Page 6 of 19
CM3.2-3 | CM3.2-3 | Safe Water and Waterborne Disease — SDL Guide (Part 2)
Waterborne Diseases: Aetiology and Pathogenic Basis
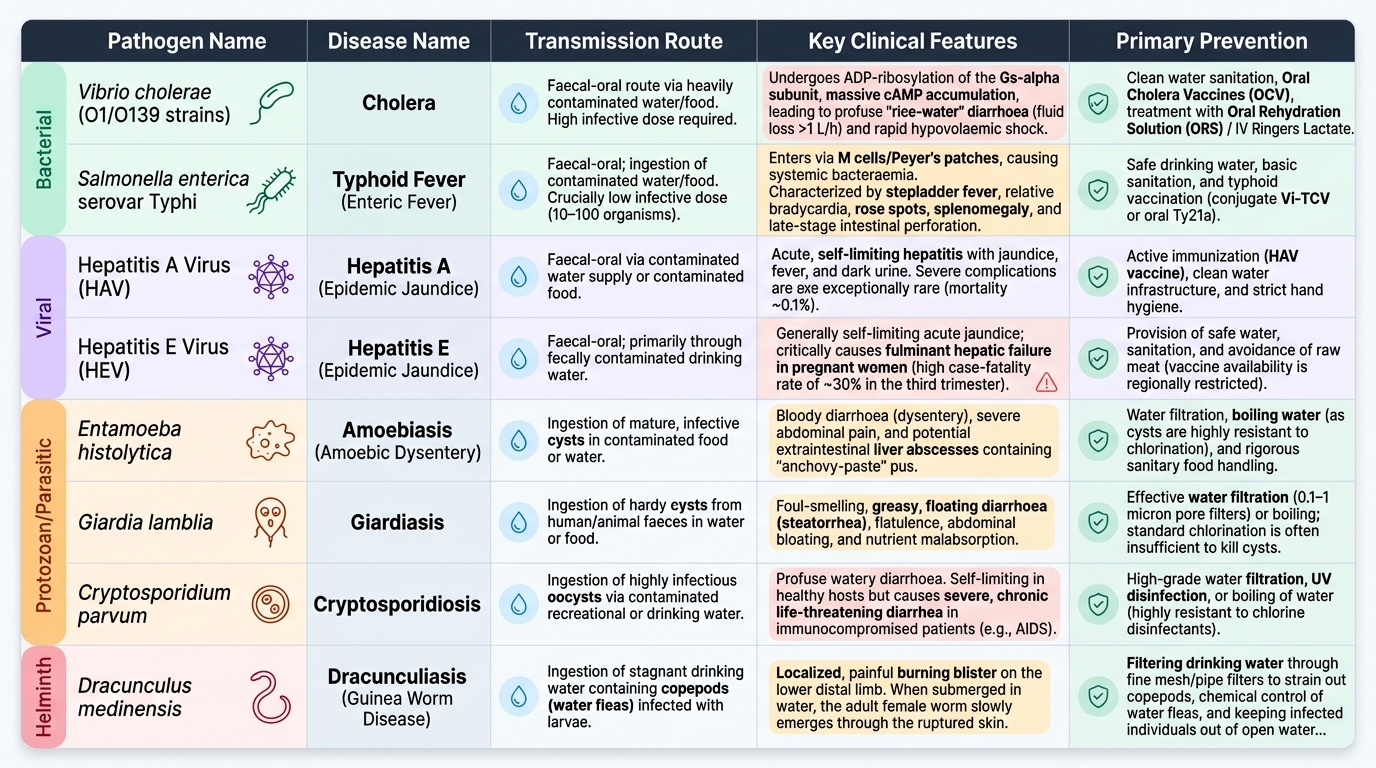
Waterborne diseases are transmitted via the faecal-oral route: human or animal faeces contaminate a water source; a susceptible host ingests a sufficient infective dose; the pathogen replicates in the GI tract or elsewhere and causes disease. The pathogen spectrum and key clinical/pathogenic features are summarised in the figure below.
Provided image
Cholera is caused by Vibrio cholerae O1 (El Tor biotype, responsible for the 7th pandemic) or O139. The organism colonises the small intestine and secretes cholera toxin (CT), a protein that ADP-ribosylates the Gs alpha subunit of adenylyl cyclase, locking it in the 'on' position. This causes massive cAMP accumulation in enterocytes, leading to active secretion of Cl⁻ into the gut lumen with passive water and Na⁺ following—producing the characteristic rice-water diarrhoea. The fluid loss can exceed 1 L/hour, causing life-threatening hypovolaemic shock within hours. Treatment is oral rehydration solution (ORS) or intravenous fluids (Ringer's lactate); doxycycline shortens the illness.
Typhoid (enteric fever) is caused by Salmonella enterica serovar Typhi. Unlike cholera, the infective dose is low (10–100 organisms). S. Typhi enters through M cells in the Peyer's patches, is taken up by macrophages, and causes a systemic bacteraemia. The clinical features include stepladder fever, relative bradycardia, rose spots, splenomegaly, and intestinal ulceration (Peyer's patch necrosis) in the third week that can lead to perforation or haemorrhage. The Widal test (serology) is widely used but has poor specificity; blood culture is the gold standard.
Hepatitis A (HAV) and Hepatitis E (HEV) are both RNA viruses causing waterborne epidemic jaundice. Critically: Hepatitis B and C are blood-borne and are NOT waterborne diseases. HAV causes a self-limiting hepatitis; severe complications are rare and mortality is <0.1%. HEV is typically also self-limiting but causes fulminant hepatic failure in pregnant women, with a case-fatality rate of ~30% in the third trimester—making it one of the most dangerous waterborne pathogens in India specifically. Large-scale HEV epidemics occur in India during and after monsoon flooding when sewage contaminates water supplies.
Amoebiasis is caused by Entamoeba histolytica. Cysts are ingested via contaminated water or food, excyst in the large intestine, and trophozoites invade the mucosa causing flask-shaped ulcers with bloody mucoid diarrhoea (amoebic dysentery). Trophozoites may enter the portal circulation and form amoebic liver abscess (the most common extra-intestinal complication in India). Treatment is metronidazole followed by diloxanide furoate to eliminate luminal cysts.
Dracunculiasis (guinea worm disease), caused by Dracunculus medinensis, is a helminthic waterborne disease acquired by drinking water containing infected Cyclops copepods. The worm migrates to subcutaneous tissues over 1 year; the female (up to 1 m long) then slowly emerges through a blister, classically at the lower limb. It is on the verge of global eradication—fewer than 15 cases were reported worldwide in 2023 (WHO)—making it one of public health's great success stories, achieved entirely through water safety (filtering drinking water through a fine-mesh cloth) and case containment.
Water Conservation and Rainwater Harvesting
Water conservation addresses the growing mismatch between freshwater demand and supply driven by population growth, climate change, and over-extraction of groundwater. The central principle is that the best water is the water you don't waste: conservation interventions range from household-level behavioural change (fixing leaks, greywater reuse for gardening, drip irrigation in agriculture) to watershed-scale management (afforestation to improve infiltration, regulation of groundwater extraction).
Rainwater harvesting (RWH) is the collection and storage of rainfall for direct use or groundwater recharge. Two main systems are used in India:
- Rooftop rainwater harvesting: rainwater from building rooftops is collected through gutters into first-flush diverters (which discard the initial contaminated run-off) and then into underground storage tanks or recharge pits. This system is particularly valuable in water-scarce urban and peri-urban areas and is now mandated in new buildings in many Indian states.
- Surface run-off harvesting: traditional water-harvesting structures—johads (Rajasthan), kunds, tanks, check dams, and percolation ponds—capture monsoon run-off at the watershed level, enabling both direct storage and aquifer recharge. The revival of traditional water-harvesting in Rajasthan (the 'johad movement' led by Rajendra Singh) restored water tables and river flow in drought-prone districts.
From a public health perspective, rainwater is generally of good bacteriological quality when collected from clean rooftops, but it must be stored in sealed tanks and treated (chlorinated or boiled) before drinking. Stagnant harvested water can become a mosquito breeding site if not managed properly—a water conservation intervention must not inadvertently create a vector breeding risk.
SELF-CHECK
A 28-year-old woman at 34 weeks gestation presents with 5-day history of jaundice, dark urine, and nausea. She has no prior liver disease. She lives in a flood-affected district where piped water supply was disrupted 3 weeks ago and the community used a shared open well. Rapid serology shows IgM anti-HEV positive. Which statement about her prognosis is MOST accurate?
A. Hepatitis E in pregnancy is self-limiting with the same benign course as in non-pregnant adults
B. She is at significantly higher risk of fulminant hepatic failure than the general population, with a case-fatality rate of approximately 30% in the third trimester
C. Hepatitis E in this context is likely a false positive as hepatitis viruses are not waterborne
D. Hepatitis E is dangerous only if she is also co-infected with hepatitis B
Reveal Answer
Answer: B. She is at significantly higher risk of fulminant hepatic failure than the general population, with a case-fatality rate of approximately 30% in the third trimester
Hepatitis E (HEV) is a recognised waterborne disease transmitted via the faecal-oral route, typically through contaminated water—exactly the scenario described (open well use after flood disruption). In the general population, HEV causes a self-limiting hepatitis. However, in pregnant women—especially in the second and third trimesters—HEV causes fulminant hepatic failure with a case-fatality rate of approximately 25-30%, making it one of the most dangerous waterborne pathogens encountered in Indian clinical practice. This patient requires urgent tertiary-level hepatology care. Note: Hepatitis B and C are blood-borne, not waterborne—an important distinction that the incorrect option tests.
Surveillance and Monitoring of Water Quality
Routine surveillance of drinking water quality ensures that standards are maintained between the treatment plant and the consumer. Monitoring operates at two levels: regulatory monitoring (by water utilities and state health departments) and epidemiological surveillance (by district health officers and IDSP units).
Bacteriological water testing uses two standard techniques:
- Most Probable Number (MPN) test (presumptive and confirmatory phases in lactose broth tubes): estimates the most likely number of coliforms per 100 mL; used for routine surveillance.
- Membrane filtration method: water is filtered through a 0.45-µm membrane; colonies of E. coli or total coliforms are counted after incubation. More precise and faster than MPN.
Residual chlorine testing using a DPD (N,N-diethyl-p-phenylenediamine) comparator is a simple field test performed at the tap to confirm that chlorination is adequate. Under Jal Jeevan Mission, ASHA workers and panchayat volunteers are trained to perform this test with BTB (brom thymol blue) or DPD field test kits.
Outbreak investigation for a waterborne disease cluster follows the standard epidemiological steps: (a) confirm the diagnosis; (b) establish case definitions; (c) describe the epidemic curve by time, place, person; (d) formulate and test a hypothesis about the water source; (e) implement control measures (boil-water advisory, emergency chlorination, source restriction); (f) evaluate the intervention. A point-source outbreak typically produces a sharp epidemic curve peaking within one incubation period—characteristic of a single contamination event (e.g. a one-time well contamination).
Under the Jal Jeevan Mission, every GP-level Water Quality Testing Laboratory tests water samples for physical, chemical, and bacteriological parameters. Community-based water quality testing has been expanded, with results uploaded to the JJM dashboard for district-level monitoring and action.
CLINICAL PEARL
Hepatitis E in pregnancy is a medical emergency. When you see a pregnant woman with jaundice in any Indian setting—especially during or after monsoon season, or after a water supply disruption—HEV must be at the top of your differential. Do not be falsely reassured by the fact that most hepatitis E in the general population is mild and self-limiting: the same virus kills one in three pregnant women who acquire it in the third trimester. Admit immediately, involve hepatology, and alert the district CMO—because a single pregnant woman with HEV almost certainly means a community-level water contamination event affecting others who are not yet symptomatic.
SELF-CHECK
In slow sand filtration, the most important mechanism by which bacterial and protozoal pathogens are removed is:
A. Mechanical sieving through fine sand particles that physically block all organisms larger than 0.45 µm
B. Chlorination added to the filter medium before filtration begins
C. The Schmutzdecke: a biological layer of bacteria and protozoa at the sand surface that degrades organic matter and eliminates pathogens through predation and metabolic activity
D. Gravity sedimentation of organisms heavier than water within the filter bed
Reveal Answer
Answer: C. The Schmutzdecke: a biological layer of bacteria and protozoa at the sand surface that degrades organic matter and eliminates pathogens through predation and metabolic activity
The Schmutzdecke (German: 'dirty layer') is the critical component of slow sand filtration. This biologically active layer forms spontaneously at the surface of a slow sand filter over 1-2 weeks of operation ('ripening') and consists of bacteria, algae, protozoa, and fungi that collectively create an ecosystem where pathogens are removed through predation, competition, and metabolic degradation. Efficiency reaches 99.99% for bacteria and 99.9% for Giardia cysts. Unlike rapid sand filtration (which is purely mechanical and requires coagulation pre-treatment), slow sand filtration is a biological process. Disruption of the Schmutzdecke (e.g. by backwashing too aggressively or running the filter dry) requires a new ripening period before effective pathogen removal resumes.