Page 2 of 8
CM19.1-4 | CM19.1-4 | Essential Medicine List, Primary Care Requirements and Counterfeit Prevention — SDL Guide (Part 2)
Counterfeit, Substandard and Falsified Medicines: Definitions and Prevention
Poor-quality medicines are a major public health crisis that directly undermines the essential medicines framework. WHO distinguishes three distinct categories that are often incorrectly grouped under the single term 'counterfeit.' Understanding the distinction matters because the prevention and regulatory response differs for each.
Substandard medicines (also called 'out-of-specification' products) are authorised medicines — approved by the national regulatory authority — that fail to meet their quality standards or specifications. Substandard medicines have the correct active pharmaceutical ingredient (API) but at the wrong concentration, with wrong dissolution properties, or with degradation products from improper storage. Common causes include poor manufacturing practices (non-GMP), improper storage conditions in the supply chain (heat, humidity), or improper handling. Substandard medicines are a quality failure, not necessarily a deliberate fraud.
Unregistered/unlicensed medicines are medicines that have not undergone evaluation and/or approval by the relevant national or regional regulatory authority for the market in which they are distributed. These may have acceptable quality but have not been assessed for safety and efficacy in the regulatory process.
Falsified medicines are medicines that deliberately or fraudulently misrepresent their identity, composition, or source. A falsified medicine may have the correct packaging, the correct labelling, and appear identical to the genuine product — but contain no active ingredient, a wrong ingredient, the correct ingredient at wrong dose, or dangerous contaminants. Falsification is a deliberate criminal act. Notable falsified medicine events include: falsified artesunate in Southeast Asia (2001–2010) responsible for thousands of malaria deaths; falsified insulin in sub-Saharan Africa; falsified COVID-19 vaccines during the pandemic.
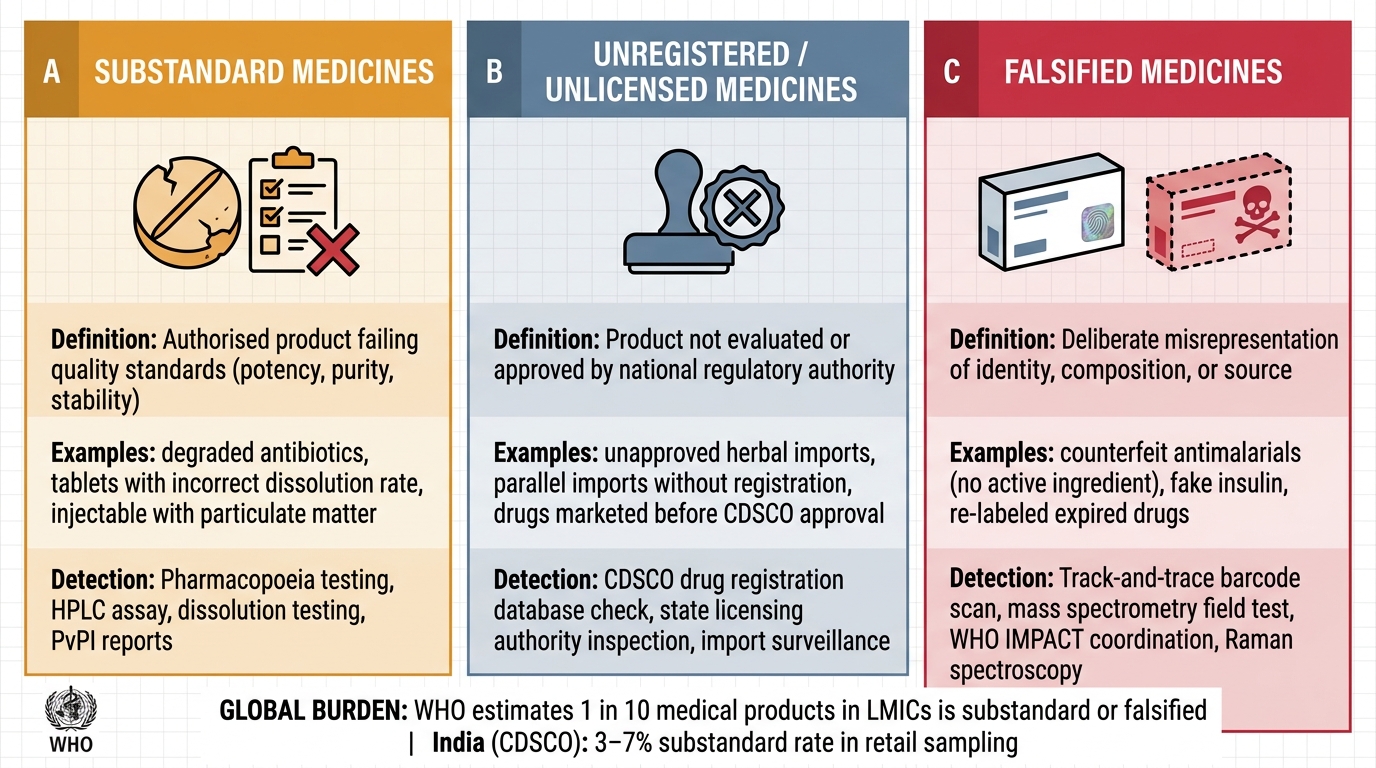
WHO Classification of Substandard, Unregistered, and Falsified Medicines
The global burden is alarming: WHO estimates that 1 in 10 medical products in LMICs is substandard or falsified. In India, CDSCO surveys have found substandard drug rates of 3–7% in random sampling of retail pharmacy stocks, with higher rates in remote areas and unlicensed outlets.
Prevention mechanisms in India:
- CDSCO (Central Drugs Standard Control Organisation): India's national regulatory authority under the DGHS, Ministry of Health. CDSCO approves new drugs, licences manufacturers, conducts post-market surveillance, and coordinates with State Licensing Authorities (SLAs) for manufacturing and retail inspection.
- Pharmacovigilance Programme of India (PvPI): operated by CDSCO and the Indian Pharmacopoeia Commission (IPC), collects adverse drug reaction reports and signals that can indicate substandard or falsified products.
- Track-and-trace systems: CDSCO has mandated barcoding and track-and-trace for scheduled drugs to enable authentication throughout the supply chain from manufacturer to patient.
- WHO IMPACT (International Medical Products Anti-Counterfeiting Taskforce): established 2006, a multi-stakeholder platform coordinating international enforcement, regulatory cooperation, and awareness. India participates through CDSCO.
- Facility-level detection: a PHC medical officer or pharmacist should inspect incoming drug consignments for packaging integrity, correct labelling, manufacturing and expiry dates, batch numbers, and consistency of tablet/capsule appearance. Colour, size, or embossing irregularities warrant rejection and reporting to the State Licensing Authority.
SELF-CHECK
A PHC pharmacist finds a batch of amoxicillin capsules that were manufactured by a licensed company but contain only 60% of the stated 500 mg dose due to a manufacturing error. How should this be classified under WHO's 2017 terminology?
A. Falsified medicine
B. Unregistered medicine
C. Substandard medicine
D. Unlicensed medicine
Reveal Answer
Answer: C. Substandard medicine
A medicine from a licensed, authorised manufacturer that fails to meet its quality specification (in this case, 60% of stated dose rather than the required ≥90–110%) is classified as a substandard medicine under WHO's 2017 terminology. It is not falsified (no deliberate misrepresentation) and not unregistered (the manufacturer is licensed). Substandard products result from quality failures in manufacturing or storage, not criminal fraud.
Evaluating Essential Medicines Programmes: Availability, Affordability, and Rational Use Indicators
Measuring the performance of an essential medicines programme requires standardised indicators that go beyond medicine lists and procurement data. WHO and Health Action International (HAI) developed a standard methodology — the WHO/HAI survey methodology — for measuring medicine availability and affordability at the facility and patient level. This methodology is used by national governments, researchers, and international agencies to generate comparable data across countries and over time.
Availability indicators measure the percentage of a basket of essential tracer medicines that are actually present at facilities on the day of survey. A tracer medicine list typically includes 14–30 essential medicines drawn from the national EML, spanning acute conditions (antibiotics, antimalarials, ORS), chronic conditions (antihypertensives, antidiabetics), and child health (vaccines, micronutrients). The WHO/HAI benchmark is ≥80% availability of tracer medicines as a target for functioning essential medicines programmes. India's national surveys consistently find availability well below this threshold in public facilities, particularly at peripheral levels.
Affordability indicators measure the number of days of wages for the lowest-paid government worker required to purchase a standard course of treatment. An antibiotic course costing more than one day of wages is considered unaffordable by WHO/HAI definition. When measured in this way, many essential medicines in Indian private pharmacies are unaffordable for the poorest quintile — which is the direct justification for government generic pharmacy schemes (Jan Aushadhi) and price regulation through DPCO.
Rational use indicators measure prescribing and dispensing behaviour against evidence-based standards. WHO's core prescribing indicators include: (1) average number of medicines per encounter (WHO benchmark ≤2); (2) percentage of encounters with an antibiotic prescribed (WHO benchmark 20–26%); (3) percentage with injectable prescribed (WHO benchmark 10–17%); (4) percentage of medicines prescribed from EML or formulary (benchmark 100%); (5) percentage of medicines actually dispensed (benchmark 100%). Indian PHC studies consistently show prescription rates above WHO benchmarks for antibiotics (40–60%) and injectables (25–35%), indicating systematic irrational prescribing.
NLEM performance in India: The inclusion of a medicine in NLEM 2022 and the consequent DPCO price ceiling measurably increases affordability. Studies comparing prices before and after NLEM inclusion show price reductions of 30–60% for generic equivalents. However, NLEM listing does not automatically guarantee availability — procurement, supply chain, and storage remain separate failure points that must be monitored independently.
CLINICAL PEARL
A common examination and practical trap: the WHO EML and India's NLEM are frequently confused with prescription-only medicine lists or banned drug lists — they are neither. NLEM inclusion means: (1) the medicine is recommended as a first-choice agent for the relevant indication in India's health system; (2) its price is regulated by DPCO through NPPA; (3) it should be available at the appropriate level of care. A medicine NOT on NLEM can still be legally prescribed and dispensed — the list is a selection and prioritisation tool, not a prohibition. Conversely, NLEM listing does NOT mean a medicine is available at your PHC — that depends on state procurement and supply chain efficiency. Always check your facility's actual stock against the theoretical NLEM.
Applying the Essential Medicines Framework in Clinical Practice
The operational application of the essential medicines framework for a PHC medical officer spans three daily activities: prescribing from the formulary, calculating and ordering drug requirements, and detecting and reporting substandard or falsified medicines.
Prescribing from the formulary: When prescribing, prefer NLEM/state formulary medicines as first-line agents. Use generic names (not brand names) — this is both legally mandated for government prescriptions and essential for interoperability with the drug store. When a formulary medicine is unavailable, document the substitution and report the stock-out to the supply chain officer — this generates the demand signal needed for restocking. Apply the P-drug principle: for your most common ten diagnoses, know which medicine you will prescribe first, why, and what the alternatives are.
Calculating medicine requirements at the PHC level follows a standard method:
1. Morbidity method: estimate number of episodes for each disease in the catchment area per quarter (population × incidence rate); multiply by the standard treatment protocol quantity per episode; add a 25% safety stock buffer.
2. Consumption method: take actual consumption in the previous period (e.g., 3 months) and adjust for any supply interruptions; project forward with a 25% buffer.
For example, a PHC serving a population of 10,000 with a 3% annual incidence of uncomplicated UTI (300 episodes/year = 75/quarter) would require approximately 75 × 14 tablets (ciprofloxacin 500 mg BD × 7 days = 14 tablets/episode) = 1,050 tablets per quarter, plus 25% safety stock = approximately 1,313 tablets. The calculation is then submitted to the block or district medical store for procurement.
| Step | Morbidity Method | Consumption Method |
|---|---|---|
| Data source | Population + incidence + treatment protocol | Actual previous consumption records |
| Best when | Starting a new facility or for new conditions | Facility has reliable stock records |
| Buffer | Add 25% safety stock | Add 25% safety stock |
| Limitation | Requires accurate morbidity data | Perpetuates historical irrational use if present |
Detecting substandard and falsified medicines at the facility level is a gatekeeping function. On receipt of consignments, inspect: packaging integrity (no tears, moisture damage), correct labelling (generic name, dose, batch number, manufacturing date, expiry date, manufacturer name and licence number), visual consistency of tablets/capsules (uniform colour, embossing, size, no crumbling), and correct cold chain documentation for temperature-sensitive products. Report suspected substandard or falsified medicines to the State Drug Controller through the prescribed adverse drug reaction reporting format and CDSCO's online reporting portal. Suspected medicines should be quarantined — not administered — pending investigation.
Jan Aushadhi Kendras are government generic medicine stores that stock NLEM and other generic medicines at prices 50–90% below branded equivalents. As a community physician, knowing the location of the nearest Jan Aushadhi Kendra and directing patients there when government stock is unavailable is an access intervention within your daily practice.
SELF-CHECK
A PHC serves a population of 5,000 people. The annual incidence of acute respiratory infections requiring a 5-day amoxicillin course (250 mg TDS = 15 tablets/episode) is 10% of the population. Using the morbidity method with a 25% safety stock buffer, how many amoxicillin 250 mg tablets are required per quarter?
A. 938 tablets
B. 1,172 tablets
C. 4,688 tablets
D. 2,344 tablets
Reveal Answer
Answer: D. 2,344 tablets
Using the morbidity method: Annual episodes = 5,000 × 10% = 500 episodes/year ÷ 4 = 125 episodes/quarter. Tablets per quarter = 125 × 15 = 1,875 tablets. Safety stock buffer = 1,875 × 25% = 469 tablets. Total requirement = 1,875 + 469 = 2,344 tablets. Option D (2,344) is correct. Option A (938) would be roughly a quarter of the base requirement without buffer — a common error of using annual episodes directly without converting to quarterly. Option C (4,688) is approximately twice the correct answer — a doubling error.