Page 2 of 19
CM3.1 | CM3.1 | Environmental Pollution Hazards — SDL Guide (Part 2)
Water Pollution and Chemical Hazards
Water pollution is classified by the type of contaminant: biological (bacteria, viruses, protozoa, helminths), chemical (heavy metals, pesticides, nitrates, industrial effluents), and radiological (uranium, radon in groundwater). While biological contamination and waterborne disease are covered in detail in CM3.2/CM3.3, chemical water pollutants deserve attention here as distinct environmental health hazards with chronic health consequences.
Arsenic contamination of groundwater—endemic in parts of West Bengal, Bihar, Jharkhand, and Assam—is a major Indian public health crisis. Chronic arsenic ingestion causes characteristic effects: Mees' lines on nails, arsenical keratoses on palms and soles, skin hyperpigmentation and depigmentation ('raindrop' pattern), peripheral neuropathy, and an elevated risk of bladder, lung, and skin cancers. The WHO and BIS guideline for arsenic in drinking water is ≤10 µg/L; India's provisional standard is 50 µg/L for areas where safer sources are unavailable.
Fluoride in groundwater is a dual hazard: at 0.5-0.8 mg/L it prevents dental caries; above 1.5 mg/L (WHO) it causes dental fluorosis (mottled enamel); above 4 mg/L, skeletal fluorosis (osteosclerosis, kyphosis, crippling). Endemic fluorosis affects 17 Indian states (BIS acceptable limit 1.0 mg/L, permissible limit 1.5 mg/L).
Nitrate in well water (from agricultural run-off) causes methaemoglobinaemia in infants (<6 months old) via bacterial gut conversion of nitrate to nitrite, which oxidises haemoglobin's Fe2+ to Fe3+ (methaemoglobin cannot carry oxygen). This is the 'blue baby syndrome.' The WHO/BIS standard for nitrate in drinking water is ≤45 mg/L (as NO3-).
Pesticides (organochlorines, organophosphates) in water sources cause long-range environmental contamination through bioaccumulation up the food chain (biomagnification)—a concept illustrated by DDT, where concentrations 10,000,000-fold higher than ambient water were detected in top-of-chain birds.
SELF-CHECK
A city's air quality monitoring shows PM2.5 at 95 µg/m³ (24-hour average). India's NAAQS 24-hour PM2.5 standard is 60 µg/m³. A radiologist working in a nuclear medicine department asks whether this air quality reading is also relevant to her radiation exposure. Which statement is MOST accurate?
A. PM2.5 at 95 µg/m³ is safe because it is below the WHO 2021 guideline of 15 µg/m³
B. PM2.5 is a non-ionising environmental pollutant, whereas her occupational radiation is ionising—these are separate categories of hazard, but the outdoor air reading IS above India NAAQS
C. PM2.5 causes radiation sickness if inhaled in sufficient quantity
D. Non-ionising radiation from PM2.5 and the ionising radiation she works with both require the same regulatory body (AERB) for safety oversight
Reveal Answer
Answer: B. PM2.5 is a non-ionising environmental pollutant, whereas her occupational radiation is ionising—these are separate categories of hazard, but the outdoor air reading IS above India NAAQS
PM2.5 at 95 µg/m³ exceeds the India NAAQS 24-hour limit of 60 µg/m³ (not the WHO guideline value which is 15 µg/m³—a common confusion). Particulate matter and ionising radiation are entirely distinct hazard categories: PM2.5 causes respiratory/cardiovascular harm through inflammation and systemic uptake, while ionising radiation causes DNA damage. They are regulated by different bodies (CPCB for air quality; AERB for radiation). The comparison tests whether students can correctly classify hazard categories and recall the correct Indian standard.
National Standards and Regulatory Framework
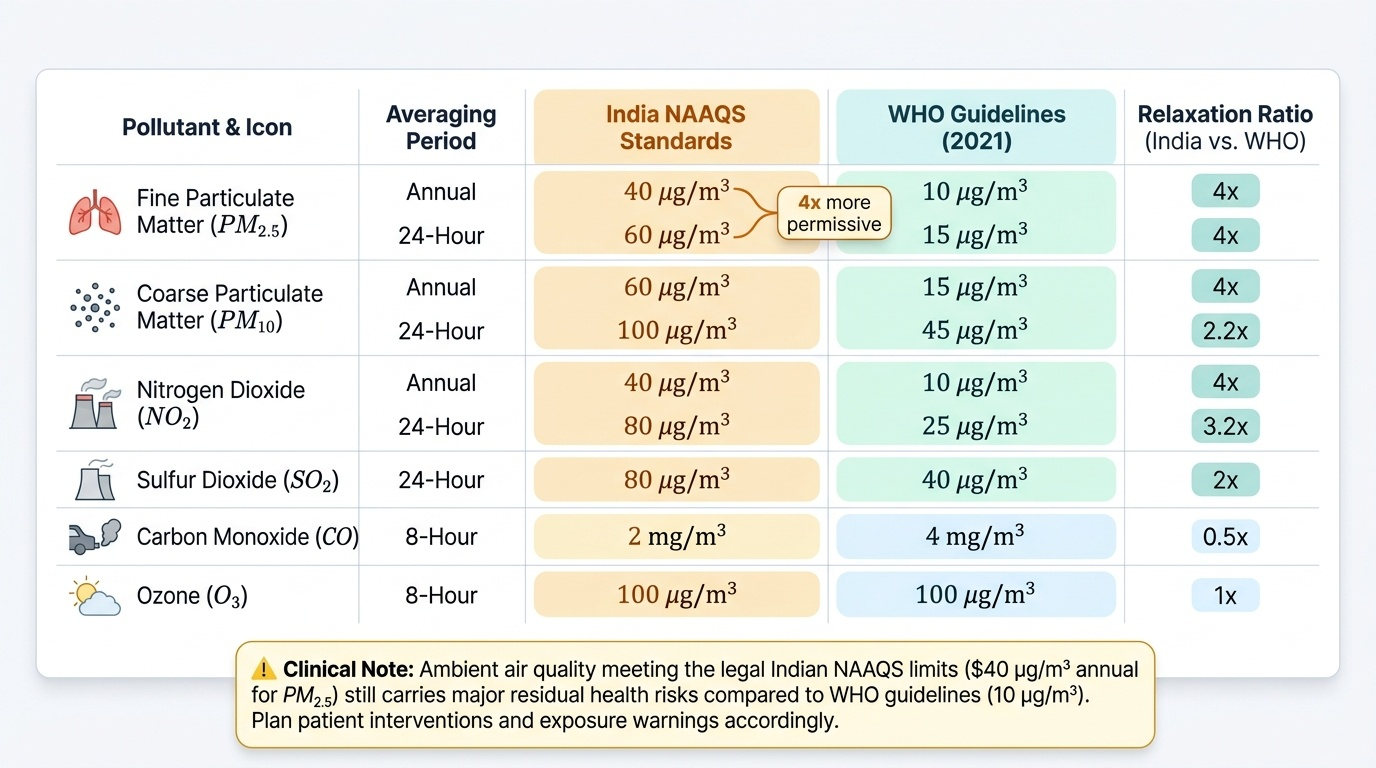
India regulates ambient air quality through the National Ambient Air Quality Standards (NAAQS), notified by the Ministry of Environment, Forest and Climate Change (MoEFCC) under the Air (Prevention and Control of Pollution) Act, 1981, and revised in 2009. NAAQS sets concentration limits for eight pollutants over two averaging periods (24-hour and annual). Key values relevant to this SDL are compared with WHO 2021 guidelines in the figure below.
Provided image
Note that India's NAAQS PM2.5 annual standard (40 µg/m³) is four times more permissive than the WHO 2021 guideline (10 µg/m³), reflecting feasibility considerations in a developing economy context. Understanding this gap is important when advising patients: even 'legal' ambient air quality in India carries residual health risk relative to WHO benchmarks.
For water quality, the Bureau of Indian Standards (BIS IS 10500:2012) specifies acceptable and permissible limits for drinking water. The Central Pollution Control Board (CPCB) administers water quality standards for surface and ground water under the Water (Prevention and Control of Pollution) Act, 1974.
For noise, the Environment (Protection) Amendment Rules 2000 establish day/night noise limits by zone. For occupational noise, the Factories Act 1948 (and the Noise Pollution Regulations) set the 85 dB(A)/8-hour limit. For radiation, the Atomic Energy (Radiation Protection) Rules 2004 set a 20 mSv/year effective dose limit for radiation workers and 1 mSv/year for the general public.
A critical national programme is the National Clean Air Programme (NCAP), launched in 2019, targeting a 20-30% reduction in PM2.5 and PM10 concentrations by 2024 in 122 non-attainment cities. The programme funds source apportionment studies, continuous ambient air quality monitoring stations (CAAQMS), and city-level action plans.
Monitoring, Surveillance, and Health Impact Assessment
Assessing the public health impact of environmental pollution requires integrating environmental monitoring data with health outcome surveillance. Ambient air quality monitoring in India is conducted through the CPCB's National Air Quality Monitoring Programme (NAMP) and the city-level CAAQMS (Continuous Ambient Air Quality Monitoring Stations) network. The AQI (Air Quality Index) translates pollutant concentrations into a 0-500 scale with six colour-coded categories (Good 0-50, Satisfactory 51-100, Moderate 101-200, Poor 201-300, Very Poor 301-400, Severe 401-500), making it a practical communication tool for clinicians advising high-risk patients.
Health impact assessment (HIA) uses epidemiological methods—cohort studies, time-series analyses, case-crossover designs—to quantify the fraction of disease attributable to a given pollutant concentration. The attributable fraction (or population attributable risk) estimates what proportion of cases would be prevented if exposure were reduced to a reference level. These analyses underpin the disease burden calculations (e.g. WHO Global Burden of Disease) that justify regulatory standards.
For lead surveillance, blood lead levels (BLL) are the gold standard biomarker. For arsenic, urinary arsenic speciation (inorganic arsenic + metabolites) reflects recent exposure; nail/hair arsenic reflects cumulative exposure. For fluoride, urinary fluoride and spot-check of water source fluoride concentrations guide programme responses.
Sentinel surveillance at the district level—where clinicians report clusters of potentially environment-linked illness (e.g. acute CO poisoning episodes in winter, clusters of methaemoglobinaemia in an agricultural village)—is a core physician responsibility under India's Integrated Disease Surveillance Programme (IDSP).
SELF-CHECK
In a village in West Bengal, several adults develop skin hyperpigmentation and palmoplantar keratoses over 10-15 years of using borewell water. Borewell water testing reveals arsenic at 65 µg/L. Which of the following best describes the regulatory context?
A. 65 µg/L is below both the WHO guideline (100 µg/L) and BIS standard, so no action is needed
B. 65 µg/L exceeds the WHO guideline of 10 µg/L but is within India's provisional standard of 50 µg/L, so the population is legally protected
C. 65 µg/L exceeds BOTH the WHO guideline (10 µg/L) and India's provisional standard (50 µg/L); the population is at risk and alternative safe water must be provided
D. 65 µg/L is only a concern for children, not adults with keratoses
Reveal Answer
Answer: C. 65 µg/L exceeds BOTH the WHO guideline (10 µg/L) and India's provisional standard (50 µg/L); the population is at risk and alternative safe water must be provided
The WHO guideline for arsenic in drinking water is 10 µg/L. India's provisional acceptable standard is 50 µg/L (used in endemic areas where safer sources are unavailable), with the recognising that the ideal standard is 10 µg/L. At 65 µg/L, the water exceeds even the provisional Indian limit, placing the population in a confirmed high-risk zone. The skin findings (hyperpigmentation + palmoplantar keratoses) are classic signs of chronic arsenicosis. Action is mandatory: alternate safe water sources must be identified and provided.