Page 17 of 25
CM1.9-10 | CM1.9-10 | Communication in Doctor-Patient Relationships — SDL Guide
Learning Objectives
- Explain the importance of effective communication skills in health and doctor-patient relationships
- Describe the consequences of poor communication — non-adherence, diagnostic error, patient dissatisfaction
- Describe the four models of doctor-patient relationship (Emanuel & Emanuel)
- Apply verbal communication skills: open and closed questions, plain language, avoiding jargon
- Demonstrate active listening and empathy in clinical encounters
- Describe the Calgary-Cambridge structured consultation framework
- Explain the principles of breaking bad news (SPIKES) and motivational interviewing
- Demonstrate communication skills in a simulated clinical environment
INSTRUCTIONS
Communication is not a soft skill — it is a clinical tool, as important as any diagnostic test. Research shows that effective communication independently improves patient outcomes: patients who understand their condition are more adherent, have fewer complications, and are more satisfied. This module prepares you for both the theoretical framework and the simulated practice of clinical communication — skills that will be assessed in your OSCE examinations and exercised every day of your clinical career.
References
- Park's Textbook of Preventive and Social Medicine, 26th edition — Ch on Doctor-Patient Communication (textbook)
- Silverman J, Kurtz S, Draper J. Skills for Communicating with Patients, 3rd ed. Radcliffe, 2013 — Calgary-Cambridge framework (textbook)
- Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA. 1992;267(16):2221-6 (source)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2018, the Consumer Forum in a major Indian city awarded compensation to a patient's family after a court found that the doctor had failed to adequately explain the risks of a surgical procedure before obtaining consent. No clinical error had occurred — the surgery was technically competent — but the patient had not understood what she was consenting to, and the doctor's notes contained no evidence of an explanation having been given. The legal and ethical issue was communication failure, not clinical failure. This case is not exceptional: in India, communication failures are among the most common causes of patient complaints, consumer forum cases against doctors, and loss of therapeutic trust — and they are entirely preventable with the skills taught in this module.
WHY THIS MATTERS
Every subsequent clinical posting — medicine, surgery, obstetrics, paediatrics, psychiatry — will require you to communicate effectively with patients and their families. The NMC CBME curriculum has specifically included communication competencies (CM1.9 and CM1.10) because research consistently shows that technical clinical skill without communication competence produces worse patient outcomes: patients who do not understand their diagnosis are less adherent, return to hospital more frequently, and have poorer quality of life. Communication is assessable, teachable, and improvable with practice — and this module provides the theoretical foundation for the simulated and clinical practice that follows.
RECALL
You have already encountered interpersonal health communication in the context of IEC and BCC (CM1.6) — where the doctor's individual consultation was described as a personalised behaviour change communication event. Recall the Health Belief Model: a patient's likelihood of adhering to treatment depends on their perceived susceptibility, perceived benefit, perceived barriers, and self-efficacy — all of which are shaped primarily by how the clinician communicates. As you read this module, connect each communication skill to the BCC principle it operationalises: active listening addresses perceived barriers; empathy addresses emotional state; teach-back addresses self-efficacy; motivational interviewing addresses stage of change.
The Burden of Poor Communication — Non-Adherence, Harm, and Inequity
The consequences of poor communication in health care are measurable, serious, and far-reaching. Non-adherence to prescribed medications and treatment plans is the most direct outcome: multiple systematic reviews show that patients who report poor communication with their doctor are two to three times more likely to be non-adherent to long-term therapy. In diseases requiring sustained treatment — tuberculosis, diabetes, hypertension, epilepsy — non-adherence directly causes treatment failure, disease progression, and preventable complications. In TB specifically, treatment non-adherence is a primary driver of drug resistance, which has major public health consequences well beyond the individual patient.
Diagnostic error is the second major consequence: a doctor who does not listen to or appropriately question the patient may miss crucial elements of the history, leading to misdiagnosis. Studies of closed malpractice claims consistently identify communication breakdown — particularly failure to take a complete history, failure to explain findings, and failure to listen to patient concerns — as a leading contributor to diagnostic error. In India, where resource constraints limit access to expensive investigation, the clinical history is even more central to diagnosis than in high-income settings; communication is therefore proportionally more critical to diagnostic accuracy.
Patient dissatisfaction, complaint, and medico-legal risk are downstream consequences of persistent poor communication. The Consumer Protection Act (2019, superseding the 1986 Act) is applicable to medical services in India, and patient complaints to consumer courts frequently cite failure to explain diagnosis, treatment options, and risks — i.e., communication failures rather than technical errors alone. The Medical Council of India (now NMC) Code of Medical Ethics explicitly requires that doctors communicate clearly and honestly with patients and obtain informed consent through genuine explanation, not merely a signature.
Health inequity is the third dimension: patients with low literacy, poor language concordance with the clinician, or marginalised social positions receive systematically worse communication quality in clinical encounters — they ask fewer questions, are less likely to have their questions answered, and leave with less understanding of their health status and treatment plan. Effective communication is thus an equity tool as well as a clinical one.
Determinants of Effective Communication — What Shapes the Doctor-Patient Relationship
Communication quality in clinical encounters is shaped by factors from three domains: the doctor, the patient, and the relationship model that structures their interaction.
Doctor factors: Training and skill in communication are the most modifiable doctor-side determinants. Additional factors include time pressure (short consultations constrain communication), fatigue and burnout (impair empathy and active listening), attitudes (paternalistic vs patient-centred orientation), and language proficiency relative to the patient's language.
Patient factors: Literacy, language, and cultural background powerfully shape communication: a low-literate patient may not understand medical jargon; a patient from a different linguistic background may not disclose symptoms in the absence of an interpreter; cultural norms around authority may prevent patients from questioning the doctor even when they do not understand the advice. Emotional state also matters — a patient who is anxious or afraid will have reduced information processing capacity.
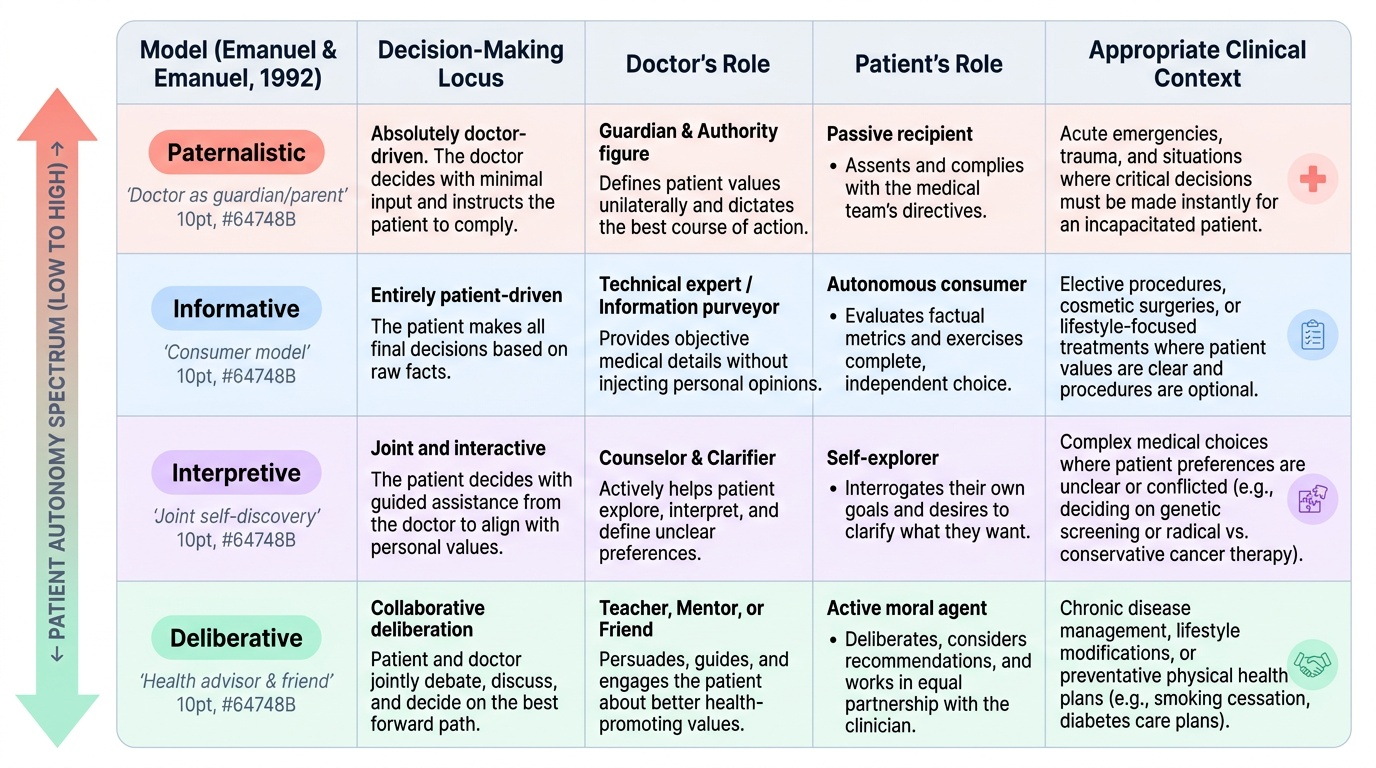
Models of the doctor-patient relationship: Emanuel and Emanuel (1992) described four models that range along a spectrum of patient autonomy:
- Paternalistic model: The doctor acts in the patient's best interest as the doctor defines it — makes the decision and instructs the patient to comply. Appropriate in acute emergencies where the patient is incapacitated. Generally considered ethically inadequate when the patient is competent and can participate in decisions.
- Informative model: The doctor provides complete factual information; the patient makes all decisions based on their own values. Also called the 'consumer model.' Appropriate for elective decisions about lifestyle or optional procedures. Weakness: leaves the patient without guidance when they want the doctor's view.
- Interpretive model: The doctor helps the patient clarify their own values and then uses those values to guide a joint decision. More interactive than informative — requires genuine exploration of patient preferences.
- Deliberative model: The doctor acts as a health advisor and friend — not only presenting options but engaging the patient in deliberation about which option best serves their health and long-term values. Most demanding in terms of time and communication skill; considered the gold standard for complex, high-stakes decisions.
Provided image
Environmental factors: Privacy, physical setting, absence of interruptions, seating position (at the same level as the patient rather than behind a desk creates a more egalitarian encounter), and time allocation all shape communication quality. In Indian public sector facilities, these environmental factors are frequently suboptimal — but a skilled communicator can partially compensate through mindful technique even in challenging settings.
SELF-CHECK
A patient with newly diagnosed type 2 diabetes presents for her first visit. The doctor explains her condition, outlines three management options (lifestyle alone, metformin alone, lifestyle + metformin), and helps her explore which option aligns best with her lifestyle values and personal priorities, ultimately making a joint decision. This most closely exemplifies which model of doctor-patient relationship?
A. Paternalistic
B. Informative
C. Interpretive
D. Deliberative
Reveal Answer
Answer: C. Interpretive
The doctor is helping the patient clarify her own values and preferences — 'which option aligns best with your lifestyle values' — and using those values to guide a joint decision. This is the interpretive model (Emanuel & Emanuel). The deliberative model would go further: the doctor would actively advocate for the option that best serves the patient's long-term health values, not just reflect them back. Informative would present options and leave all choice to the patient without guidance.
Verbal and Non-Verbal Communication Skills
The clinical consultation relies on both verbal and non-verbal channels of communication, and skilled clinicians manage both simultaneously. Verbal communication refers to the content and structure of spoken language; non-verbal communication refers to everything else — tone of voice, body language, facial expression, physical proximity, and gesture.
Verbal communication principles:
- Open questions cannot be answered with yes/no; they invite the patient to tell their story in their own words. Examples: 'What brings you in today?', 'Tell me more about the pain,' 'How has this been affecting your daily life?' Open questions are used at the beginning of the history to gather breadth and understand the patient's perspective before narrowing to specific details.
- Closed questions are answered with yes/no or a specific fact: 'Is the pain worse at night?', 'Do you smoke?', 'How many tablets did you take?' Closed questions are used to clarify specific details and complete the systematic review.
- Jargon avoidance: Using medical terminology without checking comprehension creates a barrier. 'Your liver enzymes are elevated and we're concerned about hepatocellular damage' communicates very little to a patient without medical knowledge. 'Your blood tests show that your liver is not working as well as it should' is comprehensible and actionable.
- Chunking and checking: Providing large amounts of information at once overwhelms patients; effective communicators give information in small 'chunks' and check comprehension between each.
Non-verbal communication:
- Eye contact: Appropriate eye contact conveys interest, respect, and engagement; avoidance (e.g. looking at the computer screen throughout the consultation) signals disinterest.
- Posture and body language: Open posture (uncrossed arms, leaning forward slightly) signals attention and empathy; closed posture signals disengagement.
- Proxemics: The physical distance between doctor and patient carries cultural meaning. In India, the appropriate distance varies by relationship and cultural context; clinical sensitivity to patient discomfort with proximity is important.
- Tone of voice: The emotional content of communication is carried disproportionately by tone (how something is said) rather than words (what is said). A technically correct explanation delivered in a brusque, dismissive tone communicates disrespect and undermines therapeutic alliance.
| Question type | Definition | Example | When to use |
|---|---|---|---|
| Open | Cannot be answered yes/no; invites narrative | 'Tell me what brings you in today' | Beginning of history; understanding the patient's perspective |
| Closed | Yes/no or specific fact answer | 'Do you have any chest pain at night?' | Clarifying details; systematic review |