Page 4 of 11
CM13.{3,5} | CM13.{3,5} | Man-made Disasters and Simulated Response — SDL Guide
Learning Objectives
- Describe man-made disasters occurring in India and worldwide, using the CBRN classification framework
- Identify the characteristic health consequences of each category of man-made disaster with reference to Indian events
- Explain the principles of medical response in a simulated disaster environment: incident command, START triage, decontamination, and mass casualty management
- Apply START triage criteria to assign priority categories to casualties in a simulated mass casualty incident
INSTRUCTIONS
On the night of 2–3 December 1984, a pesticide factory in Bhopal released approximately 40 tonnes of methyl isocyanate gas into the densely populated surrounding neighborhoods. Within hours, thousands were dead. By conservative estimates, over 3,800 people died immediately; long-term health consequences affected over 500,000 survivors. This was not a natural disaster. It was a failure of industrial safety, emergency planning, and community preparedness. As a community physician, you may never work near a pesticide factory — but you will work near industries, conflict zones, chemical plants, or transportation corridors carrying hazardous materials. This module prepares you to understand man-made disasters and to act effectively within the medical response system when they occur.
References
- Park's Textbook of Preventive and Social Medicine, 27th Edition — Chapter on Disaster Management (textbook)
- NDMA Guidelines on Management of Chemical (Terrorism) Disasters, Government of India (policy)
- START Triage — Simple Triage And Rapid Treatment, Mass Casualty Incident Protocol, NDRF (training)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are on call at a district hospital on a Tuesday evening when the casualty officer calls: 'Sir, there has been an explosion at the fertiliser plant on the outskirts of town. We have 30 patients incoming by ambulance — burns, inhalation injuries, and several unresponsive.' Over the next 20 minutes, 47 casualties arrive simultaneously. The emergency department has 8 treatment bays. There are three doctors available, including you. Two patients are screaming; three are silent and blue; the rest are crowded at the entrance. You have 90 seconds to decide who gets care first — and in what order — before the system collapses.
This is a mass casualty incident (MCI). The principles you apply in the next 90 seconds will determine how many of these 47 people survive. This module teaches you those principles.
WHY THIS MATTERS
Man-made disasters are not rare anomalies — they are a consistent feature of industrialising economies. India's rapid industrial growth, combined with population density in urban and peri-urban areas, creates significant risk from technological accidents, chemical releases, and infrastructure failures. The Bhopal gas tragedy of 1984 remains the world's largest industrial disaster by immediate casualty count. Rail accidents, factory fires, building collapses, and chemical tanker accidents occur regularly across India. At the same time, global trends in terrorism and civil unrest mean that physicians may encounter deliberate CBRN (Chemical, Biological, Radiological, Nuclear) incidents. The simulated disaster environment competency (CM13.5) is designed specifically to give you functional response skills before you face a real event — so that your first mass casualty incident is not also your first time thinking about triage.
RECALL
From the companion SDL on disaster concepts and the management cycle, you know that man-made disasters are those arising from human activity — classified as technological/industrial, chemical, biological, radiological/nuclear, or conflict-related. You also know that the National Disaster Management Authority (NDMA) and its district-level arm (DDMA) are the statutory bodies coordinating disaster response. The NDRF (National Disaster Response Force) provides the specialised search, rescue, and first-response capability. Keep the disaster management cycle in mind: the response phase — which is the focus of this SDL — depends entirely on the preparedness investments made before the event. From your clinical modules, recall basic emergency medicine priorities: airway, breathing, circulation — these form the physiological basis of triage criteria.
Burden of Man-Made Disasters in India and Globally
Man-made disasters impose a substantial and often overlooked burden of death, disability, and environmental harm. Unlike natural disasters, which tend to receive high media and policy attention, many man-made disasters occur in industrial peripheries and affect economically marginalised communities — making their burden systematically undercounted and underaddressed.
Globally, the most significant man-made disaster categories by death toll include: industrial and technological accidents (factory explosions, mine collapses, structural failures); chemical incidents (toxic gas releases, water contamination); transportation disasters (rail, aviation, maritime); and deliberate violence (terrorism, armed conflict). The 20th century's three worst industrial disasters — Bhopal 1984 (India, methyl isocyanate, ~3,800–16,000 deaths), Chernobyl 1986 (Ukraine/Belarus, nuclear meltdown, tens of thousands of cancer deaths over decades), and Texas City 1947 (USA, ammonium nitrate explosion) — illustrate the catastrophic potential of technological failure.
In India specifically, man-made disasters include: chemical industry accidents (Bhopal being the paradigmatic case, but dozens of smaller incidents annually); coal mine disasters (Jharkhand and Chhattisgarh, periodic collapses); rail accidents (India has one of the world's largest rail networks and periodic major derailments); building collapses (often in urban areas with unregulated construction); and fire disasters in crowded markets, factories, and hospitals.
Health consequences of man-made disasters differ systematically from natural disasters: (1) the hazard agent itself causes specific toxicological or radiation injuries that require targeted treatment, not just supportive care; (2) contamination — of casualties, first-responders, and the environment — creates secondary exposure risks; (3) legal and forensic dimensions — man-made disasters often involve liability, industrial negligence, or criminal proceedings that require systematic medical documentation; and (4) long-term health sequelae — survivors of chemical or radiological disasters may develop cancers, reproductive problems, or chronic respiratory disease years or decades later, as Bhopal's survivor population demonstrated.
For the community physician, this epidemiological profile has direct implications: the public health response to man-made disasters must include surveillance for late-onset disease, environmental decontamination monitoring, and forensic medical documentation — functions that go beyond the acute response phase.
Classification and Characteristics of Man-Made Disasters
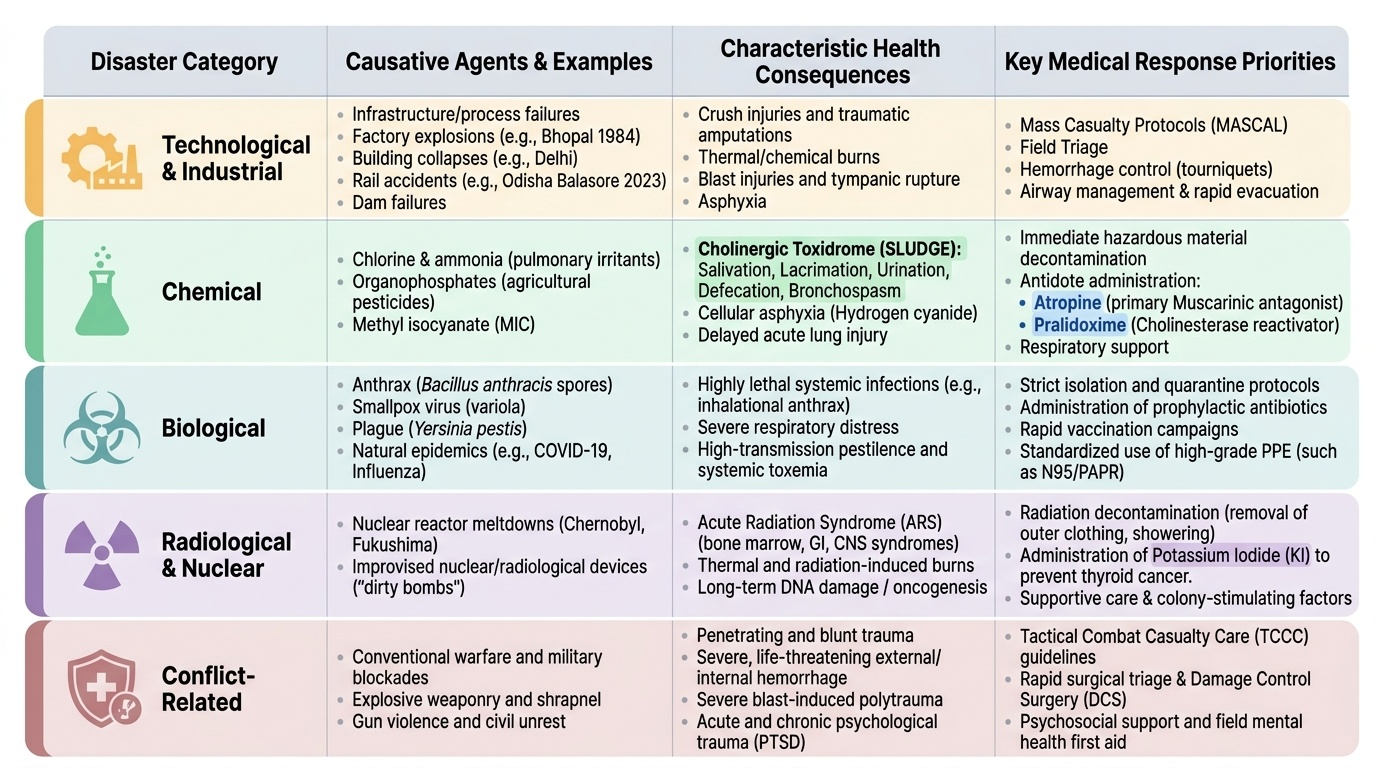
Man-made disasters are classified using the CBRN framework (Chemical, Biological, Radiological, Nuclear) for hazardous agent types, supplemented by broader categories for non-CBRN technological and conflict-related events. Understanding the category determines the response approach — each class has distinct mechanisms of injury, protective measures, and medical countermeasures.
Technological and Industrial Disasters arise from failures in industrial processes, infrastructure, or transportation. Examples: factory explosions (Bhopal 1984), building collapses (Delhi building collapses), rail accidents (Odisha Balasore rail accident 2023, 291 deaths), dam failures. Health consequences include: crush injuries, burns, blast injuries, asphyxia, and traumatic injuries. Medical response follows standard mass casualty protocols — triage, haemorrhage control, airway management, evacuation.
Chemical Disasters involve uncontrolled release of toxic chemical agents — either accidentally (industrial leak, tanker accident) or deliberately (chemical terrorism). Key toxic industrial chemicals include: chlorine (pulmonary irritant — used in Bhopal-related chlorine incidents), ammonia (pulmonary/mucosal irritant), organophosphates (cholinesterase inhibitors — agricultural pesticides), and methyl isocyanate (Bhopal agent). Health consequences are agent-specific: organophosphates cause cholinergic toxidrome (salivation, lacrimation, urination, defaecation, bronchospasm — SLUDGE); hydrogen cyanide causes cellular asphyxia; pulmonary irritants cause delayed acute lung injury. The medical countermeasure for organophosphate poisoning is atropine (muscarinic antagonist — the primary antidote) plus pralidoxime (oxime that reactivates cholinesterase if given within hours of exposure, before ageing occurs).
Biological Disasters involve release or emergence of biological agents — either natural epidemic emergence or deliberate bioterrorism. Potential bioterrorism agents include: anthrax (Bacillus anthracis — spore-forming bacteria, inhalational form most lethal), smallpox (declared eradicated but retained in two WHO-approved labs), plague (Yersinia pestis). Natural biological disasters include epidemic outbreaks (COVID-19, influenza pandemics). Medical response requires: isolation and quarantine, prophylactic antibiotics or vaccines (for bacterial agents), personal protective equipment, and coordination with public health surveillance.
Radiological and Nuclear Disasters involve uncontrolled release of ionising radiation — from nuclear plant accidents (Chernobyl 1986, Fukushima 2011), lost radioactive sources (orphan sources), dirty bombs (conventional explosive dispersing radioactive material), or nuclear weapon detonation. Health consequences depend on dose, duration, and type of radiation: acute radiation syndrome (ARS) at high doses; increased cancer risk (thyroid, leukaemia, solid tumours) at lower doses. Medical response includes: evacuation from contamination zone, thyroid-protective potassium iodide (for radioiodine exposure), decontamination of casualties, and long-term cancer surveillance.
Conflict-Related Disasters include war injuries, terrorism, civil unrest, and displacement. Health consequences: traumatic injuries (penetrating wounds, blast injuries), displacement and communicable disease in refugee settings, sexual violence, mental health sequelae.
Provided image
SELF-CHECK
A 35-year-old male worker is brought to the casualty from a pesticide factory leak. He has pinpoint pupils, profuse salivation, bronchospasm, and urinary incontinence. Which of the following is the CORRECT primary antidote?
A. A. Naloxone
B. B. Atropine
C. C. Flumazenil
D. D. Vitamin K
Reveal Answer
Answer: B. B. Atropine
This patient presents with the classic cholinergic toxidrome (SLUDGE: salivation, lacrimation, urination, defaecation, gastrointestinal cramps, emesis) plus bronchospasm and miosis — indicating organophosphate (cholinesterase inhibitor) poisoning, which is the most common chemical disaster agent in India given the agricultural context. Atropine is the primary antidote — a muscarinic antagonist that blocks the excess acetylcholine effects. Pralidoxime is the adjunctive oxime treatment (reactivates cholinesterase if given early). Naloxone reverses opioid toxicity; flumazenil reverses benzodiazepines; vitamin K reverses warfarin.
Principles of Disaster Response: Incident Command and Triage
Effective medical response to a man-made mass casualty incident requires two foundational systems to be established within the first minutes: Incident Command (who is in charge of what) and Triage (who gets care in what order). Without these two systems, even well-resourced responders produce chaotic, ineffective care.
Incident Command System (ICS) is the standardised, scalable management structure used for disaster response. The ICS establishes a clear hierarchy: at the top is the Incident Commander (IC) — a single individual with overall authority for the response. Beneath the IC are four functional sections: Operations (conducting the actual response — search, rescue, medical), Planning (situational awareness, resource tracking), Logistics (obtaining and providing resources), and Finance/Administration (costs, contracts, documentation). The medical branch operates within the Operations section. The ICS allows multiple agencies — NDRF, state police, fire service, health department, NGOs — to work under unified command with clear lines of authority and communication. In India's disaster framework, the ICS-equivalent structure is specified in NDMA guidelines and activated through the DDMA.
For the medical response team, the key ICS roles are: Medical Branch Director (coordinates all medical response at the scene), Triage Officer (leads the triage process), Treatment Area Supervisor (manages casualty collection points by colour), and Transport Officer (coordinates evacuation to hospitals). The community physician may fill any of these roles — and should know what each entails before a disaster occurs.
START Triage (Simple Triage And Rapid Treatment) is the international standard for rapid triage of multiple casualties. START allows a single responder to triage one casualty in approximately 30–60 seconds using three physiological assessments. The triage categories, signified by colour-coded tags, are:
- RED (Immediate): life-threatening injury that IS salvageable with immediate intervention. These casualties are treated first. Criteria: respiratory rate > 30/min, OR capillary refill time > 2 seconds (or radial pulse absent), OR inability to follow simple commands.
- YELLOW (Delayed): serious injury that can wait 30–60 minutes without life threat. Stable vital signs, may have fractures or significant injuries, can follow commands.
- GREEN (Minor/Walking Wounded): the walking wounded — able to walk means capable of self-evacuating. Treated last, may self-present to the treatment area.
- BLACK (Expectant/Deceased): either already dead (no pulse, no breathing after repositioning the airway) or so severely injured that survival is unlikely even with maximum resources. In a mass casualty setting, these casualties are moved aside so resources go to salvageable RED and YELLOW patients.
The START algorithm works as follows: (1) announce 'anyone who can walk, please move to the green area' — all walking-wounded self-sort to GREEN; (2) for each remaining casualty: check breathing (if absent after 30-second repositioning → BLACK); assess respiratory rate (> 30/min → RED); assess perfusion (cap refill > 2 sec or radial pulse absent → RED); assess mental status (unable to follow simple command → RED); if all three are within normal limits → YELLOW.
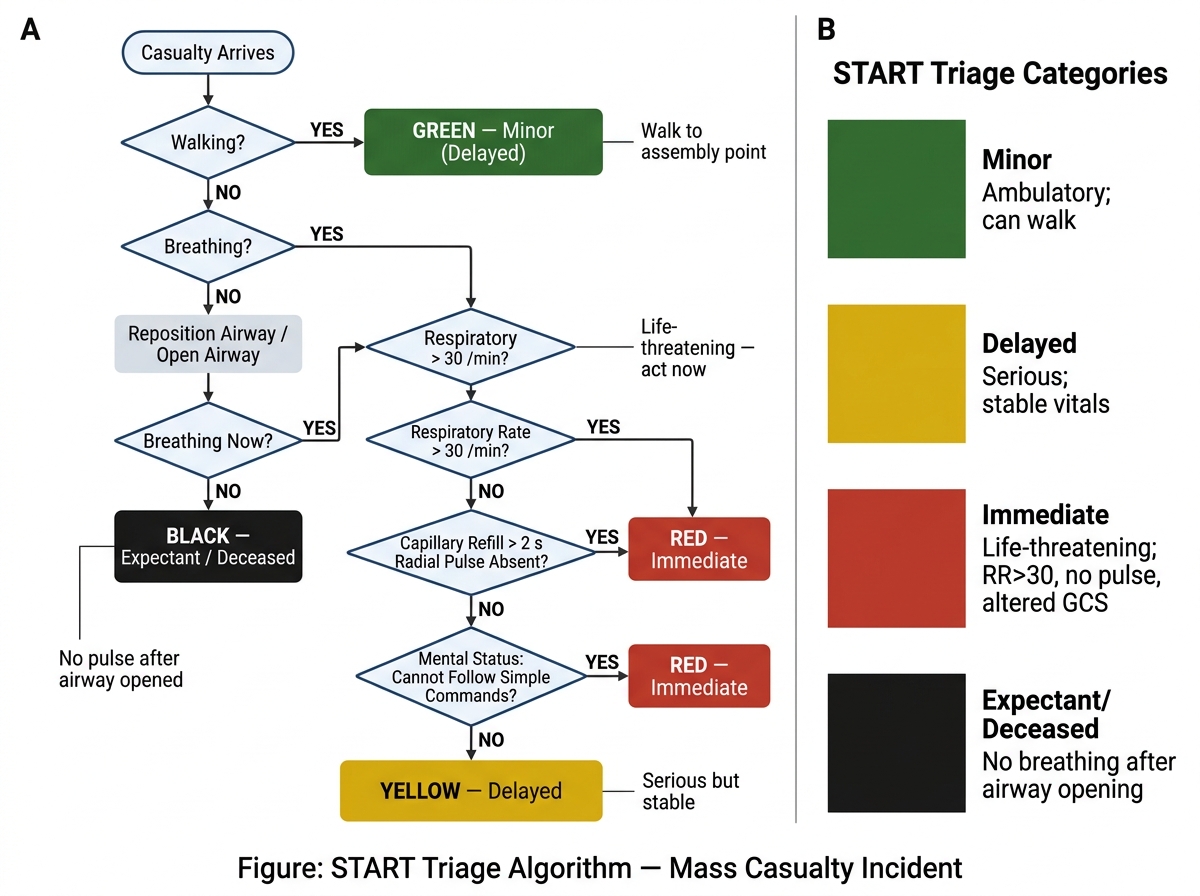
START Triage Algorithm for Mass Casualty Incident (MCI)