Page 10 of 20
CM8.4-5 | CM8.4-5 | Epidemic Control Planning — SDL Guide
Learning Objectives
- Define epidemic, pandemic, and cluster; distinguish common source from propagated outbreaks using epidemic curve shape
- Explain R0, herd immunity threshold, and the conditions that enable epidemic occurrence
- Describe the 10-step outbreak investigation process and the principles of source control, host protection, and transmission interruption
- Calculate and interpret attack rate, secondary attack rate, and case fatality rate; evaluate epidemic control measure effectiveness
- Define the PHC physician's specific responsibilities in outbreak detection, notification, investigation, and community epidemic response
INSTRUCTIONS
Every PHC physician will, at some point in their career, face an epidemic — possibly many. Whether it is a village cluster of cholera cases, a measles outbreak in a school, or a dengue surge in the monsoon season, the response in the first 48 hours is determined almost entirely by what the primary care physician knows and does. This module equips you with the epidemiological tools, the 10-step investigation framework, and the community-level control principles that turn a potential outbreak into a contained, documented, and understood event.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 4 (Epidemiology) — Epidemic Investigation (textbook)
- Gordis Epidemiology, 5th ed., Ch. 3 — Disease Outbreaks and Surveillance (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
On a Thursday morning in August, three children from the same village school present to the PHC with acute watery diarrhoea and vomiting. By Friday afternoon, there are eleven cases — two adults, nine children — all from the same hamlet. The school mid-day meal was served from a shared pot. Six of the eleven cases attended the same meal session on Wednesday. The medical officer has 30 minutes before the District Surveillance Officer calls for a situation report. What does she know, what does she need to find out, and what must she do right now?
WHY THIS MATTERS
Epidemics cause three types of harm that make them qualitatively different from individual clinical cases: (1) they concentrate morbidity and mortality in a short time window, overwhelming health facility capacity; (2) they generate community panic disproportionate to the actual case count, disrupting social and economic function; and (3) they are preventable — a well-managed outbreak investigation can identify the source, implement control, and halt transmission within days, preventing hundreds or thousands of additional cases. The PHC physician who understands epidemic epidemiology can save more lives in two weeks of an outbreak response than in months of routine clinical care. This is one of the highest-impact competencies in community medicine.
RECALL
From your earlier studies, recall:
- Epidemic curve types: a single sharp peak suggests a common-source point outbreak; a prolonged multi-modal curve suggests person-to-person (propagated) spread.
- IDSP alert pathway: S-form → P-form → L-form → District Rapid Response Team.
- Modes of transmission: direct contact, droplet, airborne, faeco-oral, vector-borne, parenteral — the mode shapes which control measure is most effective.
- Primary vs secondary prevention: primary stops exposure; secondary detects and treats early.
This SDL applies these foundations to the structured, systematic process of outbreak investigation and epidemic control.
Epidemics: Public Health Importance and Types
An epidemic is defined as the occurrence of cases of a disease in a community or region in numbers clearly exceeding the expected level based on past experience. The word 'clearly' is operationally important — it distinguishes statistical excess from normal case-to-case variation. In practice, IDSP triggers an outbreak alert when reported cases exceed the expected baseline by twofold or more, or when two or more epidemiologically linked cases of a rare disease (e.g. cholera, plague) appear in the same time-place cluster. A pandemic is an epidemic affecting multiple countries or continents simultaneously. An endemic disease is one present at a constant, predictable background level in the population. A cluster is a grouping of cases in time and place, possibly an early epidemic.
Types of epidemics by source:
Common-source outbreaks occur when all cases share a single exposure source — a contaminated water supply, a food item served at a gathering, a shared environmental exposure. The defining features are: (a) the epidemic curve shows a sharp, symmetrical single peak; (b) onset times cluster within one incubation period of the common exposure (this allows back-calculation of the probable exposure time); (c) no subsequent generations of cases appear if the source is removed. A wedding feast where the biryani was contaminated with S. aureus toxin causing gastroenteritis within 2–6 hours of the meal is the archetype.
Propagated outbreaks (person-to-person spread) show a characteristically different pattern: the epidemic curve rises gradually, with multiple modal peaks, each separated by approximately one incubation period of the pathogen. Each peak represents a new wave of secondary, tertiary, and subsequent generation cases. Measles in an unimmunized school, influenza in a hostel, and COVID-19 in a housing colony are propagated outbreaks. Control requires interrupting person-to-person transmission rather than removing a single point source.
Mixed outbreaks combine both patterns — an initial common-source exposure followed by secondary person-to-person spread (e.g. cholera from contaminated water followed by faeco-oral household spread).
The public health importance of epidemics is measured not just by case count but by: attack rate (how many of the exposed are affected), case fatality rate (how lethal is the pathogen in this outbreak), secondary attack rate (how efficiently is it spreading from case to contact), and the capacity of the local health system to absorb the case surge.
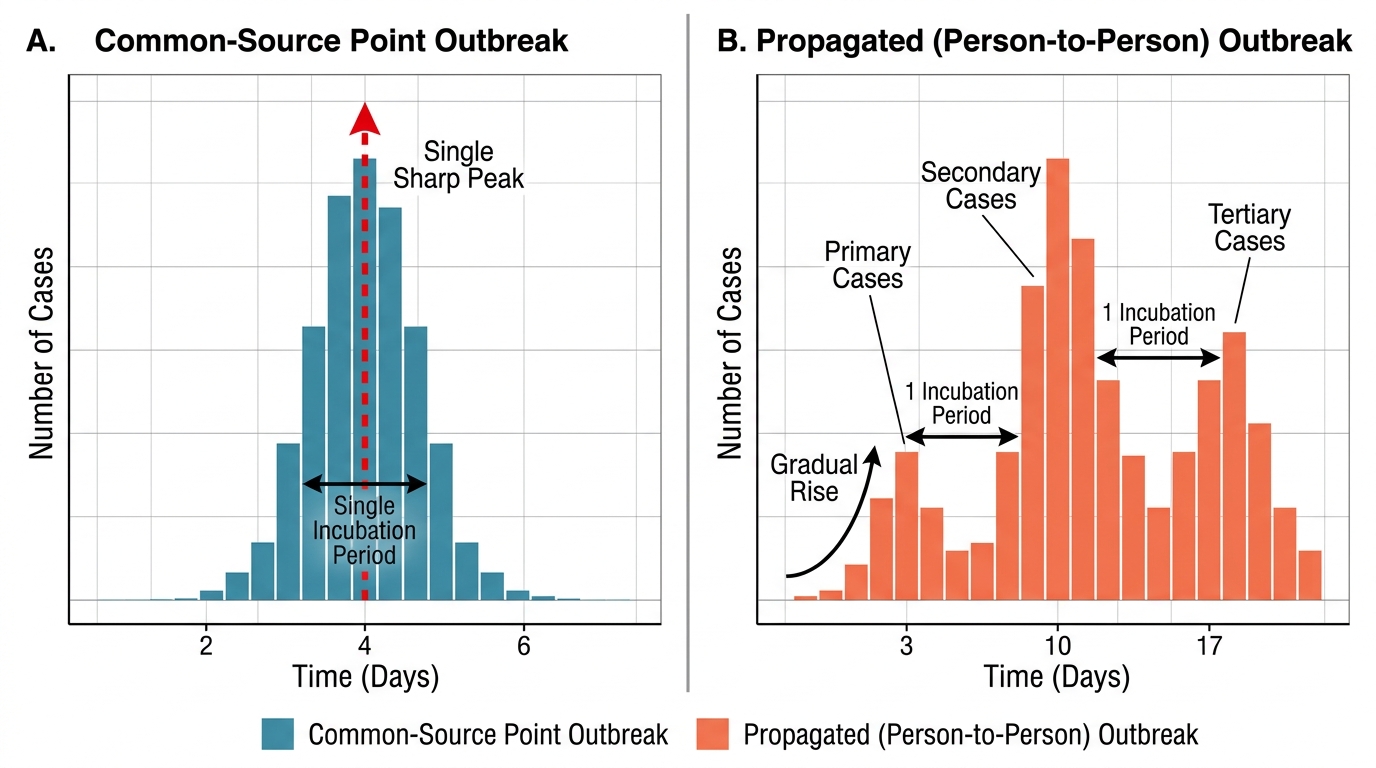
Epidemic Curve Patterns: Common-Source vs. Propagated Outbreak
SELF-CHECK
A gastrointestinal illness outbreak occurs after a school prize distribution ceremony. All 47 ill students ate the catered lunch. The onset times cluster between 2 and 8 hours after the meal, forming a sharp single peak on the epidemic curve. What type of outbreak does this most likely represent?
A. Propagated outbreak from person-to-person spread
B. Common-source point outbreak from a single contaminated food item
C. Mixed outbreak with both common source and propagated transmission
D. Endemic disease with a chance clustering
Reveal Answer
Answer: B. Common-source point outbreak from a single contaminated food item
A sharp, single-peaked epidemic curve with all cases clustered within one incubation period of a shared exposure (the catered lunch) is the hallmark of a common-source point outbreak. The 2–8 hour incubation period for toxin-mediated GI illness (Staphylococcal toxin or Bacillus cereus) is consistent. No subsequent cases beyond the lunch attendees would be expected if the source is removed.
Determinants of Epidemic Occurrence and Spread
Epidemics do not occur spontaneously — they arise when specific epidemiological conditions align. Understanding these determinants allows anticipation of which communities and contexts are at highest risk.
The basic reproduction number (R0) is the single most important epidemiological parameter characterising an epidemic's potential. R0 is defined as the average number of secondary cases generated by one infectious case in a fully susceptible population. An R0 > 1 means each case, on average, infects more than one other person — the epidemic grows exponentially. R0 < 1 means the epidemic is self-limiting and will die out. R0 = 1 is the unstable equilibrium. The effective reproduction number (Re or Rt) accounts for pre-existing immunity and control measures; Re < 1 is the target of all epidemic control programmes. Measles has an R0 of 12–18 (extremely high transmissibility); SARS-CoV-2 original strain had R0 ≈ 2–3; seasonal influenza R0 ≈ 1.2–1.4.
Herd immunity is the indirect protection of susceptible individuals that results from a sufficiently high proportion of immune persons in the population breaking transmission chains. The herd immunity threshold (HIT) is calculated as: HIT = 1 − (1/R0). For measles (R0 ≈ 15): HIT = 1 − 1/15 = 93.3% — meaning 93.3% of the population must be immune (through vaccination or prior infection) to prevent epidemic spread. For polio (R0 ≈ 5): HIT ≈ 80%. This is why measles vaccination coverage must exceed 95% (MCV2 target under UIP) to prevent outbreaks — even a 5% immunity gap allows epidemics.
Conditions enabling epidemic occurrence:
1. Accumulation of susceptibles: waning vaccination coverage, large unimmunized birth cohort, or incoming migrant population without prior immunity
2. Introduction of a new pathogen or a variant with higher transmissibility or immune escape (e.g. emergence of a new influenza strain, new SARS-CoV-2 variant)
3. Environmental/ecological change: flooding (increases vector breeding, faecal contamination of water), drought (population crowding at water sources), deforestation (zoonotic spillover)
4. Breakdown of surveillance and response: delayed detection means more exposures before control; overwhelmed health systems cannot investigate and contain
5. Social determinants: crowding, poor sanitation, low health literacy, and mistrust of health services all amplify epidemic spread
Understanding which of these determinants is operating in a specific outbreak guides the choice of control measure — you cannot vaccinate against a food-contamination outbreak, and you cannot improve water quality to control measles.
Principles of Epidemic Control and Outbreak Investigation
The systematic response to any epidemic follows a structured 10-step outbreak investigation framework, internationally standardised and used by all public health agencies. The steps are interdependent — early steps inform later ones — but control measures should be implemented as soon as there is reasonable evidence, even before the investigation is complete (outbreak investigation and control proceed in parallel).
The 10 steps of outbreak investigation:
- Verify the diagnosis — confirm that cases have the suspected disease through clinical review, laboratory testing (collect samples before starting treatment where possible), and review of existing data
- Confirm the outbreak — compare current case counts with expected baseline (IDSP historical data); confirm that the excess is real and not an artefact of changed reporting
- Define a case definition — a standardised clinical (and/or laboratory) description of what counts as a case; enables consistent case-finding. Includes: person (age, sex, occupation), place (village, ward, institution), time (onset date range). Use a working case definition initially (sensitive); tighten it as evidence accumulates
- Case finding and line-listing — active search for cases in the affected community; create a line list (one row per case: age, sex, onset date, symptoms, exposure history, address, outcome)
- Descriptive epidemiology — analyse by person (who is affected — age, sex, occupation, risk behaviour), place (map cases — spatial clustering reveals source), and time (draw the epidemic curve — reveals outbreak type and likely exposure timing)
- Generate hypotheses — based on the descriptive epidemiology, generate testable hypotheses about the source, mode of transmission, and causative agent
- Test hypotheses analytically — case-control study (compare cases vs controls on exposures) or cohort study (compare attack rates between exposed and unexposed) to identify the specific source
- Implement control measures — target the most likely source and mode of transmission; do not wait for complete epidemiological certainty
- Evaluate control measures — monitor the epidemic curve; a declining attack rate and no new cases after the incubation period confirm effective control
- Communicate findings — write an outbreak report; present to district authorities, IDSP, and affected community; update surveillance protocols
Principles of epidemic control measures target all three components of the chain of infection:
- Source control: remove or neutralise the pathogen source (ban the contaminated food, treat the water supply, isolate and treat infectious cases)
- Host protection: vaccination (when available and appropriate), chemoprophylaxis (e.g. doxycycline for cholera contacts, oseltamivir for influenza close contacts), nutritional supplementation to reduce susceptibility
- Interrupt transmission: barrier measures (hand hygiene, masks for droplet/airborne diseases), safe water and sanitation (for faeco-oral), vector control (for vector-borne), contact tracing and quarantine
Legal framework: The Epidemic Diseases Act 1897 (amended 2020) empowers state governments to declare an epidemic and take special measures including: inspecting vessels and individuals, detaining contacts, regulating gatherings, and mandating isolation. The 2020 amendment extended powers to the Central Government during public health emergencies and added provisions protecting healthcare workers from violence.
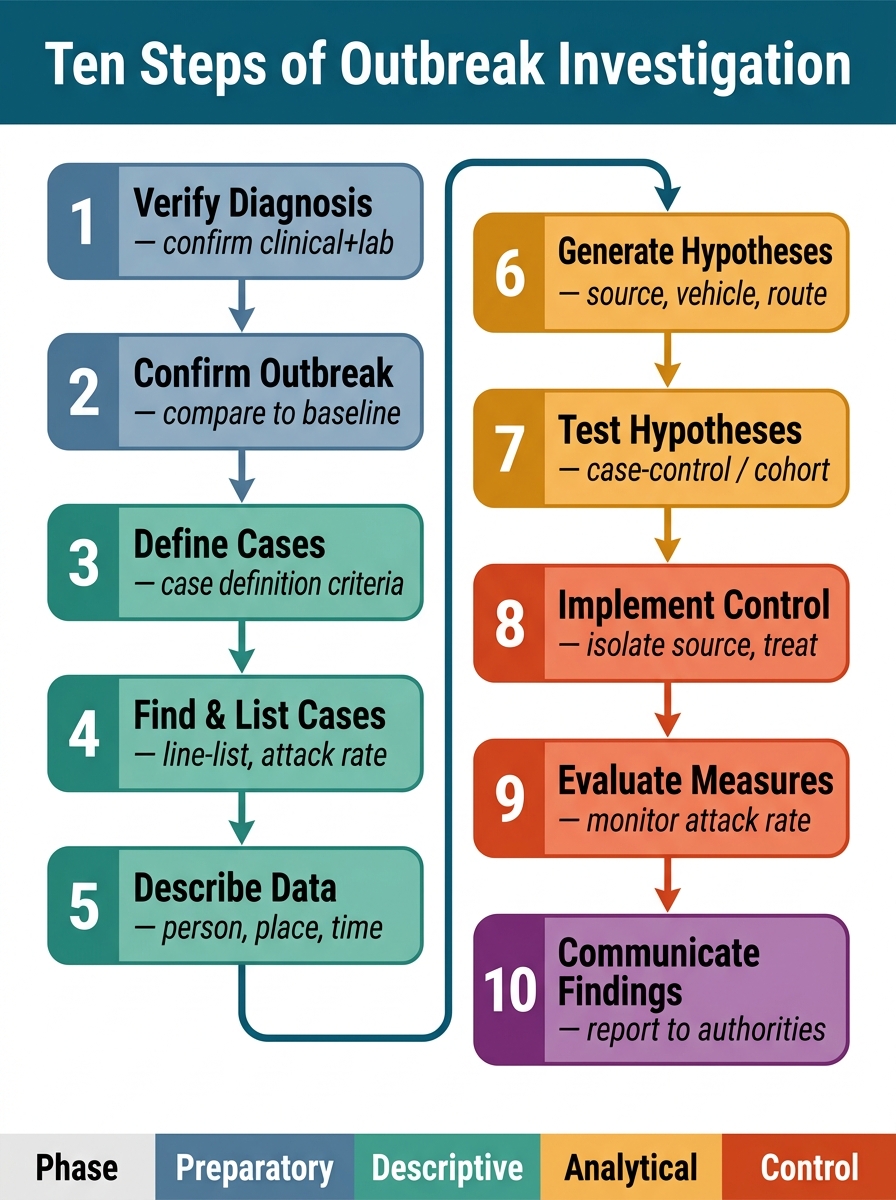
Figure: Ten-Step Outbreak Investigation Framework
SELF-CHECK
During an outbreak investigation, the medical officer notices that cases are clustered in households sharing a common borewell. This finding most directly informs which step of the outbreak investigation?
A. Step 2: Confirm the outbreak
B. Step 4: Case finding and line-listing
C. Step 6: Generate hypotheses
D. Step 8: Implement control measures
Reveal Answer
Answer: C. Step 6: Generate hypotheses
Spatial clustering of cases around a common borewell is a finding from descriptive epidemiology (Step 5) that directly generates a testable hypothesis (Step 6) — specifically that the borewell is the contaminated water source. The hypothesis would then be tested analytically (Step 7) by comparing attack rates between households using the borewell versus those not using it. Control measures (Step 8) — closing the borewell, chlorinating the water — would follow hypothesis testing or be implemented in parallel if the evidence is compelling.