Page 5 of 25
CM1.3-5 | CM1.3-5 | Determinants and Natural History of Disease — SDL Guide
Learning Objectives
- Describe the characteristics of agent, host, and environmental factors in health and disease
- Explain the multifactorial aetiology of disease using the epidemiological triad and web of causation
- Describe the stages of the natural history of disease from prepathogenesis to outcome
- Define the four levels of prevention (primordial, primary, secondary, tertiary) and their sub-modes
- Map preventive interventions to their corresponding stage of the natural history of disease
INSTRUCTIONS
This module provides the conceptual backbone of epidemiology and public health practice. The epidemiological triad explains WHY disease occurs — through the interaction of agent, host, and environment. The natural history of disease explains HOW disease evolves once initiated. The levels of prevention framework answers WHEN and HOW public health can intervene. These three frameworks recur in every subsequent Community Medicine topic — from tuberculosis control to cardiovascular disease prevention. Understand them deeply here; they are not memorisation tasks but reasoning tools.
References
- Park's Textbook of Preventive and Social Medicine, 26th edition — Ch 2 (Disease Causation) and Ch 3 (Natural History and Levels of Prevention) (textbook)
- Leavell HR, Clark EG. Preventive Medicine for the Doctor in His Community, 3rd ed. 1965 — original classification of levels of prevention (source)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old male labourer in a brick kiln develops progressive cough and weight loss. The chest X-ray shows a cavitating lesion in the right upper lobe. Mycobacterium tuberculosis is identified on sputum smear. Question: why this man? He was exposed to the same environment as a hundred co-workers — most of whom did not develop TB. The answer lies not in a single cause but in a convergence: a highly infectious organism (agent), a host with silica-damaged lungs and borderline malnutrition (host), working in an enclosed, poorly ventilated space with others who are likely TB cases (environment). This is the epidemiological triad — and understanding it is the beginning of understanding how disease is caused, prevented, and controlled.
WHY THIS MATTERS
India accounts for approximately one-quarter of the global tuberculosis burden — a statistic that defies explanation by biology alone. The epidemiological triad explains why: the pathogen is necessary but not sufficient. Host vulnerability (malnutrition, diabetes, HIV co-infection) and environmental conditions (crowding, poor ventilation, poverty) are equally decisive. Every doctor working in the Indian health system will encounter diseases whose causation is multifactorial — and every national health programme is designed around understanding and interrupting these causal chains. This module gives you the conceptual tools to reason about disease causation and prevention across all of Community Medicine.
RECALL
In your basic science years, you studied the pathophysiology of infectious diseases — how bacteria evade host immunity, how viruses replicate, how the body mounts a defence. You also encountered in Microbiology the concept that pathogenicity involves both the microorganism's properties and the host's immune status. Now extend that thinking: in Community Medicine, the 'host' is not only immunological — it includes behavioural, demographic, and genetic characteristics — and the 'environment' is not only physical but social and economic. Keep in mind the homeostasis model: disease = imbalance; and the community is a system in which balance can be restored by acting on any part of the triad.
Disease as a Population Burden — Why Causation Matters
Disease in a population is rarely the result of a single, sufficient cause. The germ theory of disease — one pathogen, one disease — was a revolutionary advance in 19th-century medicine, but it is an incomplete model for understanding why disease rates vary dramatically between populations exposed to the same pathogen, or why non-communicable diseases occur in people with no identifiable pathogen. Modern epidemiology replaced the single-cause model with the concept of multifactorial aetiology: disease arises from the simultaneous or sequential interaction of multiple causal factors, no single one of which is invariably necessary or sufficient.
Brian MacMahon introduced the concept of the web of causation to visualise this multiplicity: disease is the downstream outcome of an interconnected web of biological, behavioural, environmental, and social factors, each connected to others by probabilistic relationships. Disrupting any strand in the web can reduce disease risk — which is the theoretical basis for public health interventions that target risk factors rather than pathogens directly. For example, lung cancer risk is reduced not only by removing cigarette smoke (the proximate carcinogen) but also by poverty reduction (which reduces smoking prevalence), education (which improves health literacy), and clean indoor air standards (which reduce co-exposures).
Understanding multifactorial aetiology is clinically liberating: it means that disease prevention does not require eliminating every possible cause — it requires identifying the most actionable causal factors and reducing their contribution. This is the intellectual foundation for risk-factor epidemiology and for all national prevention programmes.
The Epidemiological Triad — Agent, Host, and Environment
The epidemiological triad (also called the epidemiological triangle) is the classical framework for conceptualising disease causation in terms of three interacting elements: the agent, the host, and the environment. Disease results when the balance among these three is disrupted — specifically when the agent overwhelms the host's defences within a permissive environment. The triad is particularly useful for communicable diseases but has been adapted for non-communicable conditions as well (e.g. the 'agent' in coronary artery disease includes lipid particles and inflammatory mediators; the 'environment' includes diet and physical activity context).
Agent factors are the proximate causes of disease — the necessary (though not always sufficient) biological, chemical, physical, or nutritional stimuli:
- Biological agents: bacteria (Mycobacterium tuberculosis), viruses (dengue, HIV), parasites (Plasmodium vivax), fungi (Candida), prions
- Chemical agents: toxins (arsenic, lead), industrial chemicals, pesticides, drugs in overdose, carcinogens
- Physical agents: ionising radiation, ultraviolet radiation, extremes of heat or cold, mechanical trauma, noise
- Nutritional agents: deficiencies (iodine, iron, vitamin A, D) or excesses (saturated fats, sodium, excess calories)
Host factors determine susceptibility and resistance — the biological and behavioural characteristics of the individual or population:
- Genetic constitution: sickle-cell trait protects against falciparum malaria; BRCA mutations increase breast cancer risk
- Age and sex: children are more susceptible to vaccine-preventable diseases; men have higher CVD risk in middle age
- Immunity: prior infection, vaccination status, nutritional immune competence
- Nutritional status: malnutrition is the most powerful host susceptibility factor for infectious disease in children
- Occupation, habits, and behaviour: a healthcare worker has high TB exposure risk; a smoker has elevated lung cancer risk
Environmental factors are the external conditions that determine the agent's survival, transmission, and the host's exposure:
- Physical environment: geography (altitude, climate), housing (crowding, ventilation), water and sanitation quality
- Biological environment: reservoirs (rodents for plague, cattle for brucellosis), vectors (Anopheles for malaria, Aedes for dengue), vehicles (contaminated food/water)
- Socioeconomic environment: poverty, education, social support, occupational hazards, access to health care
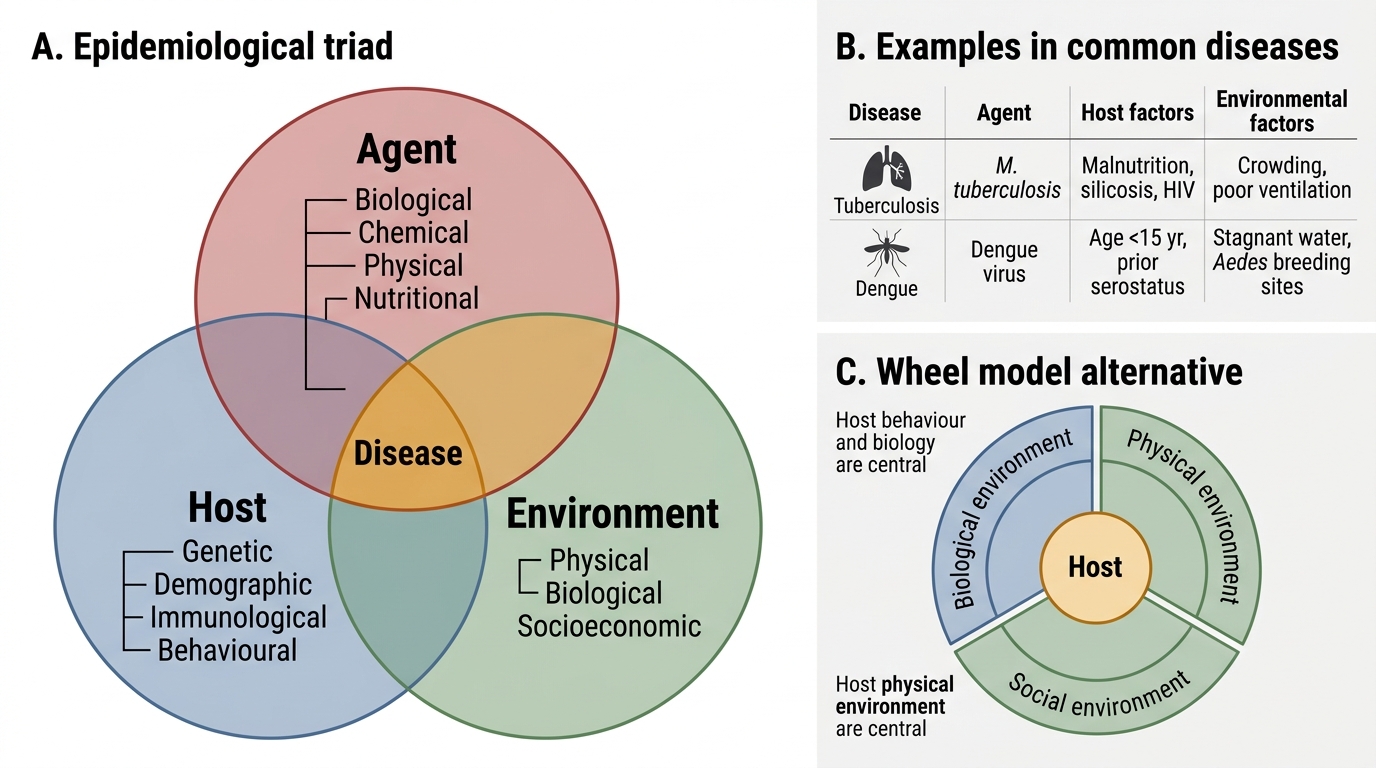
Epidemiological Triad and Wheel Model
| Category | Agent | Host | Environment |
|---|---|---|---|
| Types | Biological, chemical, physical, nutritional | Genetic, demographic, immunological, behavioural | Physical, biological, socioeconomic |
| TB example | M. tuberculosis (biological) | Malnutrition, silicosis, HIV (immune) | Crowding, poor ventilation (physical) |
| Dengue example | Dengue virus (biological) | Age <15 yr, prior infection serostatus | Stagnant water, Aedes breeding sites |
The wheel model (an alternative to the triad) places the host at the centre surrounded by biological, physical, and social environments, emphasising the centrality of human behaviour and biology. Both models are acceptable for NMC purposes; the triad is more commonly tested.
SELF-CHECK
In a study of a TB outbreak in a slum, most residents were exposed to the index case but only 15% developed disease. Which factor BEST explains why 85% remained unaffected despite exposure?
A. The agent (M. tuberculosis) was low-virulence in this outbreak
B. Environmental factors (ventilation) prevented transmission to all
C. Host factors (immunity, nutritional status, genetics) determined differential susceptibility
D. The web of causation concept states that no single factor causes disease
Reveal Answer
Answer: C. Host factors (immunity, nutritional status, genetics) determined differential susceptibility
When the same agent in the same environment causes disease in some but not others, host factors — especially immune competence, nutritional status, prior sensitisation, and genetic susceptibility — are the primary explanation for differential outcomes. The multifactorial model assigns the 'why this person?' question to host factors when agent and environment are held relatively constant.
Natural History of Disease — From Prepathogenesis to Outcome
The natural history of disease describes the complete, uninterrupted course of a disease as it would evolve in the absence of any treatment or preventive intervention — from the earliest ecological interaction between the agent and host through to the final outcome of recovery, disability, or death. Understanding the natural history is foundational to prevention planning: each stage of the natural history corresponds to a specific preventive opportunity.
The natural history has two main periods:
1. Stage of Prepathogenesis (Pre-pathogenesis Period): The agent, host, and environment interact, but no pathological change has yet occurred in the host. The ecological conditions for disease are ripening: the agent is present in the environment, the host is exposed and susceptible, environmental conditions are favourable for transmission or exposure. The host is not yet 'ill' by any biological criterion, but the balance has shifted and disease initiation is plausible. This stage is the target for primordial and primary prevention — interventions that act BEFORE the disease process begins.
2. Period of Pathogenesis: Once the agent or causal stimulus has entered or begun acting upon the host, the pathological process is initiated. This period has sub-stages:
- Early pathogenesis (sub-clinical phase): Pathological changes are underway but the host is asymptomatic and undiagnosed. The host may still be capable of spreading infectious disease (carrier state). This is the population represented by the 'below-waterline' portion of the iceberg phenomenon — the submerged mass of unrecognised disease that is vastly larger than the visible clinical tip.
- Advanced pathogenesis (clinical phase): Signs and symptoms appear; the patient presents to health services. Clinical and tissue diagnosis becomes possible.
- Outcome: The disease resolves into one of three states: (a) complete recovery, (b) disability (physical, mental, or social) — permanent or temporary, or (c) death.
The iceberg phenomenon, introduced to epidemiology by Gordon (1952), is critical for understanding the true community burden of a disease. For many infections — tuberculosis, dengue, poliomyelitis, COVID-19 — the number of sub-clinical or minimally symptomatic cases vastly exceeds the number reaching a diagnosis. Surveillance based only on clinical cases therefore grossly underestimates the true disease burden and may mislead programme design.