Page 4 of 21
CM7.2 | CM7.2 | Disease Transmission and Control Principles — SDL Guide
Learning Objectives
- Enumerate and describe the modes of transmission of communicable and non-communicable diseases (CM7.2)
- Describe the chain of infection and identify intervention points at each link
- Discuss measures for prevention and control of communicable and non-communicable diseases at each level of prevention
INSTRUCTIONS
How does a pathogen travel from one person to another — and how can that journey be interrupted? The chain of infection is the fundamental conceptual tool of communicable disease control, and understanding its links is what allows public health practitioners to choose the right intervention rather than the most visible one. This module builds that chain, classifies every transmission route with Indian examples, and shows how the same framework extends to non-communicable diseases through risk factor control.
References
- Park's Textbook of Preventive and Social Medicine, 27th edition — Chapter 2: Epidemiology; Chapter 5: Communicable Disease Control (textbook)
- Gordis L. Epidemiology, 5th edition — Chapter 2: The Dynamics of Disease Transmission (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 1906, typhoid fever struck 13 servants in a wealthy New York household. The family's cook — a woman named Mary Mallon — had worked in seven households over ten years; typhoid followed her to every one. Mary herself was perfectly healthy. Public health officials traced the outbreak to her, named her 'Typhoid Mary', and isolated her twice. She was an asymptomatic carrier: she harboured Salmonella Typhi in her gallbladder and shed it into food she prepared without washing her hands. She was not malicious; she simply did not understand how transmission worked. Understanding transmission — agent, reservoir, source, route, and host — is what converts a mysterious epidemic into a solvable public health problem.
WHY THIS MATTERS
India's disease burden is still disproportionately shaped by communicable diseases. Tuberculosis, diarrhoeal diseases, vector-borne diseases (malaria, dengue, chikungunya), vaccine-preventable diseases, and HIV together account for a substantial share of preventable mortality, especially in children under five. As a doctor, you will be the first point of contact for patients with these conditions and the first person in a position to interrupt transmission — through treatment (reducing source infectiousness), notification (triggering public health response), and counselling (modifying behaviour that perpetuates the chain). The transmission framework in this module is not an academic classification — it is the operational map that directs every control decision.
RECALL
From Year-1 microbiology, recall: (1) Bacteria replicate independently and can be killed by antibiotics; viruses require host-cell machinery and are controlled by antivirals and vaccines; parasites (protozoa, helminths) have complex life cycles often involving vectors or intermediate hosts. (2) Pathogenicity is the ability to cause disease; virulence quantifies severity; infectivity quantifies the ability to establish infection in an exposed host. (3) In pharmacology you learned about antimicrobial stewardship — prescribing antibiotics only when indicated. From the transmission perspective, appropriate treatment reduces the duration of infectiousness and thus breaks the chain at the source end.
How Disease Burdens Populations: Transmission as the Engine
Communicable diseases — those caused by biological agents capable of being transmitted from one host to another — remain a leading cause of morbidity and mortality globally and in India. The WHO estimates that infectious and parasitic diseases, respiratory infections, and diarrhoeal diseases together caused approximately 17 million deaths in 2019, with the vast majority in low- and middle-income countries. In India, tuberculosis alone kills approximately 500,000 people per year despite being curable; vaccine-preventable diseases like measles and pertussis persist where immunisation coverage is incomplete; cholera and typhoid recur wherever safe water and sanitation are unavailable. Understanding how these diseases spread — the mechanics of transmission — is the prerequisite for preventing them.
Non-communicable diseases (NCDs) — cardiovascular disease, diabetes, chronic obstructive pulmonary disease, cancers — are caused not by a single biological agent but by a web of modifiable risk factors (tobacco, unhealthy diet, physical inactivity, alcohol, air pollution). While the word 'transmission' is not conventionally applied to NCDs, many of their risk factors propagate through social networks, shared environments, and commercial systems in ways that are structurally analogous to transmission. The prevention framework — reducing exposure at the source, interrupting pathways, and increasing host resistance — applies to both disease categories, which is why a unified approach is conceptually powerful.
The chain of infection model provides the conceptual scaffold. Disease cannot occur without all links in the chain being intact; breaking any link prevents disease. Public health interventions are catalogued by which link they target — and choosing the most efficient link to break is the core of programme design.
Agent, Reservoir, Source, and Host: The Transmission Chain
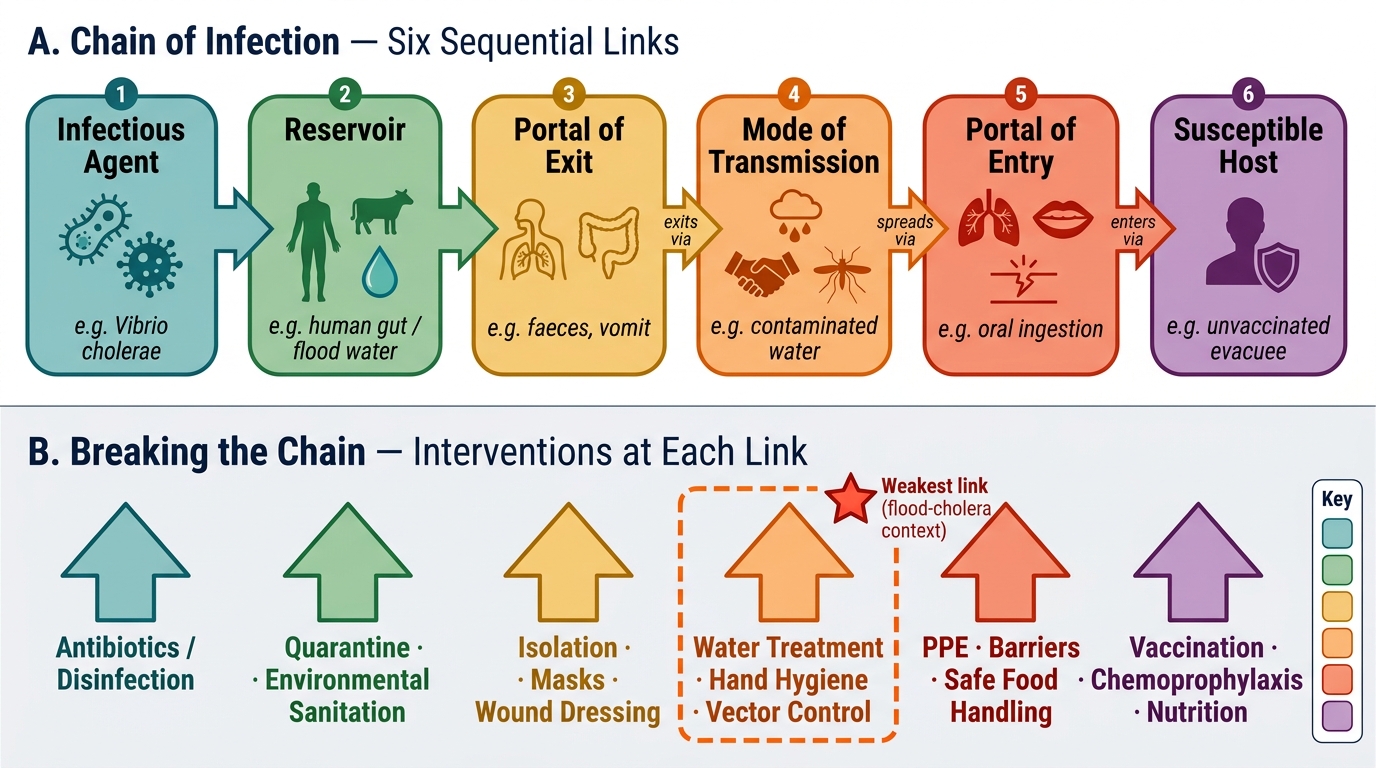
The chain of infection has six sequential links, and understanding each is prerequisite to understanding where to intervene.
The infectious agent (the pathogen) is characterised by four properties: (1) infectivity — how readily it establishes infection in an exposed host; (2) pathogenicity — the proportion of infected individuals who develop clinical disease; (3) virulence — the severity of disease in those who become ill; and (4) immunogenicity — the ability to induce a host immune response (relevant to vaccine design). Some agents survive prolonged periods outside hosts (spores of Clostridium); others survive only seconds (Neisseria gonorrhoeae).
The reservoir is the natural habitat in which the agent lives, multiplies, and from which it depends for survival — it may be human (typhoid, HIV), animal (zoonoses — plague = rats, rabies = dogs/bats, leptospirosis = rodents), or environmental (soil for tetanus/anthrax, water for Legionella). Distinguishing the reservoir from the source is clinically important: the source is the specific person, animal, or object from which infection is actually transmitted to a new host. For measles, the reservoir and source are the same (infected human); for salmonellosis, the reservoir is poultry but the source is contaminated food.
The portal of exit is how the agent leaves the reservoir: respiratory tract (influenza, TB, measles — via respiratory secretions), gastrointestinal tract (cholera, typhoid — via faeces), skin/mucous membranes (varicella, syphilis), blood (HIV, hepatitis B — via blood/sexual fluids), or transplacental/perinatal.
The mode of transmission (covered in detail in the next section) carries the agent from source to host.
The portal of entry is how the agent enters the new host: respiratory tract (inhalation of droplet nuclei), gastrointestinal tract (ingestion), skin (wound inoculation, arthropod bite), mucous membranes (sexually transmitted infections).
The susceptible host is determined by immunity status (natural infection, vaccination), age (extremes of age are more susceptible), nutritional status, genetic factors, and co-morbidities (immunosuppression).
Chain of Infection and Intervention Strategies
The conceptual power of this model is that it is a checklist: for every communicable disease, you can map out each link and ask — which is the weakest (most interruptible) link in this chain in the current context? For cholera in a flood situation, the answer is almost always the mode of transmission (water safety) rather than the reservoir (human cases are abundant) or host susceptibility (vaccination coverage may be low in the emergency population).
SELF-CHECK
Mary cooks food in multiple households and transmits typhoid fever while remaining healthy herself. Which term describes Mary's role in the transmission chain?
A. Index case
B. Reservoir
C. Asymptomatic carrier
D. Susceptible host
Reveal Answer
Answer: C. Asymptomatic carrier
Mary is an asymptomatic (healthy) carrier — a person who harbours and can transmit the pathogen without showing clinical disease. The reservoir for Salmonella Typhi is the human gut (and gallbladder in chronic carriers); Mary is simultaneously the reservoir, source, and portal of exit. An index case is the first identified case in an outbreak; a susceptible host is one who can acquire infection.
Modes of Transmission: Direct and Indirect Routes
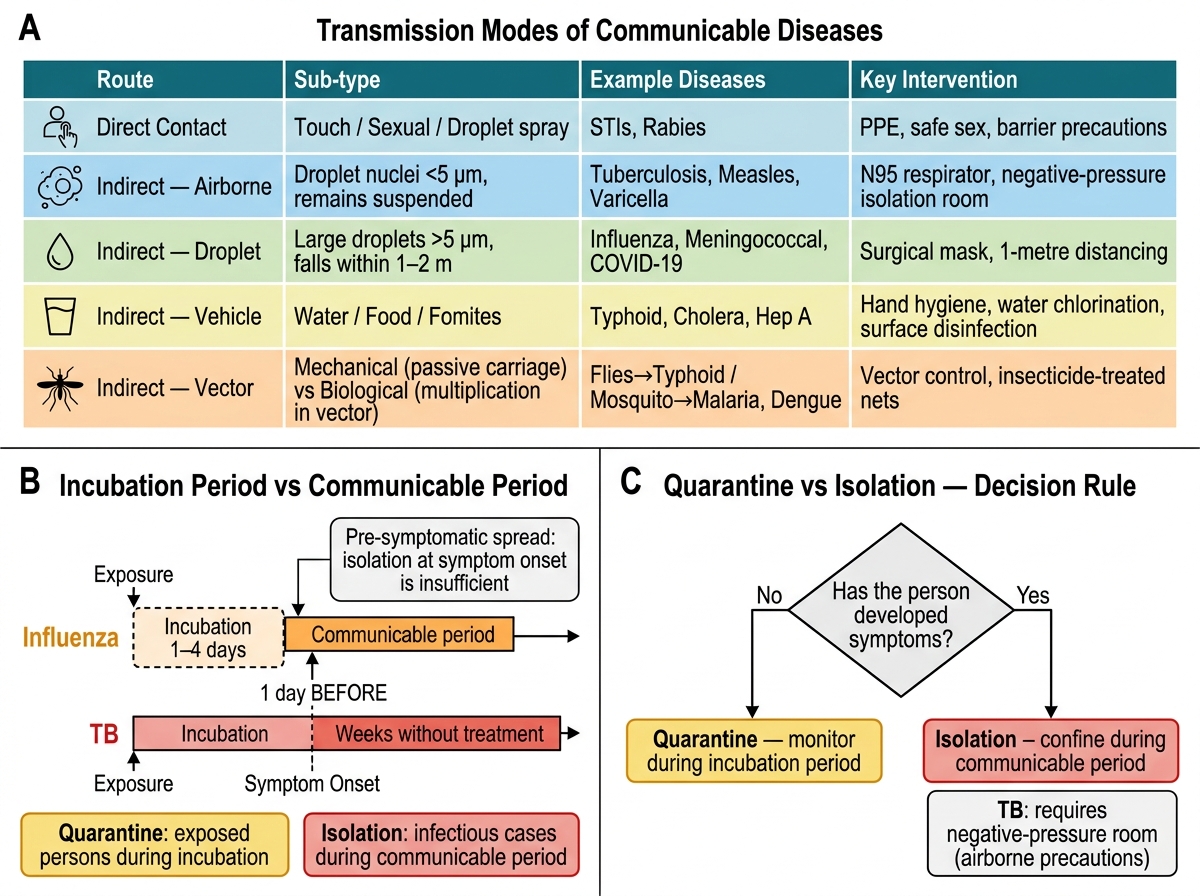
Modes of transmission are classified into direct and indirect categories. The distinction matters because control strategies differ fundamentally: direct transmission requires interrupting close contact; indirect transmission requires addressing the vehicle or vector.
Direct transmission requires close physical proximity or contact between source and host:
- Direct contact transmission: skin-to-skin (impetigo, scabies), mucous membrane contact (sexually transmitted infections — gonorrhoea, syphilis, HIV via sexual intercourse)
- Droplet transmission: large respiratory droplets (>5 µm) expelled during coughing, sneezing, or speaking; travel ≤1–2 metres and settle quickly; examples: influenza, COVID-19 (close-range), meningococcal meningitis
- Vertical (perinatal) transmission: from mother to child transplacentally (congenital rubella, congenital CMV, congenital syphilis, HIV), during delivery (hepatitis B, HIV, HSV-2), or postnatally via breast milk (HIV, CMV)
Indirect transmission involves an intermediate vehicle or living vector:
- Vehicle-borne transmission: a contaminated inanimate substance carries the agent. Water-borne: cholera, typhoid, hepatitis A, polio. Food-borne: salmonellosis, staphylococcal food poisoning. Fomite-borne: contaminated objects (conjunctivitis via towels, hepatitis B via shared needles).
- Vector-borne transmission: a living intermediate (usually an arthropod) carries the agent.
- Mechanical vector: passive carriage without replication — houseflies transmitting enteric pathogens on their body parts or legs
- Biological vector: the agent replicates or undergoes a developmental stage in the vector — Anopheles mosquito for malaria (sporogony occurs in the vector), Aedes aegypti for dengue (viral replication), sandfly for kala-azar
- Airborne transmission: very small particles (<5 µm) called droplet nuclei remain suspended in air for prolonged periods and travel distances >1 metre; examples: tuberculosis (droplet nuclei of M. tuberculosis can remain airborne for hours in poorly ventilated spaces), measles, varicella. Dust particles from dried soil can also carry Coccidioides spores.
Classification of Transmission Modes, Epidemiological Periods, and Control Measures
Incubation period (time from exposure to first symptoms) must be distinguished from communicable period (interval during which the source can transmit). For influenza, the communicable period begins 1 day BEFORE symptom onset (pre-symptomatic transmission), which is why isolation at symptom onset is insufficient to fully prevent spread. For TB, communicable period may last weeks without treatment. This distinction directly informs quarantine (applies to exposed persons during the incubation period) versus isolation (applies to infectious cases during the communicable period) decisions.
SELF-CHECK
Tuberculosis spreads via droplet nuclei that remain suspended in air for prolonged periods. This classifies TB transmission as:
A. Direct droplet transmission
B. Fomite-borne indirect transmission
C. Airborne indirect transmission
D. Mechanical vector-borne transmission
Reveal Answer
Answer: C. Airborne indirect transmission
TB spreads via droplet nuclei — particles <5 µm that remain airborne for hours in enclosed spaces. This is airborne transmission, classified as indirect (the air acts as the vehicle). Direct droplet transmission involves large droplets (>5 µm) that fall within 1–2 metres. Fomites are inanimate objects. Mechanical vectors carry pathogens passively on their bodies. The practical implication: TB control requires negative-pressure isolation rooms and N95 masks, not just surgical masks.