Page 1 of 4
AN65.1-2 | Epithelium histology — SDL Guide
Learning Objectives
- Identify and classify epithelium under the microscope correlating type to function (AN65.1)
- Describe the ultrastructure of epithelium including junctional complexes, microvilli, cilia, and basement membrane (AN65.2)
- Apply knowledge of epithelial types to explain pathological changes in Indian clinical practice (AN65.1)
INSTRUCTIONS
Study this module alongside your histology atlas and practical slides. When you encounter an epithelium, always ask: (1) How many cell layers? (2) What shape are the surface cells? (3) What is the function of this surface? This systematic approach will allow you to identify any epithelium under the microscope.
References
- BD Chaurasia's Human Anatomy, Vol. 1 — General Histology (Textbook)
- Junqueira's Basic Histology — Text and Atlas, 16th Edition (Textbook)
- Gray's Anatomy — Histological Foundation (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 58-year-old chronic smoker from Chennai presents with hoarseness of voice for 3 months. He smokes 20 cigarettes daily for 30 years. Indirect laryngoscopy reveals an irregular lesion on the left vocal cord. Biopsy shows "squamous metaplasia with dysplasia."
The pathologist's report states: "Normal respiratory pseudostratified ciliated columnar epithelium replaced by stratified squamous epithelium; atypical cells with increased nuclear:cytoplasmic ratio present."
Why does the larynx normally have ciliated columnar epithelium? Why does smoking cause squamous metaplasia? What is the significance of finding stratified squamous instead of ciliated columnar cells?
Understanding epithelial types and their functional basis is essential to interpreting biopsy reports across all specialties.
WHY THIS MATTERS
Epithelial histology is encountered daily in Indian clinical practice:
- Biopsy interpretation — every surgical pathology report describes epithelial type (squamous, columnar, transitional); clinicians must understand what is normal vs abnormal at each site
- Metaplasia and cancer risk — squamous metaplasia of respiratory or gastric mucosa (Barrett's oesophagus, common in India) → dysplasia → carcinoma; understanding normal epithelium is prerequisite
- Cervical Pap smear — the transformation zone between stratified squamous and columnar epithelium at the cervical os is the site of cervical carcinoma; understanding this junction is essential
- NMC 2024 CBME (AN65.1–65.2) — mandates microscopic identification and ultrastructural knowledge of epithelium
- Practical examinations — histology slides of epithelium are standard in MBBS practical examinations across all Indian medical colleges
RECALL
Before we begin, recall:
- Epithelium = avascular tissue covering all body surfaces (external and internal), derived from all three germ layers
- Key features: (1) Cells in continuous sheets; (2) No blood vessels (nourished by diffusion from underlying connective tissue); (3) Rests on a basement membrane; (4) High regenerative capacity
- Classification basis: (1) Number of layers — Simple (1 layer) vs Stratified (multiple layers) vs Pseudostratified (all cells touch basement membrane but not all reach surface); (2) Shape of surface cells — Squamous (flat), Cuboidal, Columnar
- Germ layer origins: Ectoderm → skin epidermis; Endoderm → GI, respiratory, glandular epithelia; Mesoderm → mesothelium (pleura, peritoneum, pericardium), endothelium
Part 1: Classification and Types of Epithelium (AN65.1)
Simple Epithelia — one cell layer, all cells touch the basement membrane:
| Type | Shape | Location | Function | Identifying Feature |
|---|---|---|---|---|
| Simple squamous | Flat, scale-like | Alveoli, Bowman's capsule, endothelium, mesothelium | Diffusion, filtration, lubrication | Flat nucleus, minimal cytoplasm |
| Simple cuboidal | Cube-shaped | Kidney tubules, thyroid follicles, ovarian surface | Secretion, absorption | Round central nucleus, height ≈ width |
| Simple columnar | Tall, column-like | Small intestine, stomach, large intestine | Absorption, secretion | Oval basal nucleus, may have goblet cells |
| Pseudostratified columnar | Varying heights, all touch BM | Trachea, bronchi, epididymis | Mucociliary clearance, sperm transport | Nuclei at different levels; all cells touch basement membrane |
Stratified Epithelia — multiple cell layers, classified by surface cell shape:
| Type | Surface cells | Location | Function |
|---|---|---|---|
| Stratified squamous (non-keratinised) | Flat, nucleated | Oral mucosa, oesophagus, vagina, cornea | Protection against abrasion; remains moist |
| Stratified squamous (keratinised) | Flat, anucleate (keratin-filled) | Skin (epidermis) | Protection against dehydration and abrasion |
| Stratified cuboidal | Cuboidal surface | Sweat gland ducts, large excretory ducts | Secretion |
| Stratified columnar | Columnar surface | Rare: conjunctiva, parts of urethra | Protection + secretion |
| Transitional (urothelium) | Dome-shaped (relaxed) / flat (distended) | Urinary bladder, ureters, renal pelvis | Stretches without allowing urine to pass through (watertight) |
Special adaptations of surface cells:
• Goblet cells — unicellular mucus-secreting glands interspersed in simple columnar and pseudostratified epithelium of intestines and respiratory tract; secrete mucin (protective)
• Cilia — motile projections (9+2 microtubule arrangement) on respiratory pseudostratified epithelium; beat rhythmically to move mucus toward pharynx (mucociliary escalator)
• Microvilli — non-motile projections (actin core) forming the "brush border" of small intestinal columnar cells and the "striated border" of proximal kidney tubules; massively increase surface area for absorption

Figure: Part 1: Classification and Types of Epithelium (AN65.1)

Figure: Stratified Epithelia — multiple cell layers, classified by surface cell shape:
Part 2: Ultrastructure of Epithelium (AN65.2)
Junctional Complex — the apical seal between adjacent epithelial cells (from apex to base):

Figure: Part 2: Ultrastructure of Epithelium (AN65.2)
1. Tight junction (Zonula occludens) — SEALING junction
• Outermost junction (most apical)
• Integral membrane proteins (claudins, occludins) fuse the outer leaflets of adjacent cell membranes → creating a seal that prevents paracellular passage of molecules
• Clinical: Tight junction disruption → leaky gut (in Crohn's disease, NSAID-induced enteropathy — common in India), increased intestinal permeability
2. Adherens junction (Zonula adherens) — ADHESION junction
• Below tight junction
• E-cadherin transmembrane proteins + actin microfilament belt inside
• Holds cells together; loss of E-cadherin → epithelial-to-mesenchymal transition (EMT) → cancer invasion
3. Desmosome (Macula adherens) — SPOT WELD junction
• Scattered along lateral membranes below adherens junction
• Cadherins (desmogleins, desmocollins) + intermediate filaments (cytokeratins) inside
• Strongest mechanical junction; resists shearing forces
• Clinical: Pemphigus vulgaris (autoimmune, anti-desmoglein antibodies) → skin blisters; Rare in India but tested in pathology
4. Gap junction (Nexus) — COMMUNICATION junction
• Connexin proteins form channels (connexons) linking cytoplasm of adjacent cells
• Allows passage of ions and small molecules → cell-to-cell communication, electrical coupling
• Critical in cardiac muscle (intercalated discs) and smooth muscle for coordinated contraction
Basement membrane — the foundation:
• Not a true membrane; extracellular matrix layer produced by epithelial cells + fibroblasts
• Composition: Type IV collagen (structural scaffold) + laminin (cell adhesion) + heparan sulphate proteoglycans + fibronectin
• Two zones on EM: Lamina lucida (inner, contains laminin) + Lamina densa (outer, contains type IV collagen)
• Functions: (1) Structural support; (2) Selectively permeable barrier (molecular sieve); (3) Regulates cell behaviour (polarity, proliferation, differentiation)
• Clinical: Diabetic nephropathy → thickening of glomerular basement membrane (GBM) → proteinuria; Alport syndrome → type IV collagen mutation → GBM defects
Cilia ultrastructure (9+2 arrangement):
• Axoneme = 9 outer doublet microtubules + 1 central pair
• Dynein arms generate movement by sliding microtubules
• Clinical: Primary ciliary dyskinesia (Kartagener syndrome) → dynein arm defect → immotile cilia → recurrent respiratory infections + situs inversus
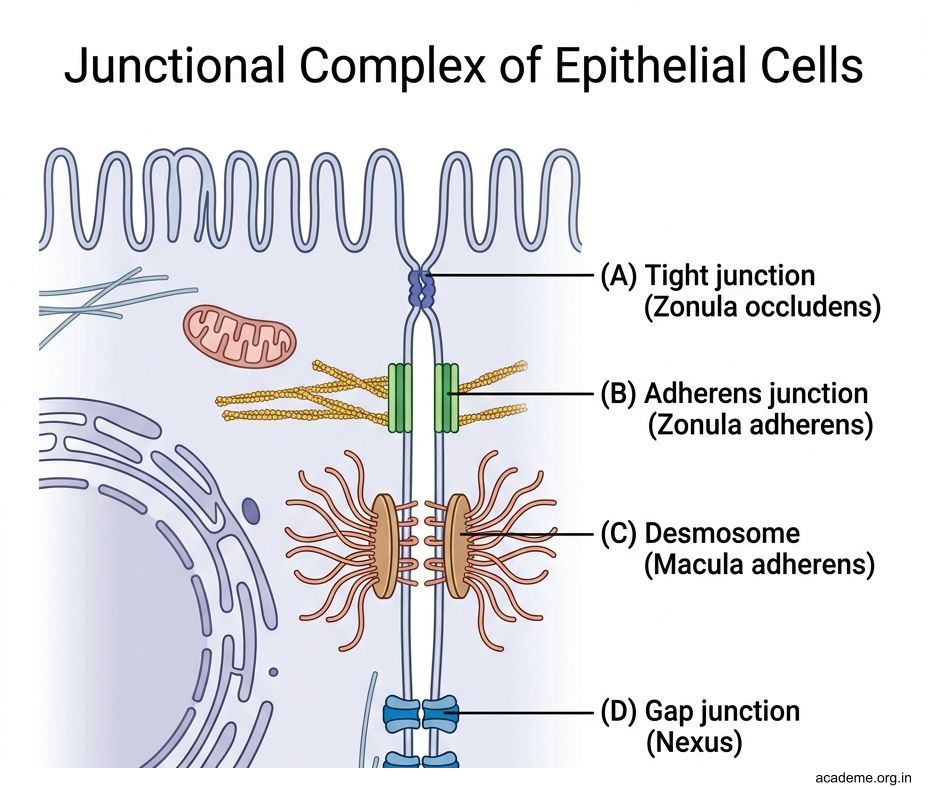
Figure: Part 2: Ultrastructure of Epithelium (AN65.2)

Figure: Metaplasia — Epithelial Adaptation to Chronic Irritation

Figure: Common examples in Indian patients:
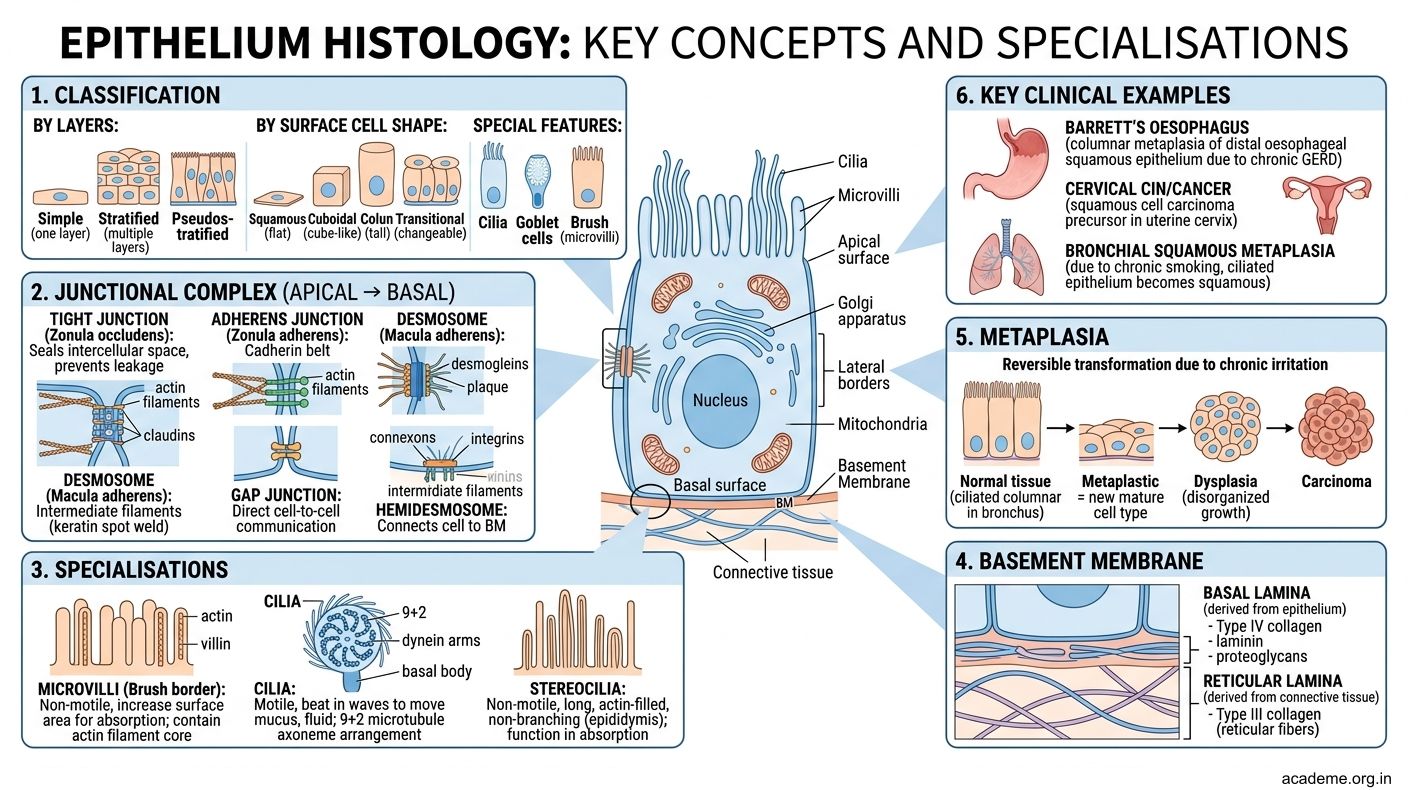
Figure: Key Takeaways — Epithelium Histology (AN65.1–65.2)
SELF-CHECK — : Epithelium
The epithelium lining the urinary bladder that can change shape between relaxed and distended states is:
A. Stratified squamous non-keratinised
B. Pseudostratified columnar
C. Transitional (urothelium)
D. Simple columnar with goblet cells
Reveal Answer
Answer: C. Transitional (urothelium)
In primary ciliary dyskinesia (Kartagener syndrome), the ultrastructural defect responsible for immotile cilia is absence of:
A. Central pair of microtubules
B. Dynein arms on outer doublets
C. Connexin proteins in gap junctions
D. Desmoglein in desmosomes
Reveal Answer
Answer: B. Dynein arms on outer doublets
The junction that acts as the "paracellular seal" preventing molecules from passing between adjacent epithelial cells is the:
A. Tight junction (zonula occludens)
B. Adherens junction (zonula adherens)
C. Desmosome (macula adherens)
D. Gap junction (nexus)
Reveal Answer
Answer: A. Tight junction (zonula occludens)
CLINICAL PEARL
Metaplasia — Epithelial Adaptation to Chronic Irritation
Metaplasia = replacement of one fully differentiated cell type by another differentiated cell type. It is a reversible change if the irritant is removed.
Common examples in Indian patients:
| Site | Normal epithelium | Metaplastic type | Cause | Risk |
|---|---|---|---|---|
| Trachea/Bronchus | Pseudostratified ciliated columnar | Stratified squamous | Cigarette smoking | Squamous cell carcinoma lung |
| Oesophagus (Barrett's) | Stratified squamous | Specialised intestinal columnar | Chronic GERD | Adenocarcinoma oesophagus |
| Cervix (transformation zone) | Stratified squamous ↔ columnar | Squamous metaplasia of columnar | HPV infection, hormones | Cervical carcinoma (most common gynaecological cancer in India) |
| Stomach (intestinal metaplasia) | Simple columnar (gastric) | Intestinal columnar with goblet cells | H. pylori, chronic gastritis | Gastric adenocarcinoma |
Key principle: Metaplasia itself is NOT cancer, but it indicates chronic injury and creates a milieu for dysplasia → carcinoma in situ → invasive carcinoma. Understanding the normal epithelium is essential to recognising when it has been replaced.
REFLECT
Return to the hook case — the chronic smoker with hoarseness and vocal cord biopsy showing squamous metaplasia:
- What is the normal epithelial type of the trachea and major bronchi? What is its specific function relevant to smoking injury?
- Why does smoking cause squamous metaplasia (hint: think about what smoking destroys first)?
- The biopsy shows "atypical cells with increased nuclear:cytoplasmic ratio." Which stage of the metaplasia → carcinoma sequence does this represent?
- If the lesion progresses to invasive squamous cell carcinoma and the surgeon takes a section of the tumour, which ultrastructural junctions would be LOST, contributing to tumour cell invasion?
Discussion: The respiratory tract is lined by pseudostratified ciliated columnar epithelium with goblet cells. Smoking paralyses cilia first (mucociliary clearance impaired) → chronic mucus stasis → epithelial irritation → squamous metaplasia (more protective against direct injury but loses the mucociliary function). Dysplasia (atypical cells) = pre-malignant stage between metaplasia and carcinoma in situ. Cancer invasion involves loss of E-cadherin (adherens junction) → EMT.
KEY TAKEAWAYS
Key Takeaways — Epithelium Histology (AN65.1–65.2)
Classification:
• Simple (1 layer): squamous (alveoli, endothelium), cuboidal (kidney tubules, thyroid), columnar (intestines), pseudostratified columnar (trachea)
• Stratified: squamous non-keratinised (oesophagus, oral mucosa), keratinised (skin), transitional (bladder)
Identify on slide:
1. Count layers: one = simple; many = stratified; appears many but all touch BM = pseudostratified
2. Shape of surface cells: flat = squamous; cube = cuboidal; tall = columnar; dome = transitional
3. Special features: cilia (respiratory), goblet cells (intestines, trachea), microvilli/brush border (small intestine, proximal tubule)
Ultrastructure — junctional complex (apex → base):
• Tight junction (zonula occludens) → Adherens junction (zonula adherens) → Desmosome (macula adherens) → Gap junction (nexus)
• Basement membrane: lamina lucida (laminin) + lamina densa (type IV collagen)
Clinical:
• Squamous metaplasia (smoking → lung cancer; Barrett's → adenocarcinoma)
• Pemphigus vulgaris (anti-desmoglein → blisters)
• Kartagener syndrome (dynein arm defect → immotile cilia)
• Diabetic nephropathy (GBM thickening)