Page 1 of 4
AN63.1-3 | Ventricular System & Special sensory pathways — SDL Guide
Learning Objectives
- Describe and demonstrate the parts, boundaries, and features of the 3rd, 4th, and lateral ventricles (AN63.1)
- Describe the anatomical basis of congenital hydrocephalus (AN63.2)
- Describe the olfactory, visual, auditory, and gustatory pathways (AN63.3)
INSTRUCTIONS
The visual pathway is the highest yield topic in this module — master the field defects for each lesion level. The ventricular system must be known anatomically for procedural localisation (shunt placement, neuroendoscopy).
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
Two patients in a neuro-ophthalmology clinic in Chennai:
Patient A (35-year-old woman): Gradually progressive loss of vision. Examination: she cannot see objects in the temporal field of BOTH eyes when tested separately. She walks into objects on her sides. Visual acuity is normal centrally.
Patient B (65-year-old man with hypertension): Sudden loss of vision in the right half of the visual field of BOTH eyes. He can read with the left half of his vision. MRI shows left occipital cortex infarct.
Two patients with bilateral visual field defects from lesions at different levels of the visual pathway. Can you explain both patterns from the anatomy of the optic chiasm and optic radiations?
WHY THIS MATTERS
- Visual field defects — tested in every clinical examination; bitemporal hemianopia = pituitary tumour; homonymous hemianopia = occipital/radiation lesion
- Hydrocephalus — VP shunting is one of the most common paediatric neurosurgical procedures in India
- Olfactory pathway — anosmia from COVID-19 (India had massive pandemic impact) + olfactory groove meningioma
- Auditory pathway — sensorineural vs conductive hearing loss distinction; acoustic neuroma
RECALL
Before we begin:
• CSF is produced in the choroid plexus of the ventricles and circulates through the ventricular system → subarachnoid space → arachnoid granulations → venous sinuses
• The visual pathway uses the optic chiasm where nasal fibres cross and temporal fibres remain ipsilateral
• Special senses = olfaction, vision, hearing, taste, balance
Part 1: Ventricular System (AN63.1)
Lateral Ventricles (2, one in each hemisphere)
• C-shaped cavity following the hemisphere
• Parts: anterior horn (frontal lobe), body (parietal), posterior horn (occipital), inferior horn (temporal)
• Choroid plexus: in body and inferior horn (most CSF production)
• Communicate with 3rd ventricle via foramen of Monro (interventricular foramen)

Figure: Part 1: Ventricular System (AN63.1)
3rd Ventricle (1, midline)
• Narrow slit between the two thalami (thalami form the lateral walls)
• Floor: hypothalamus
• Roof: choroid plexus of 3rd ventricle, fornix
• Features on the wall: hypothalamic sulcus, supraoptic recess, infundibular recess, pineal recess, suprapineal recess
• Connects to 4th ventricle via cerebral aqueduct of Sylvius (through midbrain)
4th Ventricle (1, posterior fossa)
• Between pons/medulla (anterior) and cerebellum (posterior)
• Diamond-shaped floor (rhomboid fossa) — forms the posterior surface of the pons and open medulla
• Roof: superior medullary velum + inferior medullary velum + part of cerebellum
• Three openings (exits for CSF into subarachnoid space):
- Foramen of Magendie (median aperture) — midline, into cisterna magna
- Foramina of Luschka (lateral apertures, ×2) — into the pontine cistern lateral recess
• Continues inferiorly as the central canal of the spinal cord (narrows at obex)
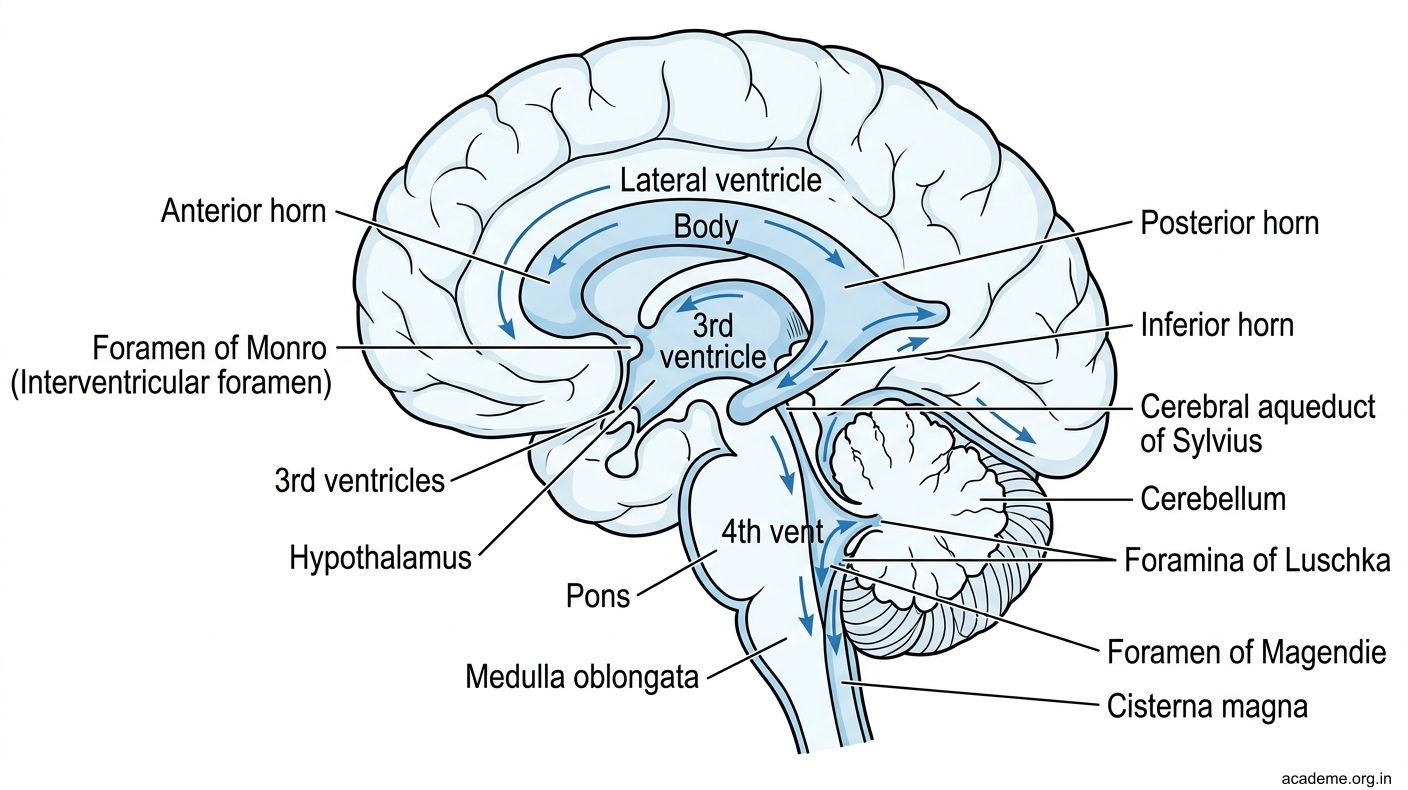
Figure: Part 1: Ventricular System (AN63.1)
Part 2: Congenital Hydrocephalus (AN63.2)
Definition: Abnormal accumulation of CSF causing ventricular dilation and raised ICP
Types relevant to congenital causes:
| Type | Mechanism | Congenital Cause |
|---|---|---|
| Obstructive (non-communicating) | CSF blocked within the ventricular system | Aqueductal stenosis (X-linked HSAS syndrome, CRASH syndrome), Dandy-Walker malformation |
| Communicating | CSF not absorbed (free flow from ventricles to subarachnoid) | Chiari malformation (foraminal block), post-meningitic scarring of arachnoid villi |
Aqueductal Stenosis (most common congenital obstructive hydrocephalus):
• Aqueduct of Sylvius is stenosed → CSF cannot flow from 3rd to 4th ventricle → lateral + 3rd ventricles dilate; 4th ventricle NORMAL
• In neonates: head enlarges before suture fusion → macrocephaly, "setting sun" sign (eyes deviate down as ICP pushes on superior colliculi)
• In older children: ICP signs (headache, vomiting, papilloedema)
Dandy-Walker Malformation:
• Failure of foramina of Magendie and Luschka to open → cystic dilation of 4th ventricle; cerebellar vermis agenesis; high tentorium
• ALL four ventricles dilate (obstructive at the level of the 4th ventricle foramina)
• Associated with corpus callosum agenesis
Chiari Malformation Type I:
• Cerebellar tonsillar descent >5 mm below the foramen magnum → blocks CSF circulation at the foramen magnum level
• Can cause communicating hydrocephalus + syringomyelia
• Common in India: presents with occipital headache (worsens on coughing/straining), myelopathy
Treatment — VP shunt vs ETV:
• VP shunt (ventriculoperitoneal shunt) — most common treatment; tubing from lateral ventricle → peritoneal cavity; relies on valve; needs revision in growing children
• ETV (endoscopic third ventriculostomy) — neuroendoscopic procedure; creates a fenestration in the floor of the 3rd ventricle → direct CSF drainage into subarachnoid space; preferred for aqueductal stenosis in older children (no implanted hardware)

Figure: Part 2: Congenital Hydrocephalus (AN63.2)

Figure: Types relevant to congenital causes:
Part 3: Special Sensory Pathways (AN63.3)
Visual Pathway — THE HIGHEST YIELD TOPIC

Figure: Part 3: Special Sensory Pathways (AN63.3)
Retina → Optic nerve → Optic chiasm → Optic tract → Lateral geniculate body (LGN, thalamus) → Optic radiations → Primary visual cortex (area 17, calcarine sulcus, occipital lobe)
Key anatomical points:
• At the optic chiasm: NASAL retinal fibres (from temporal visual field) cross; TEMPORAL retinal fibres remain ipsilateral
• The visual field is INVERTED and REVERSED in the retina: left visual field → right retinal halves (nasal of left + temporal of right)
• LGN (metathalamus): relay for visual fibres; receives from optic tract
• Optic radiations: from LGN → through internal capsule (retrolenticular part) → to visual cortex
- Upper fibres: go directly posteriorly
- Lower fibres: Meyer's loop — sweep anteriorly into temporal lobe then posteriorly → supply inferior visual field
Visual Field Defects by Lesion Level:
| Level | Lesion | Visual Field Defect |
|---|---|---|
| Optic nerve (one side) | Optic neuritis (MS), trauma | Monocular blindness (one eye only) |
| Optic chiasm (central) | Pituitary tumour | Bitemporal hemianopia (temporal fields of both eyes — nasal fibres that cross are cut) |
| Optic tract | Craniopharyngioma, infarct | Contralateral homonymous hemianopia |
| Meyer's loop (temporal lobe) | Temporal lobe tumour/resection | Contralateral SUPERIOR quadrantanopia ("pie in the sky") |
| Parietal optic radiation | Parietal lobe lesion | Contralateral INFERIOR quadrantanopia |
| Occipital cortex (area 17) | MCA/PCA infarct | Contralateral homonymous hemianopia (MACULAR SPARING — central vision preserved because macular cortex has dual blood supply from MCA + PCA) |
Patient A in hook = bitemporal hemianopia = optic chiasm compression = pituitary adenoma
Patient B in hook = left PCA infarct = right homonymous hemianopia with macular sparing
Auditory Pathway:
Cochlear hair cells → CN VIII cochlear fibres → Cochlear nuclei (pontomedullary junction) → most fibres cross via trapezoid body in pons → Superior olivary nucleus → Lateral lemniscus → Inferior colliculus (midbrain) → Medial geniculate body (MGN, metathalamus) → primary auditory cortex (areas 41/42, Heschl's gyrus, superior temporal)
- Bilateral cortical representation → unilateral cortical lesion rarely causes complete deafness
- Sensorineural deafness (cochlea or CN VIII): Rinne = AC > BC (reversed). Weber = lateralises to good ear.
- Conductive deafness: Rinne = BC > AC. Weber = lateralises to AFFECTED ear.
Olfactory Pathway:
Olfactory epithelium → CN I axons through cribriform plate of ethmoid → Olfactory bulb → Olfactory tract → divides into medial + lateral olfactory striae → Piriform cortex (primary olfactory cortex, uncus) + amygdala → entorhinal cortex → orbitofrontal cortex (conscious smell)
- Only sensory pathway that does NOT relay in the thalamus before cortex
- COVID-19 anosmia = olfactory neuroepithelium involvement (most recover)
- Olfactory groove meningioma → unilateral anosmia + ipsilateral optic atrophy + contralateral papilloedema (Foster Kennedy syndrome)
Gustatory (Taste) Pathway:
Taste buds → CN VII (ant 2/3 tongue, via chorda tympani) + CN IX (post 1/3) + CN X (epiglottis) → Nucleus tractus solitarius (NTS, medulla) → VPM thalamus (via central tegmental tract) → Gustatory cortex (inferior postcentral gyrus + anterior insula)
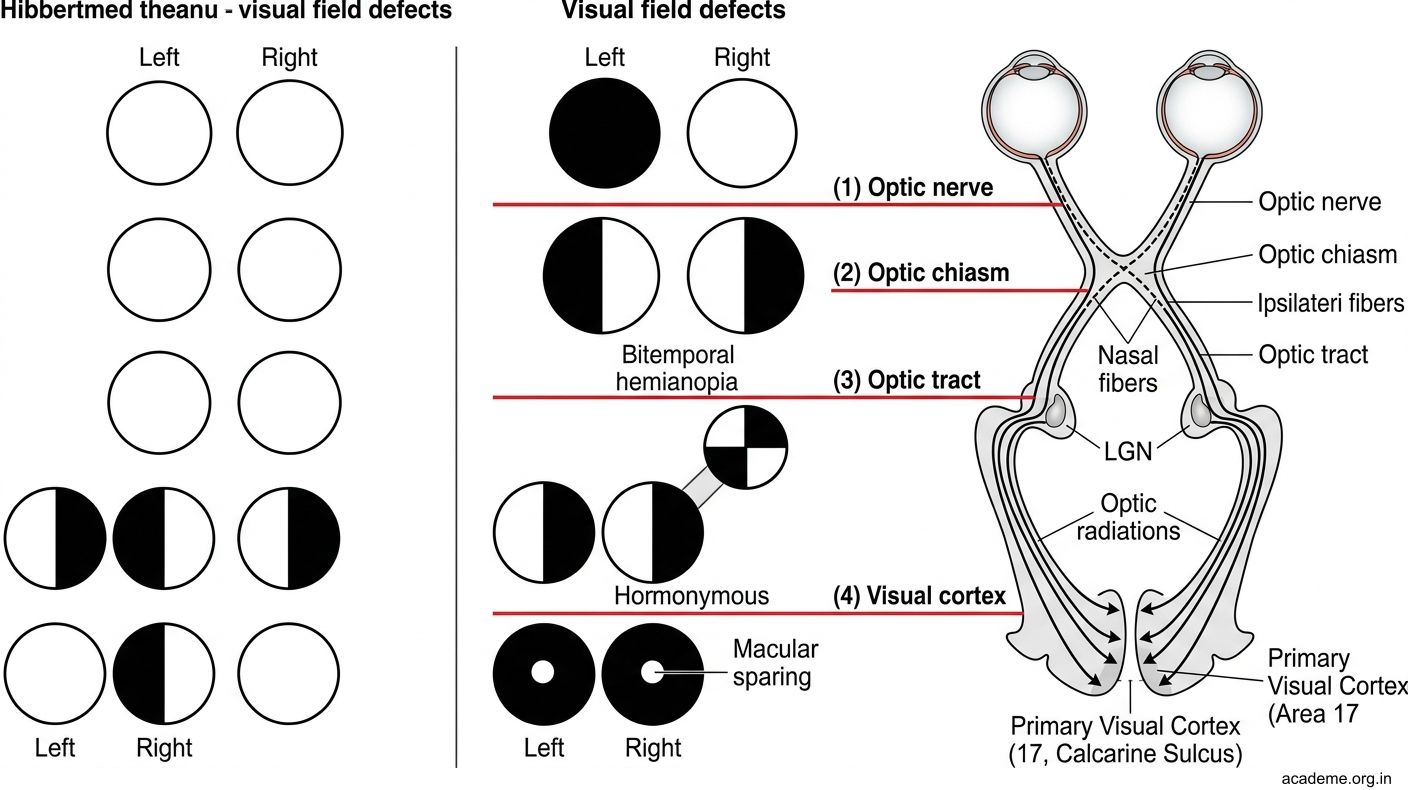
Figure: Part 3: Special Sensory Pathways (AN63.3)

Figure: Visual Field Defects by Lesion Level:

Figure: Pituitary Tumour Presentations in Indian Practice
SELF-CHECK — : Visual Pathway
A pituitary macroadenoma compresses the optic chiasm from below. The visual field defect produced is:
A. Right monocular blindness
B. Bitemporal hemianopia (loss of temporal fields of both eyes)
C. Left homonymous hemianopia
D. Right superior quadrantanopia
Reveal Answer
Answer: B. Bitemporal hemianopia (loss of temporal fields of both eyes)
Meyer's loop of the optic radiation passes through the temporal lobe and carries fibres from the inferior visual field. A right temporal lobe lesion would produce:
A. Right inferior quadrantanopia
B. Right superior quadrantanopia
C. Left superior quadrantanopia ("pie in the sky")
D. Complete right homonymous hemianopia
Reveal Answer
Answer: C. Left superior quadrantanopia ("pie in the sky")
The olfactory pathway is unique among sensory pathways because:
A. It does not relay through the thalamus before reaching the primary cortex
B. Its first-order neurons are in the thalamus
C. It crosses at the optic chiasm
D. It relays in the superior colliculus
Reveal Answer
Answer: A. It does not relay through the thalamus before reaching the primary cortex
CLINICAL PEARL
Pituitary Tumour Presentations in Indian Practice
Pituitary adenomas are the most common sellar tumours. Expansion above the sella compresses the optic chiasm → bitemporal hemianopia:
Presentation sequence as tumour grows:
1. Endocrine: Prolactinoma (galactorrhoea + amenorrhoea — most common), GH excess (acromegaly), ACTH excess (Cushing's)
2. Visual: Bitemporal hemianopia (chiasm compression)
3. Headache: Sellar stretching
4. Cavernous sinus invasion: CN III, IV, V1, VI palsies
5. Apoplexy: Sudden haemorrhage into tumour → acute visual loss + severe headache + CN palsies
Visual field testing in India: Confrontation testing (bedside), Humphrey automated perimetry. MRI pituitary (coronal views with gadolinium) for tumour characterisation. Prolactinoma: medical treatment first (cabergoline). Others: transsphenoidal surgery.
REFLECT
Return to the two patients:
- Patient A has bitemporal hemianopia. She bumps into objects at her sides because she has lost her temporal visual fields. Which fibres are cut at the optic chiasm, and why does a pituitary tumour specifically damage these?
- Patient B has right homonymous hemianopia. He can read because macular vision is spared. Which artery supplies the macular cortex area that is spared, and why is it different from the rest of the occipital cortex?
- A patient has a right temporal lobe tumour removed surgically. What visual field defect would you expect postoperatively, and which loop of the optic radiation has been damaged?
Discussion: (1) Nasal fibres (from temporal visual fields) cross at the chiasm — a tumour below the chiasm compresses these crossing fibres bilaterally → temporal field loss both eyes. (2) Macular cortex (posterior pole of occipital lobe) has dual supply from PCA + MCA; PCA infarct spares it (MCA supplies it). (3) Meyer's loop in the temporal lobe carries inferior visual field representation → right temporal resection → left superior quadrantanopia ("pie in the sky").
KEY TAKEAWAYS
Key Takeaways — Ventricular System & Special Sensory Pathways
- Ventricles: Lateral (×2) → foramen of Monro → 3rd → aqueduct of Sylvius → 4th → Magendie (median) + Luschka (lateral) → subarachnoid space
- Hydrocephalus: Aqueductal stenosis = lateral + 3rd dilated, 4th normal. Dandy-Walker = all ventricles (4th foraminal block). Treatment: VP shunt or ETV
- Visual field defects: Optic nerve = monocular blindness; Chiasm = bitemporal hemianopia (pituitary); Optic tract/radiation = homonymous hemianopia; Temporal lobe (Meyer's loop) = superior quadrantanopia; Occipital = homonymous with macular sparing
- Auditory: Cochlear nuclei → trapezoid body (cross) → lateral lemniscus → inferior colliculus → MGN → auditory cortex; bilateral cortical representation
- Olfactory: Only pathway bypassing the thalamus; piriform cortex (uncus)
- Gustatory: NTS → VPM → gustatory cortex (insula); CN VII (ant 2/3) + IX (post 1/3) + X (epiglottis)