Page 13 of 20
CM8.6-7 | CM8.6-7 | Surveillance Training and Information Systems — SDL Guide
Learning Objectives
- Quantify the cost of inadequate disease surveillance and explain the 'intelligence gap' it creates in public health
- Identify the determinants of surveillance failure including underreporting, health worker knowledge gaps, and data quality issues
- Describe how a PHC physician trains ASHA workers and ANMs in syndrome recognition, reporting, sample collection, and health education
- Explain the health information system cycle and the role of key national platforms (HMIS, IDSP, NIKSHAY, NPCDCS MIS)
- Apply surveillance data at the PHC level to detect outbreak early warning signals and guide programme decisions
INSTRUCTIONS
Public health is only as strong as its information. A disease that goes unreported cannot be controlled; a programme whose data are inaccurate cannot be evaluated; a community that does not know what symptoms to report cannot participate in surveillance. This module focuses on the intelligence infrastructure of public health — disease surveillance and health information systems — and on your practical role in training the community health workers who are your data collectors, first reporters, and health educators.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 2 (Epidemiology) — Disease Surveillance and Health Information (textbook)
- WHO: Disease Surveillance Standards and International Health Regulations 2005 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2006, the Indian state of Uttarakhand experienced a large cholera outbreak that killed dozens of people. Post-outbreak analysis revealed that the ASHA workers in affected villages had seen diarrhoeal clusters for nearly two weeks before a formal alert was filed — they did not know which syndromic symptoms required immediate reporting, and the weekly S-form had not been taught in their last refresher training. Two weeks of avoidable exposure, hundreds of additional cases, dozens of preventable deaths — the gap was not in treatment; it was in the intelligence that should have triggered the response. This is the cost of poor surveillance.
WHY THIS MATTERS
The ability to detect disease early — before it becomes an epidemic — depends entirely on the quality of information flowing from communities and health facilities to decision-makers. India's disease burden estimates for most conditions rely on modelling and household surveys precisely because routine surveillance under-captures the true incidence. This 'intelligence gap' means that national programmes are often underfunded for the diseases that actually matter most locally, and outbreaks are detected late. As a PHC physician, you control two critical input nodes in this information chain: you train the ASHA workers who are the first reporters at community level, and you manage the PHC's data entry into the national health information systems. The quality of India's public health intelligence depends, in no small measure, on the competence and commitment you bring to these tasks.
RECALL
From earlier in this cluster, recall:
- IDSP S/P/L forms: S-form (syndromic, community health workers), P-form (presumptive, PHC/CHC doctors), L-form (laboratory-confirmed).
- Programme-specific information systems: NIKSHAY (NTEP/TB), HMIS (aggregate programme data), NPCDCS MIS, NVBDCP MIS.
- ASHA worker roles: first-contact health worker for communities; primary interface for maternal-child health tracking, immunization defaulter follow-up, and disease recognition.
- Epidemic alert trigger: 2× expected cases, or cluster of ≥2 linked rare disease cases → triggers IDSP P-form and DSU alert.
This SDL focuses specifically on the information infrastructure and training responsibilities that make these systems work.
The Intelligence Gap: Why Surveillance Matters
Disease surveillance is defined by the WHO as the ongoing systematic collection, analysis, and interpretation of outcome-specific data, essential to the planning, implementation, and evaluation of public health practice. The key word is 'ongoing' — surveillance is not a one-time study but a continuous, real-time monitoring system that converts raw case data into public health intelligence.
The scale of India's surveillance intelligence gap is substantial. Studies comparing IDSP-reported cases to household survey estimates consistently show that routine surveillance captures only 5–15% of the true incidence for conditions like acute diarrhoeal disease and acute respiratory infection. For tuberculosis, NIKSHAY registration substantially improved with mandatory notification, but private-sector cases (which represent approximately 50% of the TB burden) remain under-notified despite legal requirements. For dengue, official case counts are estimated to represent less than 10% of actual infections.
This under-capture has real consequences:
1. Delayed outbreak detection — when baseline case counts are artificially low, the threshold for an 'epidemic alert' (2× expected) is never crossed even as actual cases surge
2. Resource misallocation — districts with high under-reporting appear to have low disease burden and receive less programme funding; the true high-burden areas are underfunded
3. Programme evaluation distortion — when a programme appears to be reducing cases but actual incidence is unchanged, the reason may be worsening surveillance rather than genuine control
The 2004 launch of IDSP was designed specifically to address this gap by creating a dedicated, real-time disease intelligence system covering epidemic-prone and selected non-epidemic diseases, linking community health workers, PHCs, and district/state/national surveillance units through a structured reporting hierarchy.
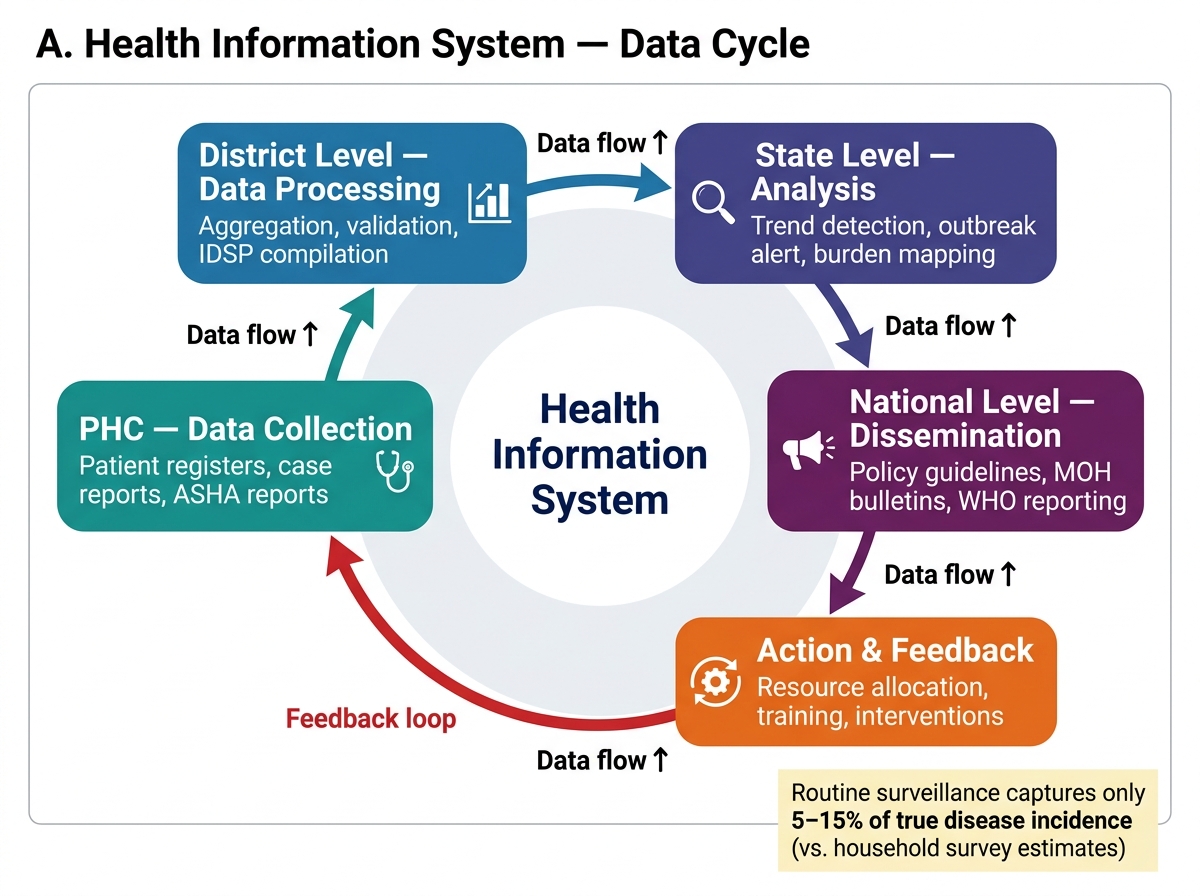
Health Information System Cycle — PHC to National Level
SELF-CHECK
Studies comparing IDSP surveillance data to household survey estimates suggest that routine reporting captures approximately what proportion of true incidence for acute diarrhoeal disease in India?
A. 5–15%
B. 30–40%
C. 50–60%
D. 80–90%
Reveal Answer
Answer: A. 5–15%
Routine surveillance systems in India capture only 5–15% of the true incidence of conditions like acute diarrhoeal disease, based on comparisons with household survey estimates. This major intelligence gap explains why outbreaks can be large before detection and why programme resources are frequently misallocated to apparently low-burden areas that are actually high-burden but under-reporting.
Determinants of Surveillance Quality and Failure
Understanding why surveillance fails is the first step toward designing interventions that improve it. The determinants of surveillance failure operate at multiple levels simultaneously.
Health worker knowledge gaps are the most modifiable determinant. An ASHA who does not know which syndromes require immediate reporting (acute flaccid paralysis, sudden unexplained deaths, large diarrhoeal clusters) cannot initiate the reporting chain. An ANM who does not know the case definition for cholera (three or more watery stools in 24 hours) cannot distinguish it from ordinary diarrhoea. A PHC doctor who does not know the IDSP P-form format will delay submission or submit incomplete data.
Underreporting arises from several distinct causes:
- Stigma: patients with HIV, leprosy, and mental health conditions may conceal symptoms or avoid formal care to avoid discrimination; health workers may not report to protect patient confidentiality
- Fear of consequences: a local elected official may pressure a PHC to suppress cholera or typhoid data to protect tourism or commercial interests; a health worker may under-report to avoid blame for an outbreak
- Pathway interruption: patients with mild illness never reach the formal health system; they are treated by informal providers (RMPs, chemists) who have no surveillance reporting obligation and typically do not report
- Private sector gap: approximately 70% of India's first-contact care is delivered by private providers; mandatory TB notification has improved but broader private-sector surveillance coverage remains minimal
Infrastructure and process limitations:
- Irregular internet connectivity in rural PHCs makes real-time HMIS/NIKSHAY data entry difficult
- High staff turnover means trained staff leave and replacements receive no IDSP training
- Paper forms are completed but not entered into electronic systems, creating a 'paper pile' that is weeks behind real time
- Absence of feedback to reporting units (PHCs receive no response to their S/P/L forms) removes the motivation to submit accurate, timely data
Data quality problems include: incorrect dates (date of report substituted for date of onset), miscoded diagnoses (ICD coding errors), incomplete demographic information, and duplicate reporting (the same case reported from PHC and from hospital).
Training Health Workers in Surveillance and Health Education
The PHC physician is not merely a user of surveillance data — she is the trainer and supervisor of the community health workers who generate the first layer of surveillance data. Under the National Health Mission (NHM), the PHC medical officer is responsible for: (a) regular ASHA refresher training; (b) ANM mentoring during monthly ASHA review meetings; and (c) sub-centre supervisory visits.
Core surveillance training content for ASHA workers:
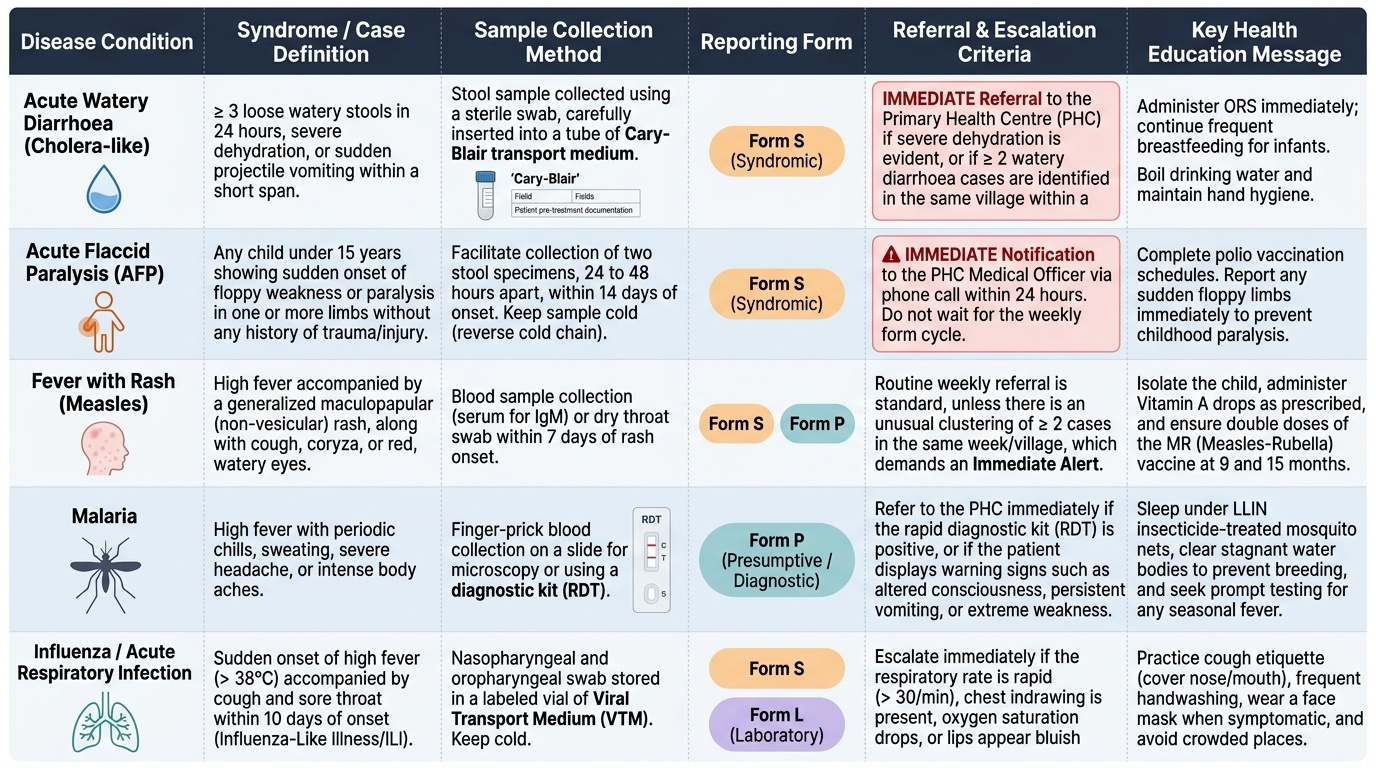
- Syndrome recognition: ASHA workers must be trained to recognise key epidemic-prone syndromes that require immediate PHC notification rather than routine weekly reporting: acute watery diarrhoea (particularly with vomiting — cholera-like), acute flaccid paralysis (AFP — any child under 15 with sudden onset weakness), unusual clustering of fever with rash (measles), and any sudden unexplained deaths (≥2 in same village in same week)
- Reporting pathway: practice completing the S-form correctly — including dates, number of cases, age-sex distribution, and locating all cases on the village map. Reinforce the reporting timeline (weekly by Monday) and the emergency escalation path (call PHC MO immediately for clusters of AFP, cholera, or unexplained deaths — do not wait for the weekly form)
- Sample collection: demonstrate proper stool sample collection for diarrhoea (Cary-Blair transport medium; label with patient name, village, date, clinical diagnosis); blood sample collection for malaria RDT; respiratory samples for influenza surveillance. Emphasise pre-treatment collection — samples taken after antibiotics have started have drastically lower diagnostic yield
- Referral criteria: clearly define which cases require immediate referral to PHC or FRU — not every case needs referral, but ASHA workers must know the red flag signs: altered consciousness, severe dehydration (sunken eyes, skin pinch test), inability to drink, respiratory distress
- Health education skills: teach ASHA workers to conduct structured IEC (Information, Education, Communication) sessions in the community. Key IEC principles: use local language; tailor the message to literacy level (use pictures and demonstrations, not only text); focus on behaviour change (hand washing, boiling water, using ORS, seeking care early), not disease information alone; address the specific misconceptions prevalent in the local community
Provided image
SELF-CHECK
An ASHA worker finds three children in a village with sudden onset of weakness in one leg, occurring within a two-day period. What is the CORRECT action for the ASHA?
A. Complete the weekly S-form at the end of the week
B. Refer the children to the ANM at the next sub-centre session
C. Immediately call the PHC medical officer and report — this is a suspected AFP cluster requiring urgent notification
D. Administer ORS and monitor for 48 hours before reporting
Reveal Answer
Answer: C. Immediately call the PHC medical officer and report — this is a suspected AFP cluster requiring urgent notification
Acute flaccid paralysis (AFP) — sudden onset limb weakness in a child under 15 — is a polio-alert condition under the National Polio Surveillance Programme. Any AFP case (even a single case) requires immediate notification to the District Surveillance Officer within 24 hours, and investigation within 2 days. A cluster of three cases is an emergency requiring immediate PHC medical officer notification — not a weekly S-form. The 60-day stool sample deadline for polio surveillance requires immediate action, not delayed reporting.