Page 2 of 20
CM8.1 | CM8.1 | Communicable Disease Control at Primary Care — SDL Guide (Part 2)
Evaluation and Monitoring: Surveillance and Outbreak Response
Monitoring the effectiveness of communicable disease control programmes requires a systematic disease surveillance infrastructure, and the PHC is the foundational reporting unit in India's national system.
The Integrated Disease Surveillance Programme (IDSP), launched in 2004, consolidates reporting of 33 epidemic-prone diseases through three reporting formats:
- S-form (Syndromic): weekly reporting by health workers (ASHA/ANM) of community-level syndrome clusters — fever with rash, acute diarrhoeal disease, acute respiratory illness, fever with chills — without laboratory confirmation; the 'early warning' layer
- P-form (Presumptive/Probable): weekly reporting by PHC/CHC medical officers of clinically diagnosed (but not yet laboratory-confirmed) cases
- L-form (Laboratory-confirmed): district and medical college laboratories confirm diagnoses; reported to district surveillance units
Data flows upward: Village → PHC → District Surveillance Unit (DSU) → State Surveillance Unit (SSU) → Central Surveillance Unit (IDSP headquarters, NCDC New Delhi). Each DSU has a Rapid Response Team (RRT) that investigates alerts.
An epidemic (outbreak) alert is triggered when reported cases exceed the expected baseline by twofold or more in a defined time-place cluster. Once an alert is raised, the PHC physician participates in or leads the initial outbreak investigation, following the standard outbreak investigation steps: (1) Verify the diagnosis; (2) Confirm the outbreak; (3) Define a case definition; (4) Case finding and line-listing; (5) Descriptive epidemiology (person, place, time — draw the epidemic curve); (6) Generate hypothesis about source; (7) Test hypothesis (analytical epidemiology); (8) Implement control measures; (9) Evaluate control measures; (10) Communicate findings and write report.
The epidemic curve (a histogram of case counts over time) is particularly informative: a sharp, symmetrical curve suggests a common source point outbreak; a prolonged or multi-modal curve suggests a propagated outbreak (person-to-person spread). Recognising the curve shape guides immediate control (e.g., removing the contaminated food source vs. isolating infectious cases).
Compulsory notification of epidemic-prone diseases (cholera, plague, yellow fever, smallpox/monkeypox) is mandated under the Epidemic Diseases Act 1897 (amended 2020). TB notification on NIKSHAY is compulsory for all providers under the Revised Schedule of the TB Notification policy.
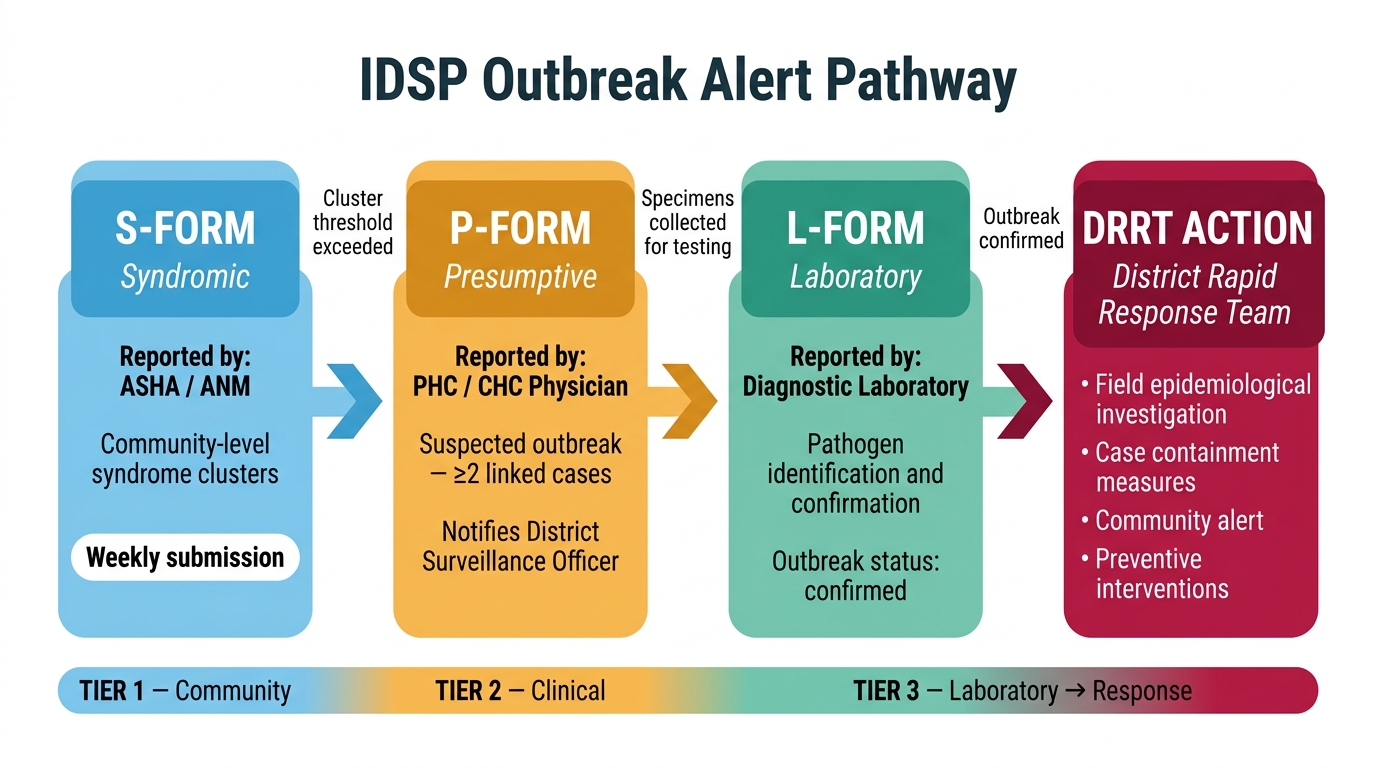
IDSP Outbreak Alert Escalation Pathway: S-form → P-form → L-form → DRRT Action
SELF-CHECK
During an IDSP surveillance cycle, which reporting format is submitted by ASHA/ANM workers based on community-level syndromes WITHOUT laboratory confirmation?
A. L-form
B. P-form
C. S-form
D. R-form
Reveal Answer
Answer: C. S-form
The S-form (Syndromic form) is submitted weekly by community-level health workers (ASHA, ANM) based on observed syndrome clusters. The P-form (Presumptive) is filled by PHC/CHC doctors, and the L-form (Laboratory) by diagnostic laboratories. Together they form IDSP's three-tier early warning system.
CLINICAL PEARL
The first 48 hours matter most. When you suspect a cluster of similar illnesses — two or more patients from the same village, school, or household presenting within a week with the same syndrome — do not wait for laboratory results before acting. File an S-form/P-form immediately, define a preliminary case definition, alert the District Surveillance Officer, and begin case-finding in the community. In cholera, typhoid, or influenza outbreaks, a 48-hour delay in reporting can mean hundreds more exposures. The IDSP exists precisely to be activated on clinical suspicion, not laboratory certainty.
The Primary Care Physician's Role: Detection to Referral
The primary care physician's responsibilities in communicable disease control extend well beyond writing a prescription. They span the full epidemiological cycle from early detection to community protection.
Case detection and diagnosis: Maintain clinical vigilance for syndrome clusters. Use PHC-level laboratory tests appropriately — sputum smear + CBNAAT for TB suspects, RDT for febrile patients in malaria-endemic areas, NS1 antigen for dengue suspects in the first five days. Know which tests are available at your PHC, which require referral to the district laboratory, and what the turnaround time is.
Notification and reporting: Register all suspected and confirmed TB cases on NIKSHAY. Report disease syndromes and confirmed cases through IDSP's S/P/L forms as appropriate. Know the list of notifiable diseases in your state (which extends the national list). Failure to notify is not merely a bureaucratic omission — it prevents the public health response from being triggered.
Treatment initiation and adherence support: Start DOTS for TB patients directly — do not wait for specialist review. Administer ACT (artemisinin combination therapy) for P. falciparum malaria and chloroquine/primaquine for P. vivax per NVBDCP guidelines. Ensure MDT is dispensed and blister packs are recorded for NLEP patients. Involve ASHA workers in adherence support.
Contact tracing and screening: Examine household and close contacts of index TB cases; offer preventive therapy (isoniazid preventive therapy, IPT) to eligible contacts. Identify and eliminate dengue and malaria vector breeding sites near index cases. Refer contacts for HIV testing after counselling when an index HIV case is identified.
Community health education: Conduct monthly village health sanitation and nutrition days (VHSNDs) to deliver immunization, health promotion, and vector control messages. Train ASHAs and ANMs in early symptom recognition and referral for priority communicable diseases.
Referral criteria: Refer when: suspected drug-resistant TB (CBNAAT detects rifampicin resistance → refer to DR-TB centre); severe malaria (altered consciousness, respiratory distress, haemoglobin <5 g/dL → refer to FRU/district hospital); complicated dengue (dengue with warning signs — persistent vomiting, haematocrit rise >20%, platelet <100,000/µL → refer immediately); HIV with AIDS-defining illness → refer to ART centre.
The PHC physician who integrates clinical acumen with public health action — notifying, tracing, educating, referring, and reporting — is the cornerstone of India's communicable disease control architecture.