Page 1 of 4
AN58.1-4 | Medulla Oblongata — SDL Guide
Learning Objectives
- Identify the external features of the medulla oblongata (AN58.1)
- Describe transverse sections at the levels of pyramidal decussation, sensory decussation, and inferior olivary nucleus (AN58.2)
- Describe cranial nerve nuclei in the medulla with their functional groups (AN58.3)
- Describe the anatomical basis of medial and lateral medullary syndromes and crossed diplegia (AN58.4)
INSTRUCTIONS
Master the external surface anatomy first, then work through each cross-section systematically from caudal to rostral. Link each nucleus to a cranial nerve and a clinical syndrome.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
- Snell's Clinical Neuroanatomy, Chapter 6 — Brainstem (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
Two patients in a neurology ward in Chennai:
Patient A (68-year-old man with hypertension): Sudden onset vertigo, vomiting, hoarseness of voice, difficulty swallowing. Examination: ataxia and Horner's syndrome on the RIGHT; loss of pain and temperature over the right face and left arm/leg. Cardiovascular exam: hypertension. MRI diffusion: right lateral medullary infarct.
Patient B (55-year-old diabetic man): Sudden right-sided weakness of the arm and leg with RIGHT-sided tongue deviation on protrusion. Examination: right hemiplegia (spastic), brisk right DTRs, and wasted tongue deviating to the RIGHT. MRI: left medial medullary infarct.
One lesion is medial, one is lateral. How does the anatomy of the medulla explain these completely different syndromes?
WHY THIS MATTERS
Medullary anatomy is clinically critical:
- Wallenberg syndrome (Lateral medullary syndrome) — among the most common brainstem strokes in India; posterior inferior cerebellar artery (PICA) territory
- Medial medullary syndrome (Dejerine syndrome) — anterior spinal artery territory; rarer but classic examination question
- Brainstem strokes — account for ~10% of all strokes; present with "crossed" (ipsilateral face + contralateral body) deficits — a hallmark of brainstem pathology
- Bulbar vs pseudobulbar palsy — distinction based on site of CN IX–XII involvement (LMN vs UMN); essential for Indian neurology practice
- Vital centres — the respiratory and cardiovascular centres in the medulla are life-sustaining; medullary compression (raised ICP) causes Cushing's triad
RECALL
Before we begin, recall:
- The medulla oblongata is the most caudal part of the brainstem, continuous with the spinal cord at the foramen magnum
- It contains vital centres: respiratory, cardiovascular, vomiting (area postrema)
- Cranial nerves IX (glossopharyngeal), X (vagus), XI (accessory), XII (hypoglossal) have nuclei in the medulla
- The medulla is structurally divided into a closed (caudal) part and an open (rostral) part, where the fourth ventricle opens
Part 1: External Features (AN58.1)
Anterior Surface of the Medulla:
• Pyramid — rounded ridge on each side of the anterior median fissure; contains the corticospinal fibres
• Pyramidal decussation — at the caudal end; 85% of corticospinal fibres cross here → visible as an "X" pattern obliterating the anterior median fissure
• Olive — oval eminence lateral to the pyramid; overlies the inferior olivary nucleus
• Rootlets of CN XII (hypoglossal) — emerge between the pyramid and olive (preolivary sulcus)

Figure: Part 1: External Features (AN58.1)
Posterior Surface of the Medulla (lower closed part):
• Posterior median sulcus — continuation of spinal cord
• Gracile tubercle (clava) — overlies nucleus gracilis; medial
• Cuneate tubercle — overlies nucleus cuneatus; lateral
• Obex — small projection at the lower end of the 4th ventricle floor (marking the opening of the central canal)
Posterior Surface (upper open part — floor of 4th ventricle):
• Hypoglossal triangle — overlies CN XII nucleus
• Vagal triangle — overlies dorsal nucleus of vagus
• Vestibular area — lateral to the sulcus limitans (CN VIII vestibular nuclei)
• Stria medullaris — fibres crossing to the cerebellum (arcuate fibres)
• Rootlets of CN IX, X, XI — emerge lateral to the olive (postolivary sulcus)

Figure: Part 1: External Features (AN58.1)
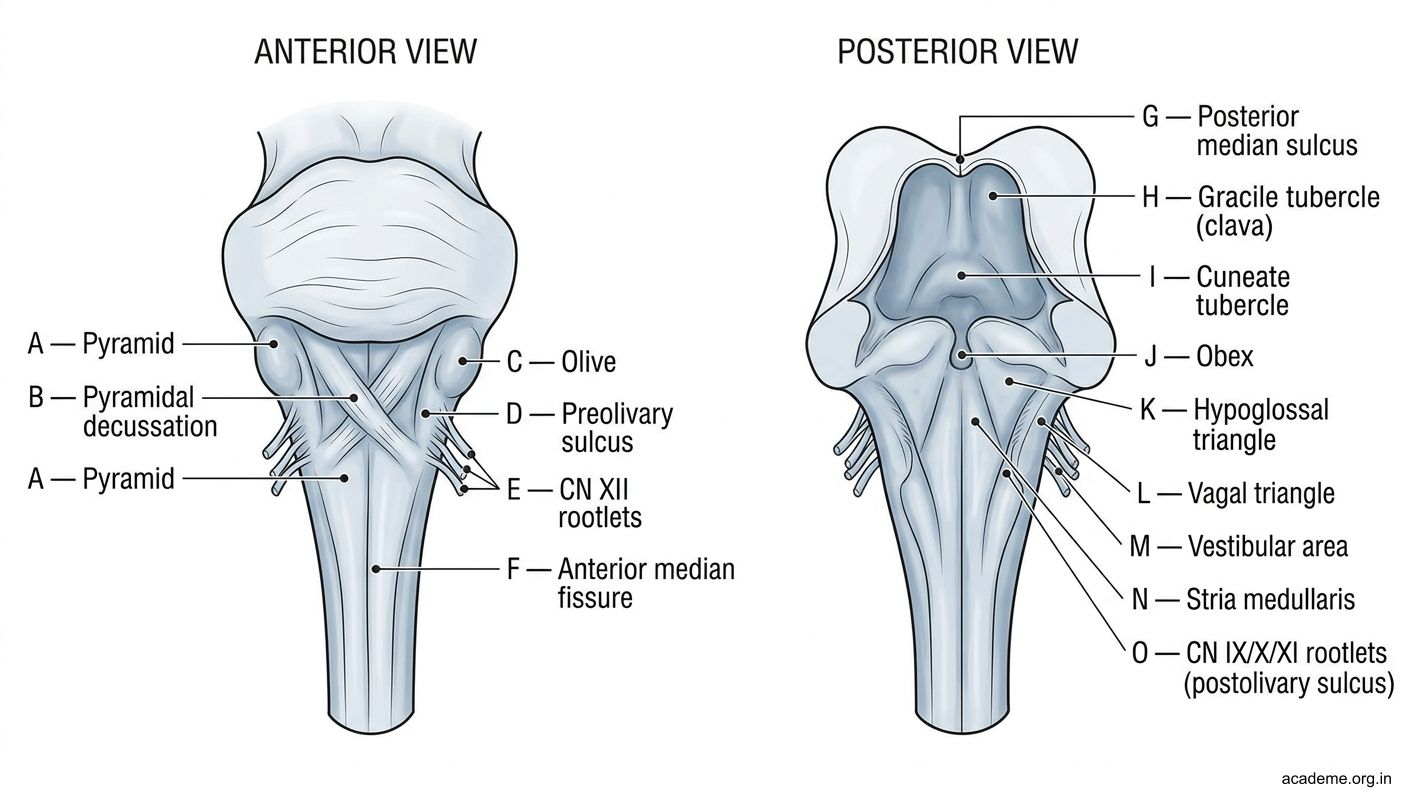
Figure: Part 1: External Features (AN58.1)
Part 2: Transverse Sections of the Medulla (AN58.2)
Section 1: Level of Pyramidal Decussation (most caudal)

Figure: Part 2: Transverse Sections of the Medulla (AN58.2)
This level is CAUDAL to the obex; resembles a spinal cord cross-section.
- Anteriorly: The pyramids (corticospinal fibres) are crossing from right to left and left to right — the "decussation" is visible as fibres interdigitating across the midline
- Posteriorly: Posterior column nuclei are beginning to appear:
- Nucleus gracilis (medial) — nucleus for fasciculus gracilis
- Nucleus cuneatus (lateral) — nucleus for fasciculus cuneatus
- Lateral: The spinal tract of CN V (carrying pain/temperature from the face) and its nucleus
- The central canal is still closed at this level
Section 2: Level of Sensory Decussation (internal arcuate fibres)
Just above the pyramidal decussation.
- Nucleus gracilis and nucleus cuneatus are now prominent (in the posterior part)
- Internal arcuate fibres — axons of 2nd order neurons from nucleus gracilis and cuneatus curve anteromedially and CROSS the midline to form the medial lemniscus on the opposite side
- This is the sensory (internal arcuate) decussation — point where posterior column information crosses
- After crossing, the medial lemniscus lies as a vertical slab in the midline posterior to the pyramid
- Lateral: Spinal nucleus of CN V + spinal tract of CN V
- Central canal — still closed
Section 3: Level of the Inferior Olivary Nucleus (rostral medulla)
The 4th ventricle has opened at this level.
Ventral (anterior) structures:
• Pyramid — contains corticospinal (15–20% uncrossed, some crossed)
• Medial lemniscus — ribbon-shaped, now lying vertically just dorsal to the pyramid
• Inferior olivary nucleus — wrinkled, bag-shaped (on cross-section = crenated outline); a relay for the cerebellum; forms the olive surface feature
Dorsal (posterior) structures (floor of 4th ventricle):
• Hypoglossal nucleus (CN XII) — most medial, near midline
• Dorsal nucleus of vagus (CN X) — lateral to CN XII nucleus; parasympathetic
• Nucleus of tractus solitarius — lateral; receives visceral sensation (taste for VII, IX, X; visceral sensation for X)
• Vestibular nuclei — in the lateral floor of the 4th ventricle (medial and inferior vestibular nuclei here)
Lateral structures:
• Nucleus ambiguus — in the lateral reticular formation; motor for CN IX, X, XI (branchiomotor); important for swallowing and phonation
• Spinal nucleus of CN V — continues from cord; pain/temperature from face
• Inferior cerebellar peduncle — connects medulla to cerebellum; contains spinocerebellar, olivocerebellar, vestibulocerebellar fibres
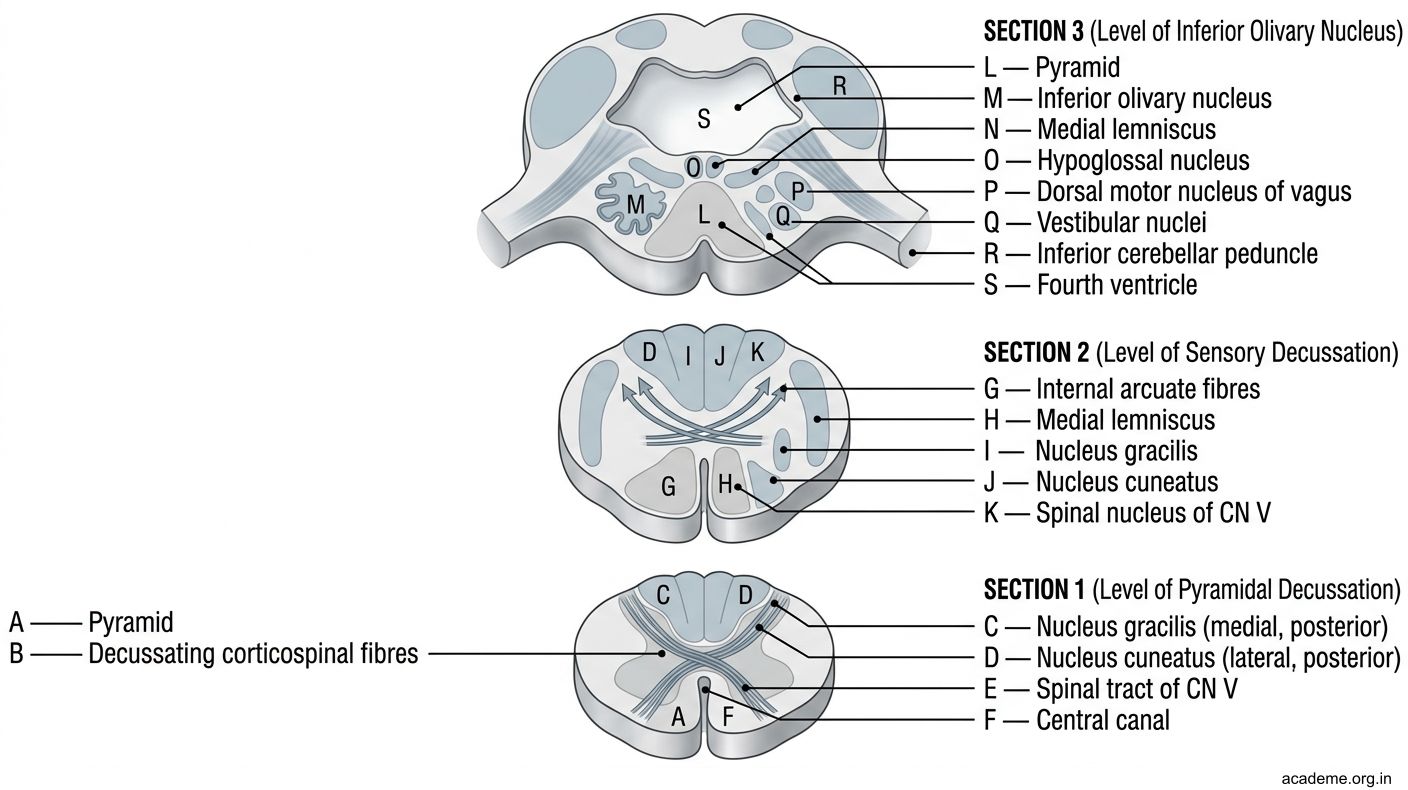
Figure: Part 2: Transverse Sections of the Medulla (AN58.2)

Figure: Section 2: Level of Sensory Decussation (internal arcuate fibres)

Figure: Section 3: Level of the Inferior Olivary Nucleus (rostral medulla)
Part 3: Cranial Nerve Nuclei in the Medulla (AN58.3)
CN IX — Glossopharyngeal
| Component | Nucleus | Function |
|---|---|---|
| GSA (somatic sensory) | Spinal nucleus of CN V | Skin of ear |
| GVA (visceral sensory) | Nucleus tractus solitarius (NTS) | Carotid sinus/body sensation |
| SVA (special visceral — taste) | NTS (gustatory nucleus, upper) | Taste from posterior 1/3 tongue |
| SVE (branchiomotor) | Nucleus ambiguus | Stylopharyngeus muscle |
| GVE (parasympathetic) | Inferior salivatory nucleus | Parotid gland |
CN X — Vagus
| Component | Nucleus | Function |
|---|---|---|
| GSA | Spinal nucleus of CN V | Skin of ear (Arnold's nerve) |
| GVA | Nucleus tractus solitarius | Thoracic and abdominal viscera |
| SVA | NTS (gustatory nucleus) | Taste from epiglottis |
| SVE | Nucleus ambiguus | Pharyngeal and laryngeal muscles |
| GVE | Dorsal nucleus of vagus | Thoracoabdominal parasympathetics |
CN XI — Accessory
| Component | Nucleus | Function |
|---|---|---|
| Cranial root | Nucleus ambiguus | Pharyngeal/laryngeal (joins vagus) |
| Spinal root | C1–C5 anterior horn | Sternocleidomastoid + trapezius |
CN XII — Hypoglossal
| Component | Nucleus | Function |
|---|---|---|
| GSE (somatic motor) | Hypoglossal nucleus | All intrinsic + most extrinsic tongue muscles |

Figure: Part 3: Cranial Nerve Nuclei in the Medulla (AN58.3)

Figure: CN XI — Accessory
Part 4: Medullary Syndromes (AN58.4)
Lateral Medullary Syndrome (Wallenberg Syndrome)
• Cause: Occlusion of posterior inferior cerebellar artery (PICA) or vertebral artery → infarct of lateral medulla
• Structures affected:
- Nucleus ambiguus (CN IX, X) → ipsilateral dysphagia, hoarseness (LMN palsy of pharynx/larynx)
- Vestibular nuclei → ipsilateral vertigo, nausea, vomiting, nystagmus
- Spinal nucleus and tract of CN V → ipsilateral facial pain/temperature loss
- Spinothalamic tract → contralateral body pain/temperature loss
- Sympathetic fibres (descending) → ipsilateral Horner's syndrome (ptosis, miosis, anhidrosis)
- Inferior cerebellar peduncle / spinocerebellar tracts → ipsilateral limb ataxia
• Summary: "DOVES" mnemonic — Dysphagia, vertigo, ipsilateral (Ocular Horner, vestibular), contralateral spinothalamic Sensation loss
| Sign | Side | Structure |
|---|---|---|
| Dysphagia, hoarseness | Ipsilateral | Nucleus ambiguus |
| Horner's syndrome | Ipsilateral | Descending sympathetics |
| Facial pain/temp loss | Ipsilateral | Spinal nucleus CN V |
| Body pain/temp loss | Contralateral | Spinothalamic tract |
| Ataxia | Ipsilateral | Inf. cerebellar peduncle |
| Vertigo, nystagmus | Ipsilateral | Vestibular nuclei |
Patient A in the hook = RIGHT lateral medullary infarct
Medial Medullary Syndrome (Dejerine Syndrome)
• Cause: Occlusion of anterior spinal artery (anterior medullary artery) → infarct of medial medulla
• Structures affected:
- Pyramid (corticospinal) → contralateral hemiplegia (arm + leg, face spared)
- Medial lemniscus → contralateral loss of fine touch, vibration, proprioception
- CN XII rootlets or nucleus → ipsilateral tongue paralysis (LMN) — tongue deviates TOWARD the side of lesion
• The "crossed hemiplegia" (contralateral body + ipsilateral CN XII) is classic
| Sign | Side | Structure |
|---|---|---|
| Hemiplegia (arm + leg) | Contralateral | Pyramid |
| Loss of fine touch/vibrn/prop | Contralateral | Medial lemniscus |
| Tongue deviation (LMN) | Ipsilateral | CN XII nucleus/rootlets |
Patient B in the hook = LEFT medial medullary infarct → right hemiplegia + right tongue deviation (LMN)
Crossed Diplegia (Diplegia of the Cross)
• Bilateral medullary involvement
• Quadriplegia + bilateral LMN cranial nerve palsies
• Rare; caused by bilateral medullary infarcts or basilar artery occlusion

Figure: Part 4: Medullary Syndromes (AN58.4)

Figure: Bulbar Palsy vs Pseudobulbar Palsy — India Clinic Essential

Figure: Key Takeaways — Medulla Oblongata
SELF-CHECK — : Medulla
At the level of sensory decussation in the medulla, which fibres are crossing the midline?
A. Corticospinal (pyramidal) fibres
B. Internal arcuate fibres (2nd order neurons from nucleus gracilis and cuneatus)
C. Spinothalamic fibres
D. Trigeminothalamic fibres
Reveal Answer
Answer: B. Internal arcuate fibres (2nd order neurons from nucleus gracilis and cuneatus)
The nucleus ambiguus in the medulla provides motor innervation to:
A. Intrinsic muscles of the tongue
B. Muscles of mastication
C. Muscles of the pharynx and larynx (via CN IX, X, XI)
D. Muscles of facial expression
Reveal Answer
Answer: C. Muscles of the pharynx and larynx (via CN IX, X, XI)
In Wallenberg syndrome, contralateral loss of pain and temperature in the body occurs because which structure is damaged?
A. Nucleus ambiguus
B. Spinal nucleus of CN V
C. Medial lemniscus
D. Spinothalamic tract (in the lateral medulla)
Reveal Answer
Answer: D. Spinothalamic tract (in the lateral medulla)
CLINICAL PEARL
Bulbar Palsy vs Pseudobulbar Palsy — India Clinic Essential
| Feature | Bulbar Palsy (LMN) | Pseudobulbar Palsy (UMN) |
|---|---|---|
| Site of lesion | Motor nuclei of CN IX–XII (in medulla) | Bilateral corticobulbar tracts (above medulla) |
| Tongue | Wasted, fasciculating | Small, spastic, no fasciculations |
| Palate | Paralysed, absent gag | Spastic |
| Speech | Nasal, dysarthric | "Hot potato" speech, dysarthric |
| Jaw jerk | Absent | Brisk |
| Emotional lability | No | Yes (pathological laughing/crying) |
| Causes in India | ALS (MND), GBS, polio, diphtheria | Bilateral MCA strokes, MND (mixed) |
Vital centres in the medulla:
• Respiratory centres (dorsal = inspiratory; ventral = expiratory + pneumotaxic in pons)
• Cardiovascular centre (vasomotor + cardiac)
• Vomiting centre (area postrema — outside BBB, responds to emetic drugs)
• Compression of medulla by raised ICP → Cushing's triad (hypertension + bradycardia + irregular breathing) = sign of impending herniation
REFLECT
Return to the two patients in the hook:
- Patient A (right lateral medullary infarct): Why is facial pain/temperature loss on the RIGHT side, while body pain/temperature loss is on the LEFT?
- Patient B (left medial medullary infarct): Why does the tongue deviate to the RIGHT? Is this UMN or LMN tongue palsy?
- In Patient A, hoarseness occurs — which nucleus is damaged and what does it innervate?
- In Wallenberg syndrome, why is there NO limb weakness despite being a stroke?
Discussion: (1) Right lateral lesion damages right spinal nucleus of CN V (face ipsilateral) and right spinothalamic tract (carrying left body pain fibres that already crossed in cord). (2) Left CN XII nucleus = LMN; tongue deviates TOWARD lesion = to the right. (3) Nucleus ambiguus → pharyngeal and laryngeal muscles via CN X. (4) The pyramids (corticospinal) lie MEDIALLY; lateral medullary infarct spares them → no limb weakness.
KEY TAKEAWAYS
Key Takeaways — Medulla Oblongata
- External features: Pyramid (anterior) + Olive (lateral) + Rootlets XII (between pyramid and olive), IX/X/XI (lateral to olive)
- Sections caudal→rostral: (1) Pyramidal decussation (corticospinal cross), (2) Sensory decussation (internal arcuate fibres cross → medial lemniscus formed), (3) Inferior olivary nucleus level (open medulla, 4th ventricle floor)
- Nuclei: XII (hypoglossal motor), Dorsal nucleus of vagus (parasympathetic), NTS (taste + visceral sensory), Nucleus ambiguus (pharynx/larynx motor — CN IX/X/XI), Vestibular nuclei, Spinal nucleus CN V
- Lateral medullary (Wallenberg): PICA territory; ipsilateral Horner + ataxia + facial pain/temp loss + dysphasia; contralateral body pain/temp loss
- Medial medullary (Dejerine): Anterior spinal artery; contralateral hemiplegia + touch/vibrn loss; ipsilateral LMN tongue palsy