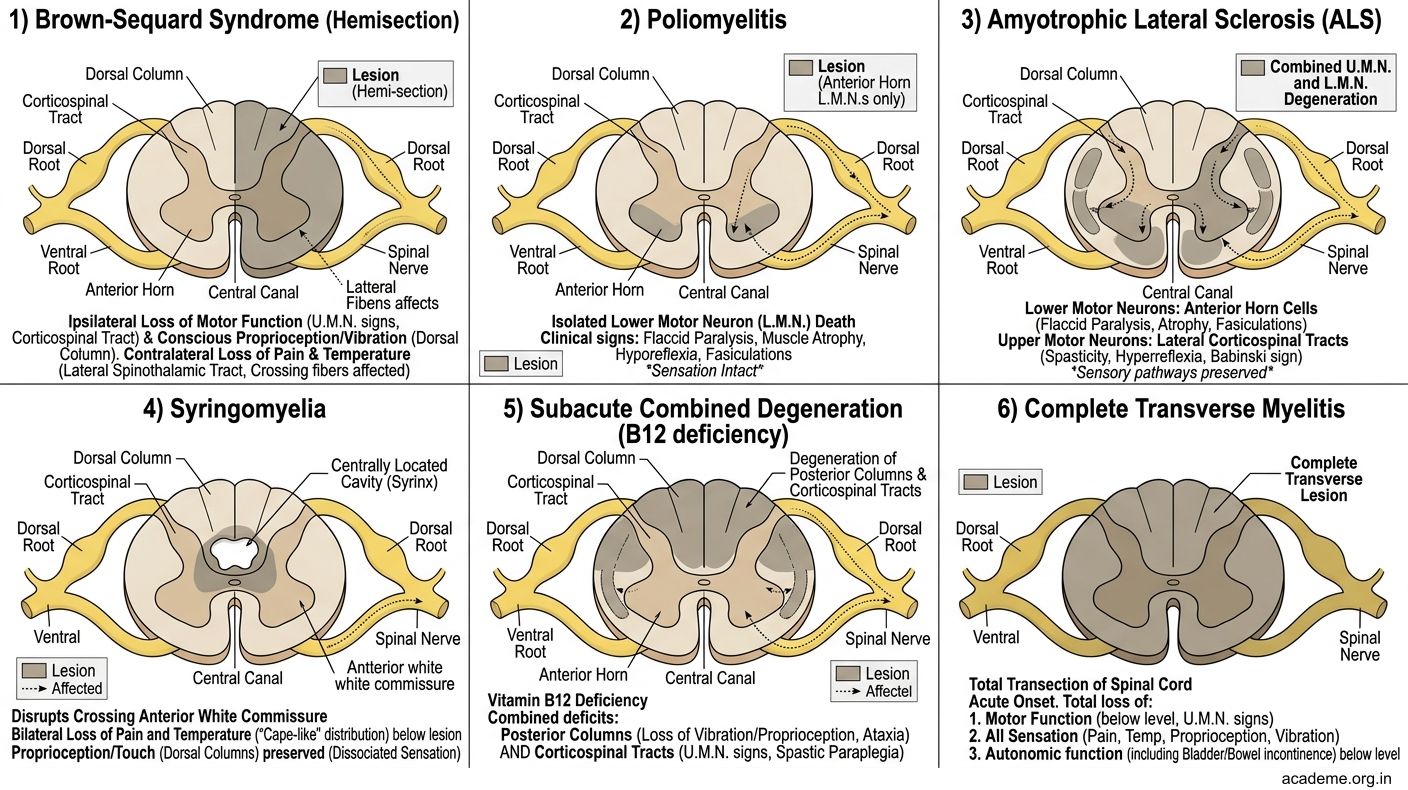
Figure: Part 4: Spinal Cord Syndromes (AN57.5)

Figure: Spinal Shock vs Neurogenic Shock — Distinction for Indian Emergency Medicine
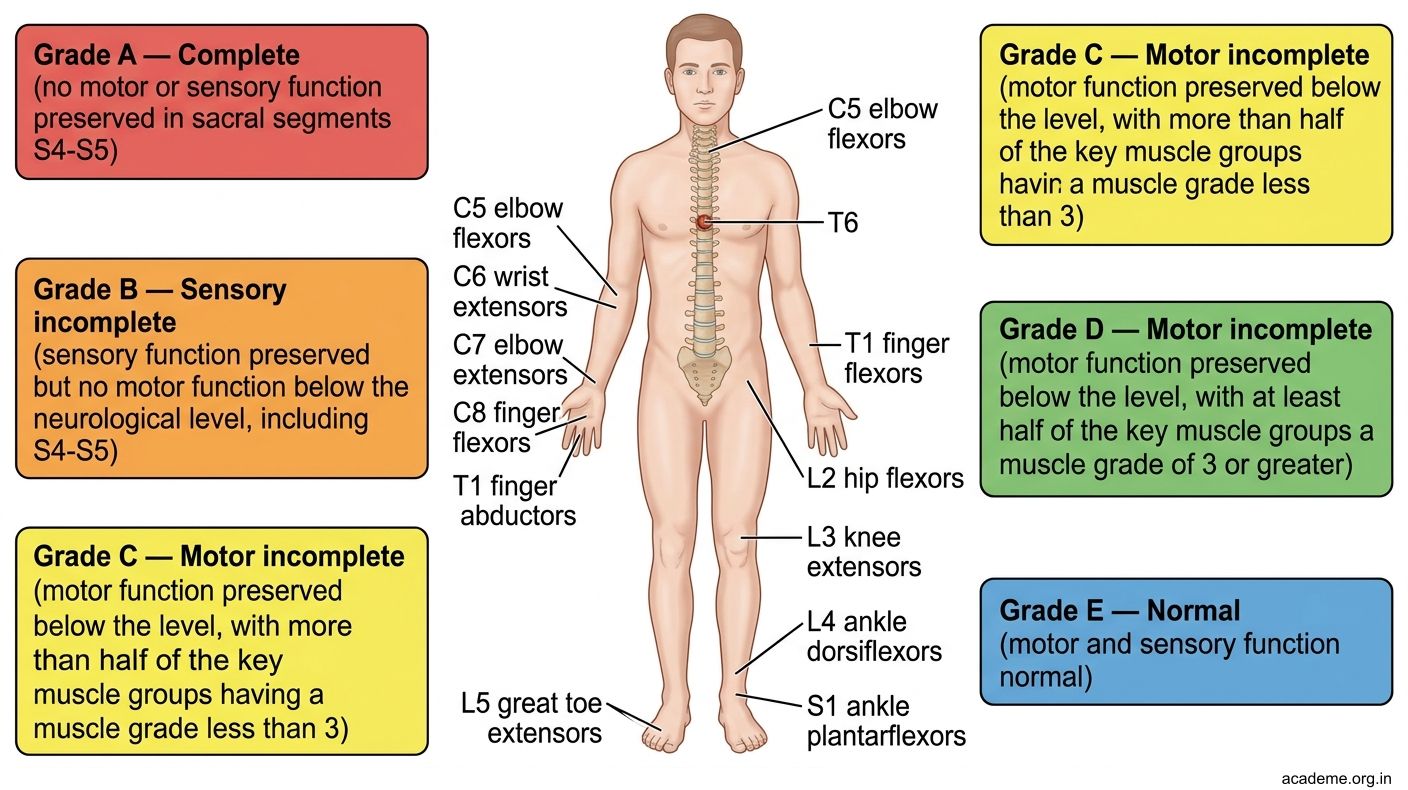
Figure: ASIA Grading (Spinal Cord Injury):
SELF-CHECK — : Spinal Cord Tracts
Fasciculus gracilis carries sensory fibres from the lower limb. At what level does the first-order neuron synapse with the second-order neuron?
A. Dorsal horn at entry level
B. Thalamus (VPL nucleus)
C. Nucleus gracilis in the medulla
D. Anterior commissure
Reveal Answer
Answer: C. Nucleus gracilis in the medulla
The lateral horn is present in the spinal cord only at which levels?
A. All spinal levels
B. T1–L2 (and S2–S4)
C. C1–T1
D. L1–S5
Reveal Answer
Answer: B. T1–L2 (and S2–S4)
A 35-year-old woman develops bilateral loss of pain/temperature over both arms and shoulders in a "cape" distribution. The most likely diagnosis is:
A. Brown-Séquard syndrome
B. Posterior column disease
C. Transverse myelitis
D. Syringomyelia
Reveal Answer
Answer: D. Syringomyelia
CLINICAL PEARL
Spinal Shock vs Neurogenic Shock — Distinction for Indian Emergency Medicine
Spinal Shock:
• Immediate flaccid paralysis + absent reflexes after acute spinal cord injury
• Lasts hours to days → then UMN signs appear (spasticity, hyperreflexia)
• Not cardiovascular — BP can be normal or raised
Neurogenic Shock:
• Loss of sympathetic vasomotor tone after injury at T6 or above
• Bradycardia (loss of cardiac sympathetics T1–T5) + hypotension (vasodilation)
• Treated with atropine (for bradycardia) + vasopressors
ASIA Grading (Spinal Cord Injury):
| Grade | Description |
|---|---|
| A | Complete: no sensory or motor below injury |
| B | Sensory incomplete only |
| C | Motor: >50% key muscles below injury grade <3 |
| D | Motor: >50% key muscles below injury grade ≥3 |
| E | Normal |
Used in every Indian spinal cord injury centre for prognosis.
REFLECT
Return to the three patients in the hook:
- Patient 1 (Brown-Séquard): The lesion is on the RIGHT side at T6. Explain why pain/temperature is lost on the LEFT (not right) below T6.
- Patient 2 (SCD from B12 deficiency): He has spastic paraplegia (UMN) but B12 deficiency also causes peripheral neuropathy. How might this modify his reflexes?
- Patient 3 (Poliomyelitis): Why is there NO sensory loss despite severe motor paralysis? Which specific grey matter structure is destroyed?
Discussion: (1) Spinothalamic fibres cross in the anterior commissure 1–2 segments above entry → right side lesion at T6 blocks fibres that entered from the left below T6 (already crossed). (2) UMN → hyperreflexia, but B12 peripheral neuropathy (affecting afferent arc) may make reflexes absent or diminished — "mixed" picture. (3) Poliovirus selectively destroys anterior horn cells (LMNs) — sensory neurons and pathways are entirely spared.
KEY TAKEAWAYS
Key Takeaways — Spinal Cord
- External features: Cervical + lumbosacral enlargements, conus medullaris (L1–L2 adult, L2–L3 neonate), cauda equina below conus
- Grey matter: Anterior horn (motor LMNs), Posterior horn (sensory), Lateral horn (T1–L2 sympathetic, S2–S4 parasympathetic)
- Posterior columns: Fine touch, vibration, proprioception — IPSILATERAL, cross in medulla
- Spinothalamic: Pain, temperature — cross 1–2 levels up in anterior commissure → ascend CONTRALATERAL
- Corticospinal: Voluntary motor — decussate in medulla, LATERAL column
- Syndromes: Brown-Séquard (hemisection), SCD (B12 — posterior+lateral columns), Polio (anterior horn → LMN only), ALS (UMN+LMN, no sensory), Syringomyelia (central, cape distribution), Transverse myelitis (all tracts)