Page 1 of 4
AN64.1-3 | Histology & Embryology (Neuroanatomy) — SDL Guide
Learning Objectives
- Describe and identify microanatomical features of the spinal cord, cerebellum, and cerebrum (AN64.1)
- Describe the development of the neural tube, spinal cord, medulla oblongata, pons, midbrain, cerebral hemisphere, and cerebellum (AN64.2)
- Describe various types of open neural tube defects and their embryological basis (AN64.3)
INSTRUCTIONS
Study histology alongside practical sections under the microscope. For embryology, trace the development from neural plate to each brain region — the week of development when each region forms determines the type of malformation from insults at that time.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Sadler's Langman's Medical Embryology, Chapter on Nervous System (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A baby girl is born at a rural hospital in Tamil Nadu. The mother had no antenatal care. At birth, a large sac is visible at the lower back, covered by a thin membrane with neural tissue exposed. The baby cannot move her legs and has no bladder control.
Another infant is born with a meningocele — a sac in the midline back covered by normal skin, no exposed neural tissue, with normal leg movements.
Both conditions are neural tube defects, but have very different outcomes. What is the embryological basis of neural tube closure, and when does it fail to cause each type?
WHY THIS MATTERS
- Neural tube defects (NTDs) — India has among the highest prevalence of NTDs globally (~4–6 per 1000 births in some regions); folate deficiency is the main preventable cause
- Folic acid supplementation — 400 mcg periconceptional folic acid reduces NTD risk by 70%; Government of India mandatory food fortification initiative
- Histology of nervous tissue — basis for understanding MS (demyelination), Alzheimer's (cortical atrophy), cerebellar tumours (Purkinje cell loss)
- Arnold-Chiari malformation — associated with myelomeningocele; causes hydrocephalus (Chiari II); common referral to Indian paediatric neurosurgeons
RECALL
Before we begin:
• The nervous system develops from neuroectoderm
• Neural plate formation occurs in week 3; neural tube closes by week 4 (Carnegie stage 11–12)
• Open NTDs occur when the neural tube fails to close
• Histology: spinal cord has grey (butterfly) + white matter; cerebellum has 3-layered cortex; cerebrum has 6-layered neocortex
Part 1: Histology of the Spinal Cord (AN64.1)
Gross structure on cross-section:
• H-shaped grey matter (posterior horn, anterior horn, lateral horn T1–L2) surrounded by white matter
• Ependymal cells line the central canal

Figure: Part 1: Histology of the Spinal Cord (AN64.1)
Microscopic features:
• Anterior horn: Large multipolar neurons (alpha motor neurons, Golgi type I), prominent Nissl bodies, occasional Golgi type II interneurons
• Posterior horn: Smaller neurons, substantia gelatinosa (Rolando) = tip of posterior horn; dense small neurons (pain modulation)
• White matter: Myelinated axons + astrocytes + oligodendrocytes; no neuronal cell bodies
• Blood-spinal cord barrier: Tight junctions in spinal cord endothelium (similar to BBB)
Identifying spinal cord in practical (key features):
1. Butterfly/H-shaped grey matter
2. Large multipolar neurons in anterior horn
3. Substantia gelatinosa (dark compact area at tip of posterior horn)
4. Central canal with ependymal cells
5. At T1–L2: lateral horn present (small neurons = preganglionic sympathetic)
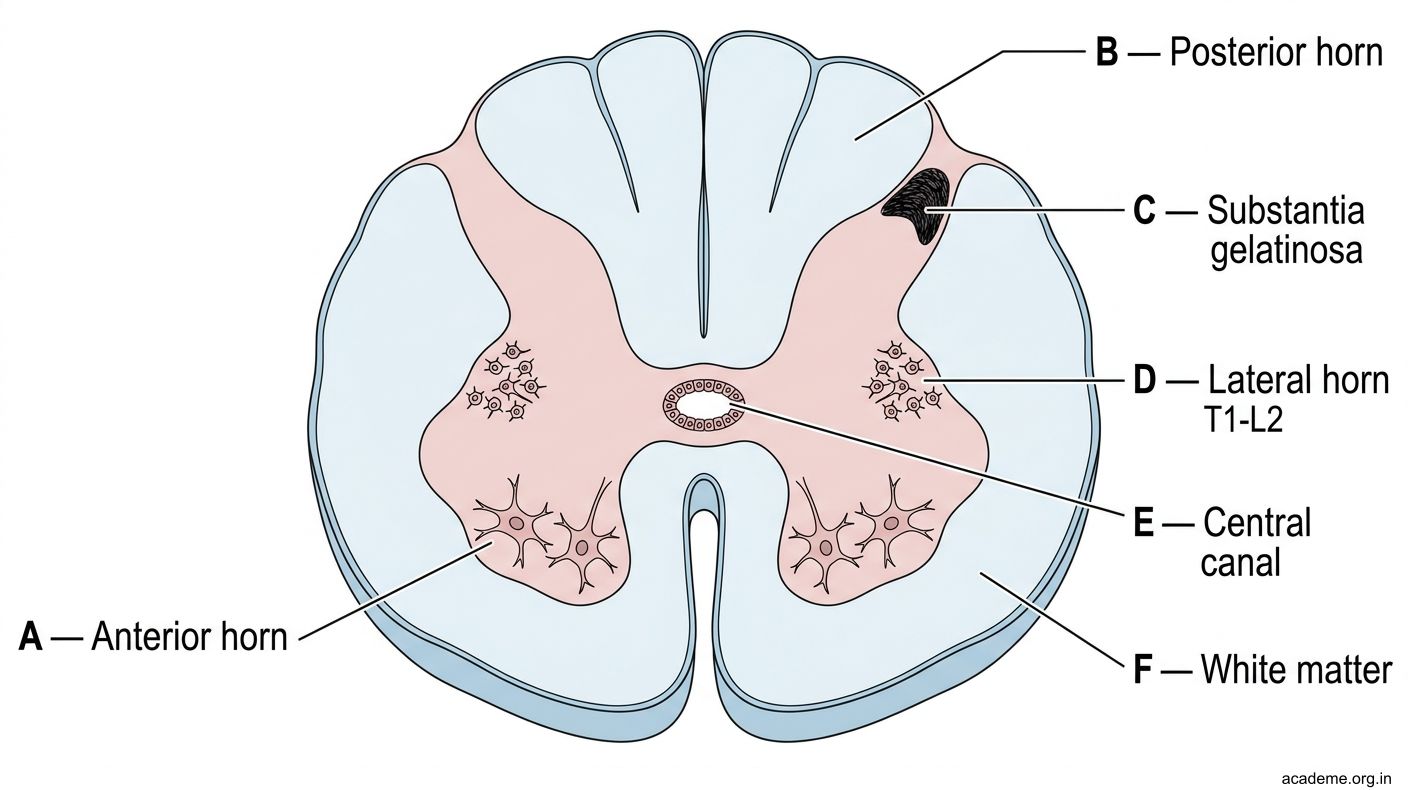
Figure: Part 1: Histology of the Spinal Cord (AN64.1)
Part 2: Histology of the Cerebellum & Cerebrum (AN64.1)
Cerebellar Cortex — 3 Layers:
| Layer | Position | Cells | Function |
|---|---|---|---|
| Molecular (outer) | Most superficial | Basket cells, stellate cells, parallel fibre axons of granule cells, Purkinje dendrites | Inhibitory interneurons; parallel fibres synapse here |
| Purkinje cell layer (middle) | Single row of large cells | Purkinje cells — large, flask-shaped, extensive dendritic tree | ONLY output of cerebellar cortex; GABAergic; inhibit deep nuclei |
| Granular (inner, deepest) | Deepest layer | Granule cells (most numerous neurons in CNS!) + Golgi cells | Granule cells = excitatory (glutamate); receive mossy fibre input; send parallel fibres up to molecular layer |
Identifying cerebellum under microscope:
1. Folial pattern (folia with core of white matter)
2. Three layers: molecular (pale, outer) → single row of large Purkinje cells → granular (dark, dense, inner)
3. Purkinje cells: distinctive large flask shape, prominent nucleolus, massive dendritic tree in molecular layer
Cerebral Cortex (Neocortex) — 6 Layers:
| Layer | Name | Key Cells | Function |
|---|---|---|---|
| I | Molecular (plexiform) | Few neurons, mostly neuropil | Dendritic arborisation |
| II | External granular | Small granule cells | Input |
| III | External pyramidal | Medium pyramidal cells | Corticocortical output |
| IV | Internal granular | Dense small granule cells | THALAMIC INPUT (main sensory input layer; best developed in sensory cortex) |
| V | Internal pyramidal | Betz cells (giant pyramidal) | MAIN CORTICAL OUTPUT (motor cortex: Betz cells → corticospinal tract) |
| VI | Multiform (fusiform) | Mixed cell types | Subcortical output, thalamocortical fibres |
Regional variations:
• Primary motor cortex (area 4): Very thick layer V (Betz cells), absent layer IV — "agranular" cortex
• Primary sensory cortex (areas 1,2,3): Prominent layer IV (koniocortex — "dust cortex" with dense granule cells), thin layer V
• Visual cortex (area 17): Line of Gennari = visible stripe in layer IV from dense myelinated thalamocortical fibres; called "striate cortex"
Identifying cerebral cortex under microscope:
1. Six layers (count them)
2. Betz cells in layer V (primary motor cortex) — largest neurons in the CNS
3. Dense layer IV (sensory cortex) — koniocortex
4. Gyri with white matter cores

Figure: Cerebellar Cortex — 3 Layers:

Figure: Cerebral Cortex (Neocortex) — 6 Layers:
Part 3: Development of the Nervous System (AN64.2)
Neural Plate Formation (Week 3, days 18–19):
• Notochord induces the overlying ectoderm to become neuroectoderm → neural plate
• Neural plate thickens, edges form neural folds, midline becomes neural groove
Neural Tube Closure (Week 4, days 22–28):
• Neural folds elevate and fuse in the midline → neural tube
• Fusion begins in the middle (future cervical region) and progresses both cranially and caudally
• Cranial neuropore closes at day 25 (Carnegie stage 11)
• Caudal neuropore closes at day 28 (Carnegie stage 12)
• Neural tube = brain (rostral) + spinal cord (caudal)
• Neural crest cells = detach from the dorsal neural tube; migrate to form: dorsal root ganglia, sympathetic ganglia, Schwann cells, adrenal medulla, melanocytes, branchial arch structures
Primary Vesicle Formation (Week 4 end):
| Vesicle | Region |
|---|---|
| Prosencephalon (forebrain) | Rostral |
| Mesencephalon (midbrain) | Middle |
| Rhombencephalon (hindbrain) | Caudal |
Secondary Vesicle Formation (Week 5):
| Primary | Divides into | Develops into |
|---|---|---|
| Prosencephalon | Telencephalon | Cerebral hemispheres, basal ganglia, hippocampus, olfactory bulb |
| Diencephalon | Thalamus, hypothalamus, retina, optic nerve | |
| Mesencephalon | (no division) | Midbrain |
| Rhombencephalon | Metencephalon | Pons + cerebellum |
| | Myelencephalon | Medulla oblongata |
| Spinal cord | — | Neural tube caudal to rhombencephalon |
Development of the Cerebral Hemispheres:
• Telencephalon balloons outward from week 5 → forms the cerebral hemispheres (expand enormously)
• Cortical neuronal migration: neurons born in the ventricular zone → migrate outward along radial glial fibres → form the 6 cortical layers in an "inside-out" pattern (earliest neurons deepest, later neurons superficial)
• Gyration begins at week 20; myelination continues until adulthood
• Corpus callosum forms by week 18–20 (agenesis of CC = failure of commissural fibres to cross)
Development of the Cerebellum:
• From the rhombic lip of the metencephalon (dorsal)
• Purkinje cells migrate from the ventricular zone
• Granule cells are born in the external granular layer (EGL) postnatally → migrate inward through the Purkinje cell layer → form the internal granular layer
• Medulloblastoma is thought to arise from remnants of the external granular layer (hence its common location in the vermis)

Figure: Part 3: Development of the Nervous System (AN64.2)

Figure: Secondary Vesicle Formation (Week 5):

Figure: Primary Vesicle Formation (Week 4 end):
Part 4: Neural Tube Defects (AN64.3)
Open Neural Tube Defects (NTDs) — Failure of Neural Tube Closure
Cranial NTDs (cranial neuropore fails to close by day 25):
| Defect | Description | Clinical |
|---|---|---|
| Anencephaly | Absence of the cranial vault + cerebral hemispheres; neural tissue exposed and degenerates; not compatible with life | Detected on antenatal US; raised maternal AFP; termination often offered |
| Encephalocele | Herniation of brain/meninges through a skull defect | Occipital (most common in India); surgical repair |
| Craniorachischisis | Failure of entire neural tube to close | Severe; rare; incompatible with life |
Spinal NTDs (caudal neuropore fails to close by day 28):
| Defect | Contents of sac | Skin cover | Neurological deficit | Infant in hook |
|---|---|---|---|---|
| Spina bifida occulta | No sac; laminar defect only | Normal skin ± tuft of hair/dimple | None usually | Not this |
| Meningocele | Meninges + CSF; no neural tissue | Normal skin | NONE or minimal | 2nd infant |
| Myelomeningocele | Meninges + CSF + neural tissue (spinal cord/roots exposed) | Thin membrane/open | Severe — paraplegia, bladder/bowel paralysis | 1st infant |
| Myeloschisis (rachischisis) | Neural tissue completely open/flat (no sac) | None — open lesion | Most severe | — |
Embryological basis:
• Failure of caudal neuropore closure → spinal canal remains open → spinal cord does not properly form/close
• The higher the level, the more severe the deficit (thoracic > lumbar > sacral)
Arnold-Chiari Malformation Type II (associated with myelomeningocele):
• Cerebellar tonsils + vermis + medulla herniate through the foramen magnum
• Causes obstructive hydrocephalus (kinking of aqueduct + hindbrain obstruction)
• Nearly ALL myelomeningocele patients have Chiari II
Risk Factors and Prevention:
• Folic acid deficiency — single most important preventable cause
• Prevention: 400 mcg folic acid DAILY from one month BEFORE conception until 12 weeks gestation (periconceptional supplementation)
• High-risk patients (previous NTD child, antiepileptics): 5 mg/day folic acid
• India: Government free folic acid supplementation through primary health centres; ICDS (Integrated Child Development Scheme) includes folate
• Diagnosis: Maternal serum AFP elevated (open defects); amniocentesis AFP + AChE; antenatal ultrasound (recommended 18–20 weeks anomaly scan)
Prenatal closure surgery (fetal MMC repair):
• Available in a few Indian centres; done at 22–26 weeks intrauterine; reduces hydrocephalus severity and improves leg function vs postnatal repair

Figure: Part 4: Neural Tube Defects (AN64.3)

Figure: Cranial NTDs (cranial neuropore fails to close by day 25):

Figure: NTD Prevention — India-Specific Public Health
SELF-CHECK — : Histology & Embryology
In the cerebellar cortex, which cell type is the largest and the only output neuron?
A. Granule cell
B. Purkinje cell
C. Basket cell
D. Stellate cell
Reveal Answer
Answer: B. Purkinje cell
Neural crest cells originate from the dorsal neural tube. Which of the following structures is NOT derived from neural crest cells?
A. Dorsal root ganglia
B. Adrenal medulla
C. Schwann cells
D. Oligodendrocytes
Reveal Answer
Answer: D. Oligodendrocytes
Myelomeningocele differs from meningocele in that:
A. Meningocele occurs in the cervical region; myelomeningocele in the lumbar region
B. Myelomeningocele is covered by normal skin; meningocele has exposed neural tissue
C. Myelomeningocele contains neural tissue (spinal cord/roots) causing neurological deficit; meningocele contains only meninges/CSF with no/minimal deficit
D. Both always cause complete paraplegia
Reveal Answer
Answer: C. Myelomeningocele contains neural tissue (spinal cord/roots) causing neurological deficit; meningocele contains only meninges/CSF with no/minimal deficit
CLINICAL PEARL
NTD Prevention — India-Specific Public Health
Periconceptional Folic Acid:
• 400 mcg/day for all women planning pregnancy (1 month before to 12 weeks after conception)
• 5 mg/day for: previous NTD, maternal diabetes, antiepileptic drugs (valproate/carbamazepine inhibit folate metabolism), obesity
Teratogens that increase NTD risk:
• Valproic acid — antiepileptic; disrupts folate metabolism + inhibits histone deacetylase; 1–2% risk of spina bifida even with folate supplementation → avoid in pregnancy if possible; use levetiracetam/lamotrigine instead
• Carbamazepine — similar but lower risk
• Methotrexate — folate antagonist
MSAFP (Maternal Serum Alpha-Fetoprotein):
• ELEVATED in open NTDs (anencephaly > myelomeningocele > meningocele/closed NTDs)
• AFP leaks from open defect into amniotic fluid → maternal serum
• Low MSAFP = Down syndrome risk
• Offered at 15–20 weeks gestation in India's triple/quadruple screen
REFLECT
Return to the two babies in the hook:
- The first baby (myelomeningocele) has paraplegia and no bladder control. Which neuropore failed to close, and at what gestational week?
- The second baby (meningocele) has a skin-covered sac but no neurological deficit. Why is neurological function preserved in meningocele?
- Both mothers had no antenatal care. Which periconceptional intervention could have reduced the risk of these defects by ~70%?
- The myelomeningocele baby also has hydrocephalus. Explain the anatomical connection between myelomeningocele and hydrocephalus.
Discussion: (1) Caudal neuropore fails to close at day 28 (week 4). (2) Meningocele = only meninges herniate; neural tissue remains in spinal canal and is normal. (3) Folic acid 400 mcg/day periconceptionally. (4) Myelomeningocele → Chiari II malformation → hindbrain/cerebellar herniation through foramen magnum → obstructs CSF flow → hydrocephalus (nearly universal in myelomeningocele).
KEY TAKEAWAYS
Key Takeaways — Neuro Histology & Embryology
- Spinal cord histology: Butterfly grey matter; large multipolar neurons in anterior horn; substantia gelatinosa at tip of posterior horn; lateral horn only T1–L2
- Cerebellum: 3 layers: Molecular (outer, basket/stellate cells) → Purkinje cell layer (single row, GABAergic, only output) → Granular (granule cells — most numerous in CNS)
- Cerebrum: 6 layers; Layer IV = thalamic input (prominent in sensory cortex); Layer V = main output (Betz cells in motor cortex = largest CNS neurons)
- Neural tube development: Week 3: neural plate. Week 4: neural tube closes (cranial neuropore day 25; caudal day 28). Week 5: 5 secondary vesicles
- Neural crest → DRG, sympathetic ganglia, Schwann cells, adrenal medulla, melanocytes
- NTDs: Meningocele (meninges only, skin-covered, no deficit) vs Myelomeningocele (neural tissue, thin membrane, severe deficit). Prevention: periconceptional folic acid