Page 1 of 4
AN60.1-3 | Cerebellum — SDL Guide
Learning Objectives
- Describe and demonstrate the external and internal features of the cerebellum (AN60.1)
- Describe the connections of the cerebellar cortex and intracerebellar nuclei (AN60.2)
- Describe the anatomical basis of cerebellar dysfunction (AN60.3)
INSTRUCTIONS
Understand the functional zones of the cerebellum (spinocerebellum, pontocerebellum, vestibulocerebellum) and map the intracerebellar nuclei to each zone. Clinical signs of cerebellar disease are direct translations of these connections.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
- Snell's Clinical Neuroanatomy — Cerebellum (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 7-year-old boy from Madurai is brought with a 3-week history of headache, vomiting (worse in the morning), unsteady gait, and difficulty holding objects. He falls to both sides when walking. Examination: nystagmus, intention tremor in both hands, dysdiadochokinesia, hypotonia, ataxic (wide-based) gait. MRI brain shows a midline posterior fossa mass in the 4th ventricle with hydrocephalus.
Diagnosis: Medulloblastoma.
Why does a midline cerebellar tumour cause these specific deficits? Why is gait affected more than limb coordination when the midline (vermis) is involved?
WHY THIS MATTERS
Cerebellar anatomy is clinically essential:
- Medulloblastoma — most common malignant brain tumour in children in India; arises in the cerebellar vermis; causes hydrocephalus by blocking the 4th ventricle
- Cerebellar ataxia — a common presentation in Indian neurology: causes include alcohol (India's second most common cause of cerebellar syndrome), vitamin B1 deficiency, paraneoplastic, MS, strokes
- Posterior fossa surgery — cerebellar tumours require knowledge of the peduncles, vermis, and tonsillar herniation
- Chiari malformation — cerebellar tonsillar herniation through foramen magnum; causes syringomyelia (discussed in spinal cord module)
RECALL
Before we begin, recall:
- The cerebellum occupies the posterior fossa, below the tentorium cerebelli
- It connects to the brainstem via three pairs of cerebellar peduncles
- Functionally: coordinates movement, maintains posture, and regulates muscle tone
- It does NOT initiate movements; it modulates them
Part 1: External and Internal Features (AN60.1)
External Features

Figure: Part 1: External and Internal Features (AN60.1)
- Two hemispheres + central vermis (worm-shaped midline strip)
- Folia — transversely oriented ridges on the cerebellar surface (equivalent to gyri)
- Fissures separate lobes:
- Primary fissure — separates anterior lobe from posterior lobe
- Posterolateral fissure — separates flocculonodular lobe from the posterior lobe
Three Lobes:
| Lobe | Location | Functional Zone |
|---|---|---|
| Anterior lobe | Above primary fissure | Spinocerebellum (muscle tone, posture) |
| Posterior lobe (largest) | Between primary + posterolateral fissures | Pontocerebellum (skilled movements) |
| Flocculonodular lobe | Below posterolateral fissure | Vestibulocerebellum (balance, eye movements) |
Three Functional Zones (phylogenetic):
| Zone | Region | Input | Function | Deep Nucleus |
|---|---|---|---|---|
| Vestibulocerebellum (archicerebellum) | Flocculonodular lobe | Vestibular nuclei | Balance, VOR, eye movements | No deep nucleus (→ vestibular nuclei directly) |
| Spinocerebellum (paleocerebellum) | Anterior lobe + vermis of posterior lobe | Spinal cord (spinocerebellar tracts) | Posture, gait, muscle tone | Fastigial (medial vermis), Interposed (intermediate) |
| Pontocerebellum (neocerebellum) | Lateral hemispheres | Cerebral cortex via pons | Skilled fine voluntary movements | Dentate nucleus |
Internal Structure:
• Surface: 3-layered cerebellar cortex (molecular, Purkinje, granular layers)
• Deep white matter (arbor vitae — "tree of life" on sagittal section)
• Intracerebellar nuclei (medial → lateral): Fastigial, Globosus, Emboliformis, Dentate
- Mnemonic: "Feel Good Every Day" (Fastigial, Globosus, Emboliformis, Dentate)
- Dentate = largest; output for voluntary fine movement (via superior cerebellar peduncle)
- Fastigial = balance, posture
- Globosus + Emboliformis = together called the Interposed nuclei
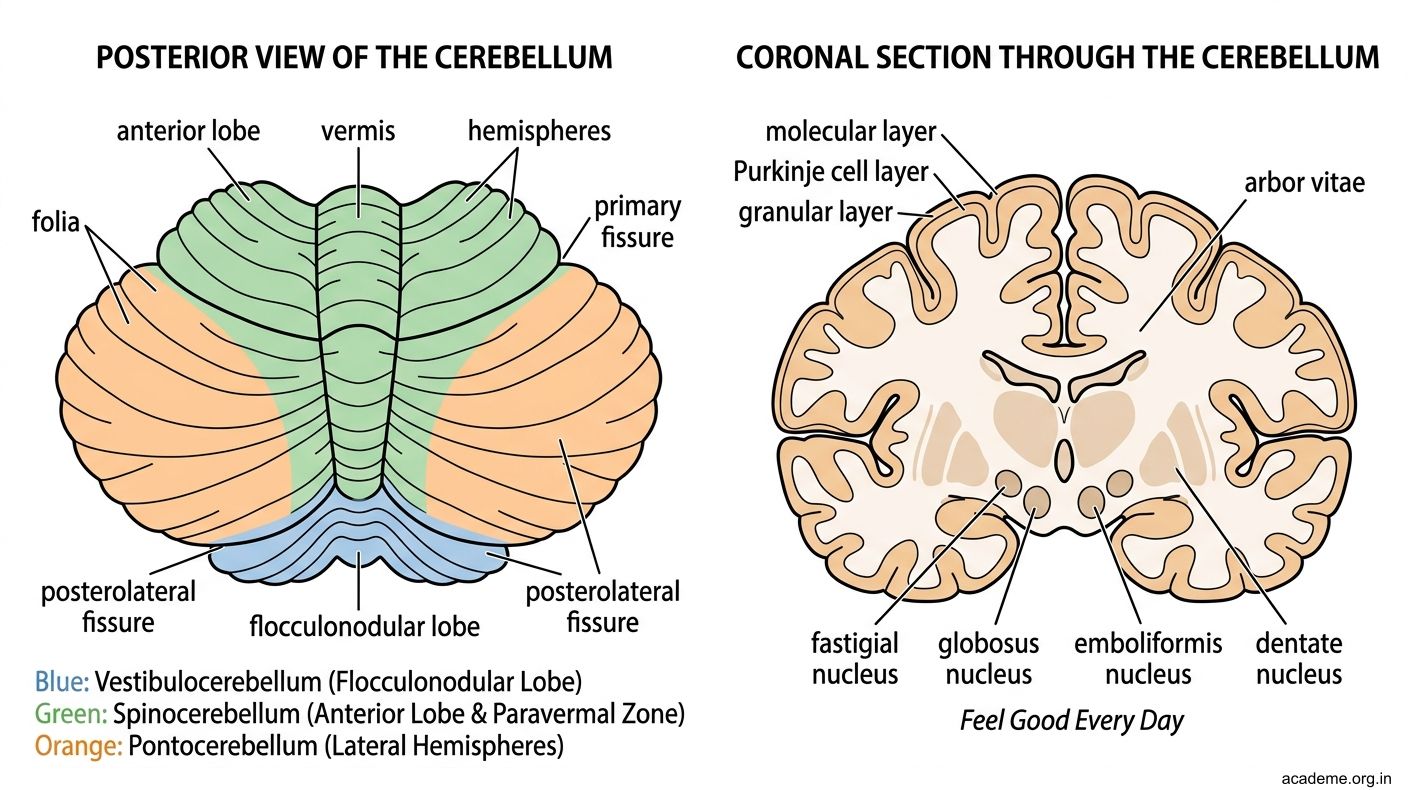
Figure: Part 1: External and Internal Features (AN60.1)

Figure: Three Functional Zones (phylogenetic):
Part 2: Connections of the Cerebellum (AN60.2)
Three Cerebellar Peduncles — Input and Output Pathways

Figure: Part 2: Connections of the Cerebellum (AN60.2)
Inferior Cerebellar Peduncle (Restiform body + Juxtarestiform body)
Inputs (afferents):
• Posterior spinocerebellar tract (from Clarke's column, proprioception)
• Cuneocerebellar tract (upper limb proprioception)
• Vestibulocerebellar fibres (balance input from CN VIII)
• Olivocerebellar fibres (from inferior olivary nucleus — error signals)
Output (efferents):
• Cerebellovestibular fibres (fastigial nucleus → vestibular nuclei)
Middle Cerebellar Peduncle (Brachium pontis) — INPUT ONLY
• Corticopontocerebellar: cerebral cortex → pontine nuclei → cross → middle cerebellar peduncle → cerebellar hemisphere
• This is the largest peduncle; carries cerebrocerebellar information for skilled movements
Superior Cerebellar Peduncle (Brachium conjunctivum) — MAINLY OUTPUT
Output (efferents):
• Dentatorubrothalamic tract: Dentate nucleus → crosses in the midbrain → red nucleus → VL thalamus → motor cortex
• This is the main cerebellar OUTPUT pathway; it decussates in the midbrain tegmentum
Input (afferents):
• Anterior spinocerebellar tract
Cerebellar Cortex Circuitry:
• Purkinje cells — the only OUTPUT neurons of the cerebellar cortex; INHIBITORY (GABA-ergic) → inhibit intracerebellar nuclei
• Climbing fibres (from inferior olivary nucleus) — 1:1 synapse with Purkinje cells; carry error signals; cause long-term depression (LTD) of parallel fibre-Purkinje synapses
• Mossy fibres (all other inputs) → granule cells → parallel fibres → multiple Purkinje cells
• Granule cells — EXCITATORY; the most numerous neurons in the CNS
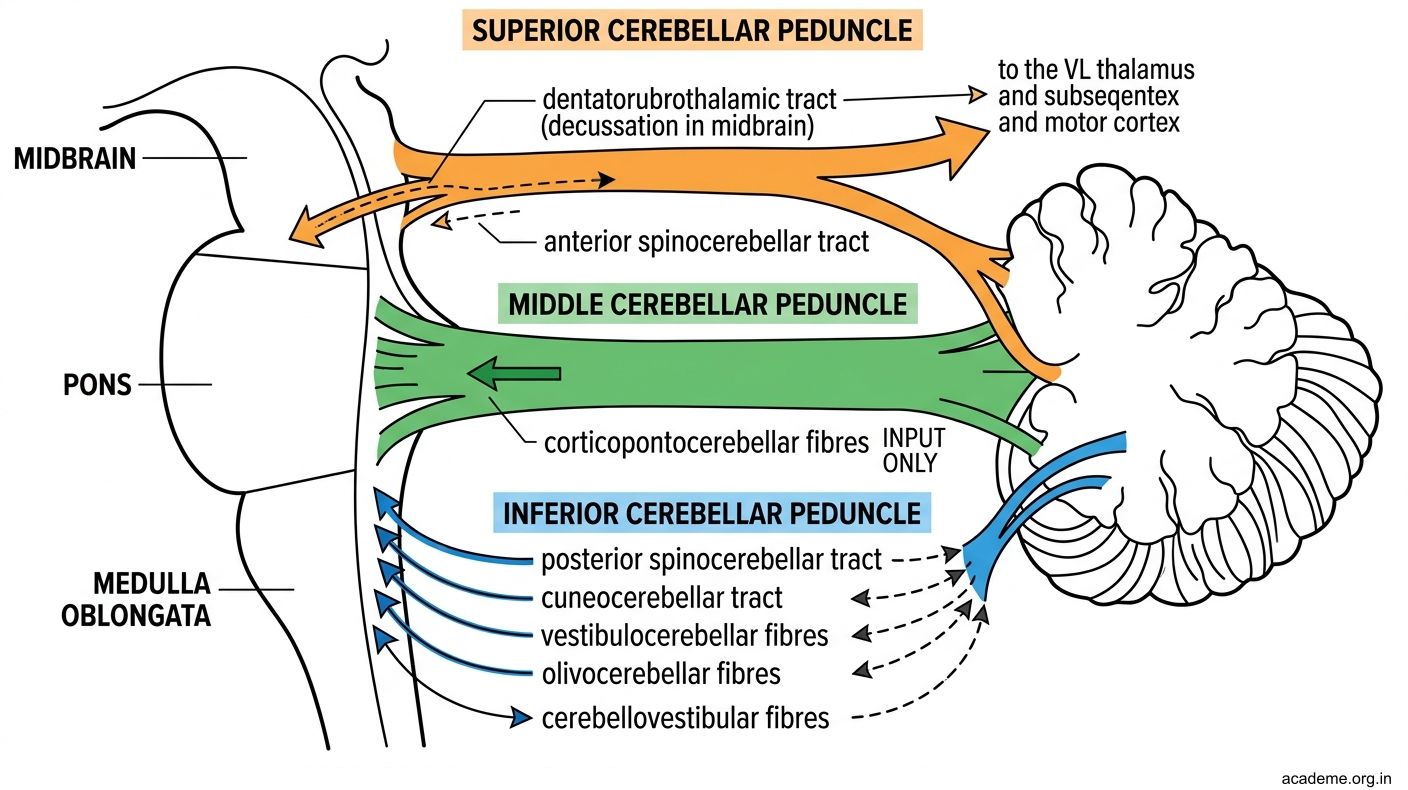
Figure: Part 2: Connections of the Cerebellum (AN60.2)
Part 3: Cerebellar Dysfunction (AN60.3)
Cardinal Signs of Cerebellar Dysfunction — "DANISH"
• Dysdiadochokinesia — inability to perform rapid alternating movements
• Ataxia (gait) — wide-based, staggering gait; falls TOWARD the side of lesion
• Nystagmus — fast phase TOWARD side of lesion (opposite to peripheral nystagmus)
• Intention tremor — tremor that worsens on approaching target (vs resting tremor = Parkinson's)
• Speech — dysarthria (scanning/staccato speech)
• Hypotonia — decreased muscle tone; pendular reflexes
Additional signs:
• Past pointing (dysmetria) — inability to accurately point to a target
• Rebound phenomenon — loss of check reflex; limb overshoots when resistance released
• Titubation — rhythmic oscillation of the trunk or head
Localising Value of Cerebellar Signs:
| Structure | Signs | Example Disease |
|---|---|---|
| Vermis (spinocerebellum) | Truncal ataxia, wide-based gait, titubation | Medulloblastoma (children), alcoholic cerebellar degeneration |
| Hemispheres (pontocerebellum) | Ipsilateral limb ataxia, intention tremor, dysdiadochokinesia | PICA stroke, tumour |
| Flocculonodular lobe (vestibulocerebellum) | Gait ataxia, nystagmus, balance disturbance | Midline posterior fossa tumours |
Why ipsilateral signs?
• Cerebellum controls IPSILATERAL limbs (unlike cerebral cortex which is contralateral)
• Double-crossing pathway: cerebellum → superior cerebellar peduncle → crosses to contralateral red nucleus/thalamus → motor cortex → crosses again in corticospinal tract → back to ipsilateral limb
Common causes in India:
• Alcoholic cerebellar degeneration — selective vermis degeneration (anterior lobe); gait ataxia predominates, arm ataxia minimal
• Medulloblastoma — children; midline; vermis → gait ataxia + hydrocephalus
• PICA territory infarct — lateral medullary + ipsilateral cerebellar hemisphere
• Paraneoplastic cerebellar degeneration — lung, breast, ovarian cancer in adults

Figure: Part 3: Cerebellar Dysfunction (AN60.3)

Figure: Localising Value of Cerebellar Signs:

Figure: Differentiating Cerebellar Ataxia from Sensory Ataxia (Posterior Column)

Figure: Key Takeaways — Cerebellum
SELF-CHECK — : Cerebellum
The ONLY output neurons of the cerebellar cortex are:
A. Granule cells
B. Purkinje cells
C. Basket cells
D. Golgi cells
Reveal Answer
Answer: B. Purkinje cells
The dentate nucleus output travels through which cerebellar peduncle?
A. Inferior cerebellar peduncle
B. Middle cerebellar peduncle
C. Superior cerebellar peduncle
D. Both superior and inferior peduncles equally
Reveal Answer
Answer: C. Superior cerebellar peduncle
A 60-year-old alcoholic presents with wide-based gait ataxia but relatively preserved arm coordination. This pattern suggests preferential degeneration of the:
A. Cerebellar vermis (anterior lobe)
B. Dentate nucleus
C. Cerebellar hemispheres bilaterally
D. Flocculonodular lobe
Reveal Answer
Answer: A. Cerebellar vermis (anterior lobe)
CLINICAL PEARL
Differentiating Cerebellar Ataxia from Sensory Ataxia (Posterior Column)
| Feature | Cerebellar Ataxia | Sensory Ataxia (Post. Column) |
|---|---|---|
| Romberg test | Negative (falls even with eyes open) | Positive (sways/falls when eyes closed) |
| Gait | Wide-based, staggering, cannot correct | Wide-based, "stamping" gait, improves with visual feedback |
| Nystagmus | Present | Absent |
| Intention tremor | Present | Absent |
| Reflexes | Pendular (hypotonia) | Absent (posterior column + peripheral neuropathy) |
| Sensation | Normal | Vibration + proprioception lost |
Romberg test: Patient stands with feet together, arms at sides. Eyes open first. Then close eyes. POSITIVE = sways with eyes closed (sensory ataxia — relies on vision to compensate for lost proprioception). Cerebellar ataxia: cannot stand steadily EVEN with eyes open → Romberg not informative.
REFLECT
Return to the hook case — the 7-year-old with medulloblastoma:
- Why does a midline vermis tumour cause truncal ataxia and wide-based gait rather than limb coordination problems?
- The child has nystagmus. Which part of the cerebellum controls eye movements and balance?
- Why does medulloblastoma in the 4th ventricle cause hydrocephalus? Trace the CSF pathway to identify the blockage.
- He has morning vomiting and headache — explain anatomically why morning is worse.
Discussion: (1) Vermis = spinocerebellum (gait, posture); hemispheres = limb coordination. (2) Flocculonodular lobe (vestibulocerebellum). (3) Tumour blocks CSF outflow through foramina of Magendie/Luschka from 4th ventricle → obstructive hydrocephalus. (4) ICP is highest in the morning after lying flat all night (CO2 accumulation + increased intracranial venous pressure in recumbency → worsens cerebral oedema) → morning headache and vomiting.
KEY TAKEAWAYS
Key Takeaways — Cerebellum
- Three lobes: Anterior (spinocerebellum, posture), Posterior (pontocerebellum, skilled movements), Flocculonodular (vestibulocerebellum, balance)
- Deep nuclei (medial→lateral): Fastigial, Globosus, Emboliformis, Dentate (mnemonic: FGED)
- Peduncles: Inferior = input (spinocerebellar, olivocerebellar, vestibular). Middle = input only (corticopontocerebellar). Superior = MAIN OUTPUT (dentatorubrothalamic, crosses in midbrain)
- Purkinje cells = only cortical output, INHIBITORY (GABA)
- Ipsilateral control of limbs (double crossing)
- DANISH signs: Dysdiadochokinesia, Ataxia, Nystagmus, Intention tremor, Speech (dysarthria), Hypotonia
- Vermis lesion → truncal/gait ataxia. Hemisphere lesion → ipsilateral limb ataxia