Page 2 of 11
CM13.{1-2,4} | CM13.{1-2,4} | Disaster Concepts, Cycle and Authority — SDL Guide (Part 2)
National Disaster Management Authority (NDMA)
India's institutional response to the 2004 tsunami was a turning point. The disaster exposed the absence of a unified national authority with clear statutory powers and resources. The Government of India responded by enacting the Disaster Management Act 2005 (Act 53 of 2005) — the first comprehensive disaster management legislation in India. The Act established a three-tier institutional framework that operates from the national to the district level.
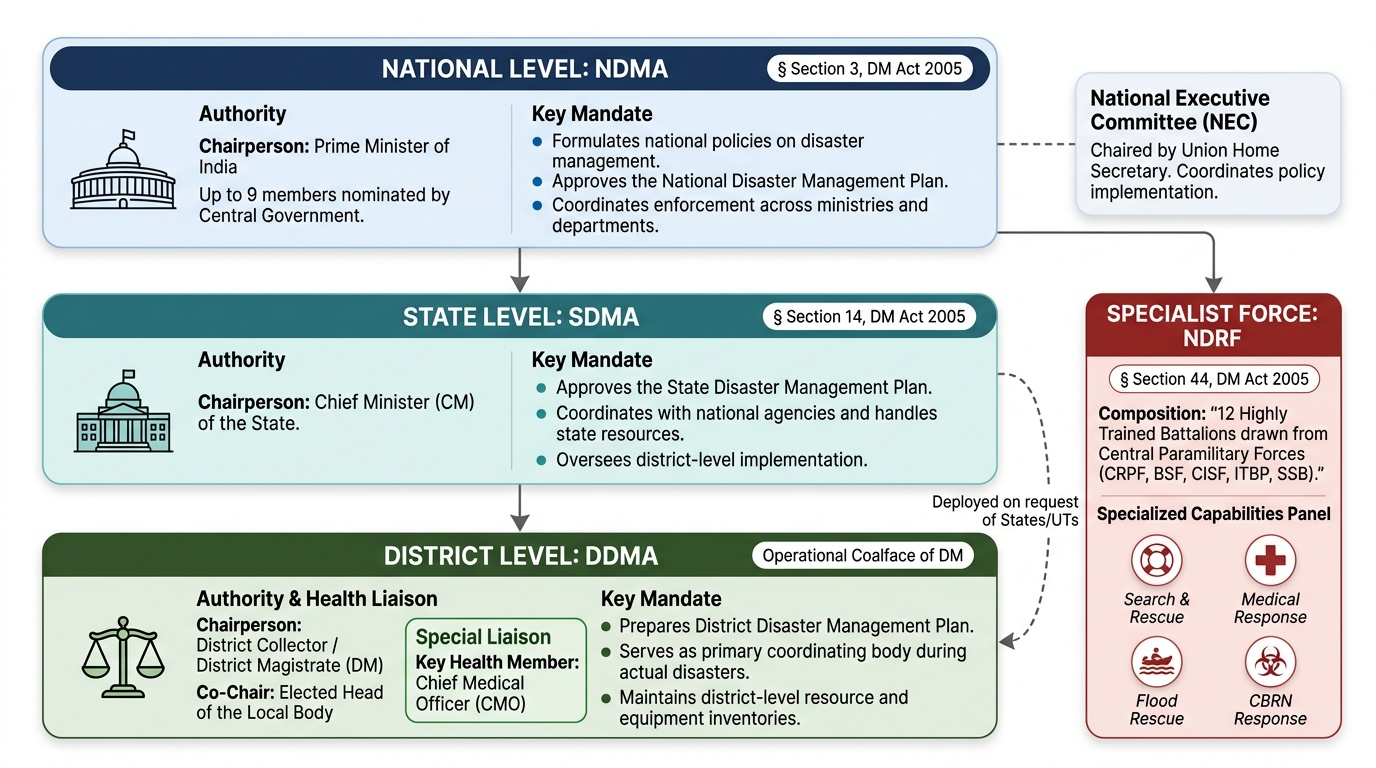
National Disaster Management Authority (NDMA) is the apex statutory body established under Section 3 of the DM Act 2005. The NDMA is chaired by the Prime Minister of India — a deliberate design choice that gives it the highest political authority for cross-ministry coordination. The NDMA consists of the Chairperson (PM) and up to nine members nominated by the central government. Its mandate includes: laying down policies on disaster management, approving the National Disaster Management Plan, and coordinating the enforcement of policies across ministries and departments. NDMA is supported by the National Executive Committee (NEC) — chaired by the Union Home Secretary — which coordinates the implementation activities.
State Disaster Management Authority (SDMA) is established in each state under Section 14 of the DM Act 2005. The SDMA is chaired by the Chief Minister of the state. The SDMA lays down the State Disaster Management Plan, coordinates with central agencies, and oversees district-level implementation.
District Disaster Management Authority (DDMA) is the operational coalface of disaster management. The DDMA is chaired by the District Collector (or District Magistrate) with the elected head of the local body as co-chair. The DDMA prepares the district disaster management plan, coordinates response during an actual disaster, and maintains the district-level resource inventory. The Chief Medical Officer (CMO) at the district level is the key health sector member of the DDMA.
National Disaster Response Force (NDRF) is the specialised rapid-response force established under Section 44 of the DM Act. The NDRF consists of 12 battalions drawn from central paramilitary forces (CRPF, BSF, CISF, ITBP, SSB), specially trained in search and rescue, medical first response, flood rescue, and CBRN response. NDRF battalions are deployed at the request of states and UTs during disasters.
Provided image
The significance of this framework for a community physician is direct. When a disaster strikes your district, you are part of the DDMA machinery. Your CMO reports to the DDMA; your public health actions are coordinated through the DDMA's emergency operations centre. Knowing this structure — and knowing who to call and who to report to — is the difference between effective and chaotic medical response.
SELF-CHECK
Under India's Disaster Management Act 2005, who chairs the District Disaster Management Authority (DDMA)?
A. A. The Chief Minister of the state
B. B. The Chief Medical Officer of the district
C. C. The District Collector (District Magistrate)
D. D. The Prime Minister's representative
Reveal Answer
Answer: C. C. The District Collector (District Magistrate)
The DDMA is chaired by the District Collector (or District Magistrate) — the senior-most administrative officer at the district level — with the elected head of the local body as co-chair. The CM chairs the SDMA (state level), and the PM chairs the NDMA (national level). The CMO is a key health sector member but not the chair.
Evaluating Disaster Preparedness and Response
Evaluation is the often-neglected but essential phase that closes the disaster management cycle. Without systematic evaluation of preparedness plans and response actions, the same errors recur in the next disaster. Evaluation in disaster management operates at two levels: pre-disaster preparedness evaluation (measuring readiness before a disaster strikes) and post-disaster after-action review (assessing what worked and what failed during response).
Pre-disaster preparedness is evaluated through several mechanisms. Mock drills and simulation exercises are the gold standard for testing preparedness plans under realistic (but safe) conditions. NDMA's guidelines mandate annual multi-hazard mock drills at the district level involving all emergency response agencies. Drills assess: notification and warning chain activation time; mobilisation of resources (ambulances, rescue equipment) within target timeframes; inter-agency communication and command coordination; and community evacuation behaviour. A drill that reveals failures is more valuable than one that runs perfectly — failures caught in a drill are prevented in a real disaster.
Resource inventories at the district level must be audited regularly: stockpiled medicines, food rations, water purification tablets, rescue boats, tents, and generator sets all have shelf-lives and maintenance requirements. Community risk mapping — identifying which localities are most exposed and which populations are most vulnerable — provides the spatial intelligence that guides resource pre-positioning.
Post-disaster response evaluation uses the after-action review (AAR) methodology. An AAR is a structured debrief conducted as soon as possible after the response phase, involving all agencies that participated. It addresses four questions: (1) What was planned? (2) What actually happened? (3) Why was there a difference? (4) What should be done differently next time? AAR findings feed directly into updated district disaster management plans — this is how the cycle closes.
For the health sector specifically, response evaluation metrics include: time from disaster onset to establishment of medical field post; post-disaster outbreak rates (did surveillance detect outbreaks within 48 hours?); and mortality rates in the post-acute period (preventable deaths from inadequate sanitation, water, or nutrition in relief camps).
The Odisha cyclone experience is instructive. The Odisha super cyclone of 1999 killed approximately 10,000 people despite advance warning — largely because of inadequate preparedness (no cyclone shelters, no evacuation plan, no stockpiling). By contrast, when Cyclone Phailin struck the same region in 2013, a systematic preparedness programme had built hundreds of cyclone shelters and trained communities in evacuation procedures. Despite Phailin's greater intensity, fewer than 50 people died. This comparison — 10,000 vs 50 deaths from cyclones of comparable intensity — is perhaps the most powerful evidence-based argument for investing in the preparedness and mitigation phases of the cycle.
SELF-CHECK
Cyclone Phailin (2013) struck Odisha with similar intensity to the 1999 super cyclone, yet caused far fewer deaths. Which disaster management phase was MOST responsible for this difference in outcomes?
A. A. Response — NDRF deployed more rapidly in 2013
B. B. Recovery — better post-cyclone rehabilitation reduced secondary deaths
C. C. Preparedness — systematic building of cyclone shelters and evacuation drills between 1999 and 2013
D. D. Mitigation — stricter building codes prevented more housing from collapsing
Reveal Answer
Answer: C. C. Preparedness — systematic building of cyclone shelters and evacuation drills between 1999 and 2013
The dramatic reduction in cyclone mortality in Odisha between 1999 and 2013 is primarily attributed to preparedness: construction of hundreds of cyclone shelters along the coast, training of local communities in early evacuation, and establishment of early warning and communication systems. These were put in place in the years between the two cyclones — demonstrating that preparedness investment over years pays off in saved lives when the next disaster strikes.
Applying Disaster Concepts in Community Medicine Practice
The disaster management framework is not an administrative abstraction — it has direct implications for how you will practice as a community physician. Understanding your role within the DDMA machinery is essential before a disaster strikes; it cannot be figured out in the chaos of response.
At the preparedness level, the community physician contributes to: developing the health annex of the district disaster management plan (specifying which health facilities serve as casualty receiving centres, where field medical posts will be established, which community health workers will be activated); maintaining the health resource inventory (drugs, blood bank capacity, ambulances, generator backup); coordinating community health awareness — ensuring that vulnerable populations (elderly, disabled, pregnant women) are identified and included in evacuation planning; and participating in mock drills that include medical response scenarios.
At the response level, the community physician's role includes: establishing and staffing the medical field post at the disaster site or at the nearest health facility; coordinating triage using the START system (covered in the companion SDL on disaster response); managing the chain of evacuation to secondary and tertiary care; activating post-disaster disease surveillance — a critical public health function that is frequently overlooked in the pressure of acute response; and ensuring the health and safety of relief workers, who are themselves at risk from the same hazards.
At the recovery level, the physician contributes to: monitoring disease outbreaks in relief camps (a high-risk environment for cholera, hepatitis A, skin infections, respiratory illness); providing psychosocial first aid and mental health support to survivors and relief workers; and documenting health data that will feed into the after-action review and update the district plan for future events.
Park's textbook is explicit about the physician's role: the medical officer is a core member of the DDMA and is expected to have functional knowledge of the disaster management cycle, the NDMA framework, triage systems, and outbreak control in disaster settings. This is not optional knowledge — it is a defined competency under NMC 2024 guidelines (CM13.1, CM13.2, CM13.4).
A critical insight from field experience: the disaster plan that exists only on paper fails. Plans must be exercised, resources must be maintained, and personnel must be trained repeatedly. The community physician who makes time — in the pre-disaster period — to read the district disaster management plan, participate in drills, and audit resource inventories will be the most effective first-responder when the event actually occurs.
CLINICAL PEARL
The Odisha 1999 vs 2013 cyclone comparison is the most powerful evidence-based argument in disaster medicine: two cyclones of similar intensity, the same coastline, 14 years apart — 10,000 deaths vs fewer than 50. The entire difference was made in the preparedness phase: cyclone shelters built, communities trained, evacuation routes established. When questioned about cost-effectiveness of preparedness investment, cite this natural experiment. Every rupee spent on preparedness saves hundreds of rupees in response and thousands of lives. As a district physician, your investment in preparedness is not bureaucratic compliance; it is the highest-yield public health intervention available to you.