Page 1 of 6
AN8.1-4 | Features of individual bones (Upper Limb) — SDL Guide
The skeleton of the upper limb is built from seven bone groups — two girdle bones, one arm bone, two forearm bones, eight carpal bones, five metacarpals, and fourteen phalanges. In this module you will learn to identify each bone, determine its side, name its important features, locate the muscle attachments that clinical anatomy depends on, and understand the special clinical significance of the scaphoid and pisiform. The skills you build here underpin every upper-limb examination and every fracture you will diagnose in clinical years.
Learning Objectives
- Identify the clavicle, scapula, humerus, radius, ulna, and carpal bones; determine their side and anatomical position (AN8.1)
- Describe the important features and joint formations of each upper limb bone (AN8.1)
- Demonstrate important muscle attachments on each bone (AN8.2)
- Identify and name the bones of the articulated hand; specify the parts of metacarpals and phalanges; enumerate the peculiarities of the pisiform (AN8.3)
- Describe scaphoid fracture and explain the anatomical basis of avascular necrosis of the scaphoid (AN8.4)
INSTRUCTIONS
Work through the five sections in order. Each section introduces 3–4 key terms; bold them in your notes. Complete the self-check questions before moving on. Have your atlas and a bone specimen (or diagram) alongside as you read.
References
- Gray's Anatomy for Students (Drake et al.) — Chapter 7: Upper Limb (Textbook)
- BD Chaurasia's Human Anatomy, Vol. 1 — Upper Limb (Textbook)
- Clinically Oriented Anatomy (Moore et al.) — Pectoral Girdle and Upper Limb (Textbook)
- OpenStax Anatomy and Physiology 2e — Ch 8: The Appendicular Skeleton (CC BY 4.0) (Open Access)
Version 2.0 | Academe Content Engine v2, Faculty Review Pending
CLINICAL SCENARIO
A 22-year-old medical student playing cricket at the SBV college ground falls awkwardly — he lands on his outstretched right hand. At the government hospital emergency, the X-ray is reported as normal. Yet the casualty MO notices exquisite tenderness in the small depression at the base of his thumb when the thumb is extended. The MO sends him for an MRI and immobilises the wrist.
Why the MRI when the X-ray is normal? What is that depression called? Which bone is most likely fractured? And why — if missed — could this injury cause lifelong wrist pain?
By the end of this module, you will answer all four questions with anatomical precision.
WHY THIS MATTERS
Fractures of upper limb bones are the most common bony injuries in India — from road traffic accidents on National Highways to falls in paddy fields, and sporting injuries at medical college grounds. Knowing the bony anatomy precisely means:
- You can determine side of a bone specimen (mandatory in practical exams — and in the mortuary or court)
- You can identify muscle attachments, which tells you which way a fracture fragment will displace
- You can explain avascular necrosis of the scaphoid — the classic missed fracture of the wrist
- You can localise nerve injuries to the bony grooves and notches where nerves are most vulnerable
Orthopaedic surgeons, emergency physicians, and physiotherapists all depend on this knowledge daily.
RECALL
From your earlier anatomy sessions on general bone features (AN2.1–AN2.4), you already know:
- Bone types: long bones (humerus, radius, ulna) have diaphysis + epiphyses; flat bones (scapula) have inner and outer compact tables with cancellous bone between
- The periosteum covers all bone except at articular surfaces; it carries blood vessels and osteoprogenitor cells for repair
- Processes are projections for muscle attachment; fossae are depressions; foramina are holes for nerves/vessels
- The epiphyseal plate is the growth zone in long bones — injuries here in children are serious (Salter-Harris fractures)
Now we will apply these principles to the specific bones of the upper limb.
The Clavicle — The Strut of the Shoulder
The clavicle (Latin: clavicula = small key) is the only long bone that lies horizontally. It is the strut connecting the shoulder girdle to the axial skeleton.
How to determine side:
The clavicle has a medial (sternal) end that is rounded and articulates with the manubrium of the sternum (forming the sternoclavicular joint — the only joint between the upper limb and the axial skeleton). The lateral (acromial) end is flat and articulates with the acromion of the scapula (acromioclavicular joint).
The shaft is curved — convex anteriorly at the medial two-thirds (where it overlies the neurovascular bundle), concave anteriorly at the lateral one-third (like an "S" when viewed from above). The inferior surface has:
• Subclavian groove (medial) — where subclavius muscle lies, protecting the subclavian vessels
• Conoid tubercle and trapezoid ridge at the lateral end — attachment of the coracoclavicular ligament (which suspends the scapula from the clavicle)
• Deltoid tubercle at the lateral end (anterior) — deltoid attachment
Key muscle attachments:
• Sternocleidomastoid (medial end, superior) — rotates and tilts head
• Trapezius (lateral one-third, posterior/superior) — elevates and retracts the shoulder
• Deltoid (lateral one-third, anterior/inferior) — abducts arm
• Pectoralis major (medial two-thirds, anterior) — adducts and flexes arm
• Subclavius (inferior surface, subclavian groove) — depresses the clavicle
Clinical points:
The clavicle is the most commonly fractured bone in the body (especially at the junction of its medial two-thirds and lateral one-third — the weakest point). In a clavicle fracture, the medial fragment is pulled up by sternocleidomastoid; the lateral fragment drops with the weight of the arm. The subclavian vessels and brachial plexus just posterior-inferior to the clavicle are at risk in displaced fractures.

Figure: The Clavicle — The Strut of the Shoulder
SELF-CHECK — : Clavicle
A patient has a fractured clavicle at the junction of its medial two-thirds and lateral one-third. The medial fragment is displaced upwards. Which muscle is responsible?
A. Trapezius
B. Sternocleidomastoid
C. Deltoid
D. Pectoralis major
Reveal Answer
Answer: B. Sternocleidomastoid
Which ligament is attached to the conoid tubercle and trapezoid ridge on the inferior surface of the clavicle?
A. Costoclavicular ligament
B. Interclavicular ligament
C. Coracoclavicular ligament
D. Acromioclavicular ligament
Reveal Answer
Answer: C. Coracoclavicular ligament
The Scapula — The Mobile Platform
The scapula (shoulder blade) is a flat triangular bone lying on the posterolateral chest wall, covering ribs 2–7. It is highly mobile — can elevate, depress, protract, retract, and rotate — making it the platform for all shoulder movements.
Surfaces and borders:
• Costal (anterior) surface: The large subscapular fossa — origin of subscapularis (medial rotator of the arm; part of the rotator cuff)
• Posterior (dorsal) surface: Divided by the spine of the scapula into the supraspinous fossa (above, origin of supraspinatus) and infraspinous fossa (below, origin of infraspinatus)
• Three borders: Medial (vertebral), lateral (axillary), and superior; three angles: superior, inferior, and lateral
• Glenoid cavity: The lateral angle bears the shallow oval articular socket that forms the glenohumeral (shoulder) joint with the humeral head
Processes:
• Spine of the scapula — projects posteriorly; its lateral continuation is the acromion (the "roof" of the shoulder, covered by the deltoid and trapezius)
• Coracoid process — a hook-like projection anteriorly at the superior angle; origin/attachment of: short head of biceps brachii, coracobrachialis, and pectoralis minor
Key muscle attachments (posterior):
• Supraspinous fossa → supraspinatus (initiates abduction; rotator cuff)
• Infraspinous fossa → infraspinatus (lateral rotator; rotator cuff)
• Lateral border of infraspinous fossa → teres minor (lateral rotation; rotator cuff)
• Inferior angle (costal surface) → serratus anterior (protracts scapula; "boxer's muscle"); if paralysed, winging of scapula results (long thoracic nerve injury)
• Medial border (costal surface) → serratus anterior (lower portion)
How to determine side: Hold the scapula with the glenoid facing laterally and the spine pointing posteriorly. The spine, when you trace it, leads to the acromion on the lateral side. The coracoid points anteriorly. The subscapular fossa (smooth concave surface) faces anteriorly and the two fossae (rough) face posteriorly.
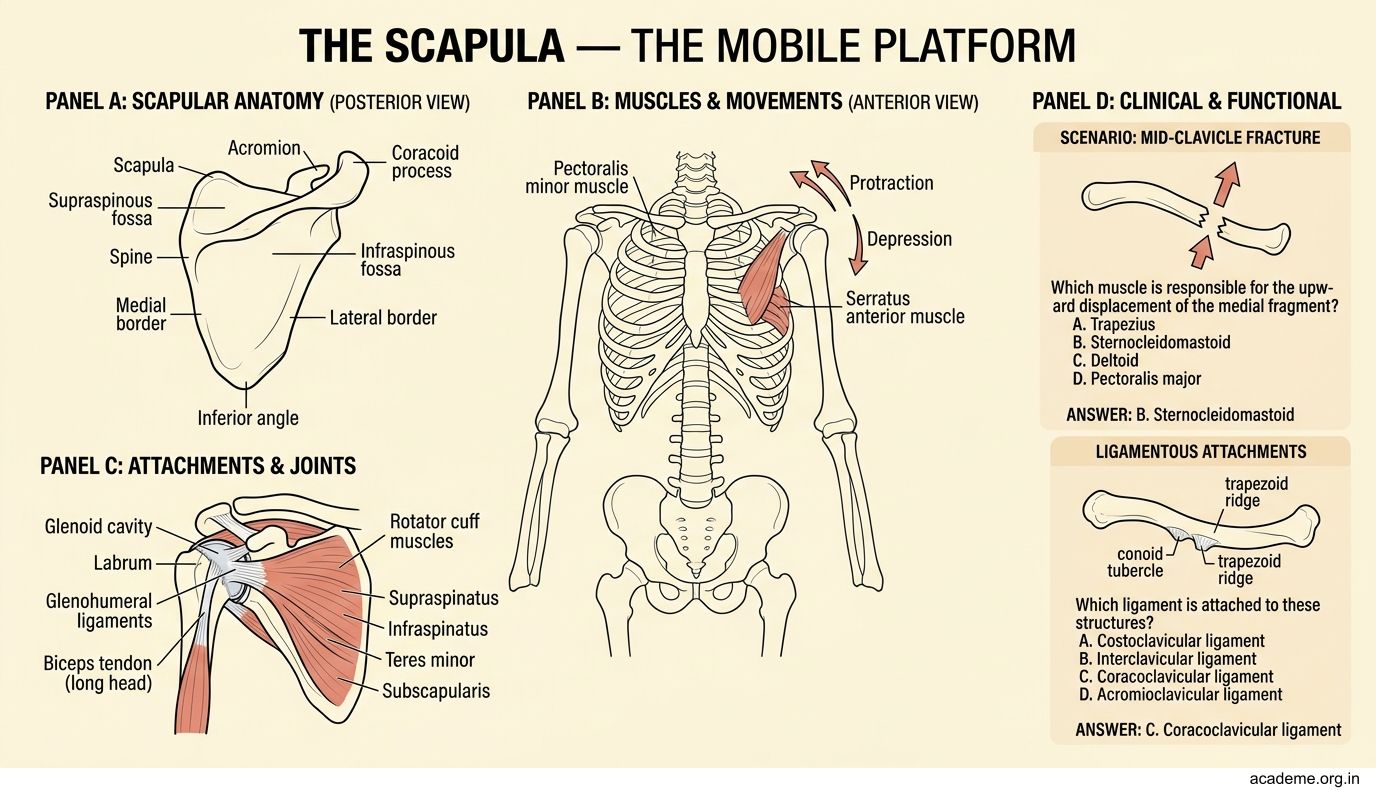
Figure: The Scapula — The Mobile Platform
The Humerus — Key Features and Clinical Grooves
The humerus is the long bone of the arm, articulating proximally with the glenoid (shoulder joint) and distally with the radius and ulna (elbow joint).
Upper end:
• Head — smooth hemisphere, covered with articular cartilage; faces medially, upwards, and backwards
• Anatomical neck — the constriction just distal to the head, between head and tuberosities (site of growth plate in children)
• Greater tubercle — lateral prominence; attachment of the rotator cuff muscles: supraspinatus (superior facet), infraspinatus (middle facet), teres minor (inferior facet)
• Lesser tubercle — anterior; attachment of subscapularis
• Bicipital (intertubercular) groove — between the two tubercles; the long head of biceps tendon passes through it; the groove is guarded by the transverse humeral ligament
• Surgical neck — the narrowed shaft just below the tuberosities (not the head); this is where most proximal humeral fractures occur; the axillary nerve and posterior circumflex humeral artery pass close here
Shaft:
• Deltoid tuberosity — mid-lateral surface; attachment of deltoid (abductor of the arm; the most important abductor beyond 90°)
• Spiral groove (radial groove) — runs obliquely on the posterior surface; the radial nerve and profunda brachii artery lie in this groove; mid-shaft fractures can injure the radial nerve here → wrist drop
• Nutrient foramen — anterior surface, directed upward (rule: "away from the elbow for upper limb")
Lower end:
• Capitulum — rounded lateral projection, articulates with the radius
• Trochlea — pulley-shaped medial projection, articulates with the ulna; it is wider anteriorly than posteriorly
• Medial epicondyle — medial prominence; attachment of the common flexor origin (flexors of the forearm); the ulnar nerve passes in its groove posteriorly → vulnerable in medial epicondyle fractures
• Lateral epicondyle — lateral prominence; attachment of the common extensor origin
• Olecranon fossa (posterior), coronoid fossa and radial fossa (anterior) — accommodate the ulna and radius during flexion/extension
How to determine side: Hold humerus vertically with the rounded head uppermost. The head faces medially; the olecranon fossa is posterior; the medial epicondyle is larger and more prominent than the lateral. The capitulum is on the lateral side (same side as radius).

Figure: The Humerus — Key Features and Clinical Grooves
CLINICAL PEARL
The radial nerve in the spiral groove of the humerus is the classic site of nerve injury in mid-shaft humeral fractures — a common injury in Indian hospitals (road traffic accidents, "nightstick" fractures). The result is wrist drop (inability to extend the wrist and fingers).
However, not all wrist drops are from mid-shaft fractures:
• Axillary radial nerve injury (crutch palsy, "Saturday night palsy") → wrist drop + loss of elbow extension (triceps paralysed) + sensory loss on posterior arm
• Spiral groove injury → wrist drop, triceps usually spared (branches leave proximal to the groove)
• Posterior interosseous nerve injury (at lateral epicondyle/supinator) → finger drop without wrist drop (ECRL intact)
Always test the triceps reflex and the sensory loss distribution to localise the level.